
Abstract
Amid the coronavirus disease 2019 (COVID-19) pandemic, there is an unprecedented increase in public avoidance of hospitals predominantly driven by fear of contracting the virus. Recent publications highlight a re-emergence of rare post–myocardial infarction complications. While mechanical complications are infrequent in the era of primary percutaneous coronary intervention, they are associated with high mortality rates. The concurrent occurrence of mechanical complications such as left ventricular aneurysm and ventricular septal rupture is an extremely rare entity. We hereby delineate a unique case of a 53-year-old Caucasian male who underwent successful concomitant closure of a ventricular septal rupture, left ventricular aneurysmectomy, and 3-vessel coronary artery bypass grafting. Due to a delayed initial presentation owing to the patient’s fear of contracting COVID-19, the surgery was carried out 3 months after the myocardial infarction. His postoperative evaluation confirmed normal contractility of the left ventricle and complete closure of the ventricular septal rupture. Six months postoperatively, the patient continues to do well. We also present a literature review of the mechanical complications following delayed presentation of myocardial infarction amid the COVID-19 pandemic. This article illustrates that clinicians should remain cognizant of these extremely rare but potentially lethal collateral effects during the ongoing global public-health challenge. Furthermore, it highlights a significant concern regarding the delay in first medical contact due to the reluctance of patients to visit the hospital during the COVID-19 pandemic.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has become a major global health challenge of this century with more than 183 million confirmed cases and over 3.97 million deaths to date. It has affected health care systems throughout the world even in the wake of recent advents such as the COVID-19 vaccine, thereby necessitating radical changes in therapeutic protocols. Consequently, the initial management of time-sensitive cardiovascular emergencies such as ST-elevation myocardial infarction (STEMI) has been limited to fibrinolytic therapy in some hospitals, often delaying the necessary percutaneous coronary intervention (PCI). 1 One study from the United States showed an estimated 38% decrease in STEMI activations during the early phase of the pandemic. 2 Similarly, a 40% decline was observed in STEMI interventions in Spain. 3 Global lockdowns, social distancing guidelines, and awareness campaigns to limit the spread of COVID-19 have resulted in a decline in timely myocardial infarction (MI) presentations worldwide. Several studies posit that the public fear of acquiring COVID-19 in the hospital might indeed be responsible for this exorbitant decline.2-4
It is notable that the incidence of serious post–MI mechanical complications has decreased remarkably over the past few decades due to early reperfusion using primary PCI. In this context, the re-emergence of once-grave but now antiquated entities such as mechanical complications after MI during COVID-19 pandemic is perplexing.5,6 The resurgence of mechanical complications can be attributed, in part, to delayed MI presentations resulting in a delay in revascularization. We chronicle here the case of a STEMI patient who reportedly avoided making first medical contact for over 3 months owing to his fear of contracting COVID-19 in the hospital. After a significantly delayed presentation, his workup confirmed the simultaneous presence of a left ventricular aneurysm (LVA) and a Becker type III ventricular septal rupture (VSR) complicating his STEMI. In addition, we undertake a systematic literature review of mechanical complications associated with delayed MI presentation amid the COVID-19 pandemic. This article highlights the need for improved public awareness and education to seek early medical care for emergent cardiovascular conditions.
Illustrative Case
Presentation
A 53-year-old obese Caucasian man presented to our medical center with a 3-month history of worsening shortness of breath and lower extremity edema. The patient described associated diaphoresis but denied any chest pain or dizziness. He did not seek medical attention early due to his apprehensions surrounding COVID-19. He denied alcohol intake or illicit drug dependence. He was not on therapy with any medications, denied recent hospitalization, and had not seen his primary care doctor in the last 10 years. At presentation, he was afebrile and hemodynamically stable.
Investigations
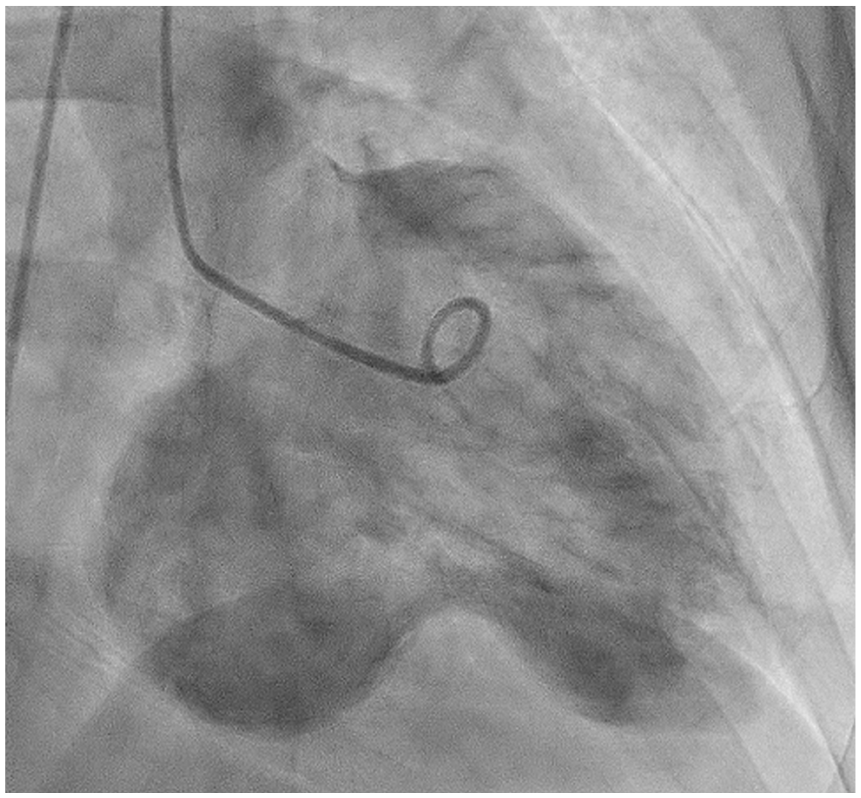
The patient underwent extensive diagnostic workup (Table 1). Electrocardiogram demonstrated ST-segment elevations in the inferior leads (Figure 1). He then underwent emergent coronary angiography, which divulged severe multi-vessel coronary artery disease, with complete occlusion of mid-right coronary artery (Figure 2; Supplementary Videos 1 and 2, available online). Left ventriculography revealed inferior wall hypokinesis of left ventricle with basilar inferior segment aneurysm and mural thrombus (Figure 3; Supplementary Video 3, available online). It also showed possible left-to-right shunt via an interventricular septum. The procedure was halted without PCI and the patient was admitted to coronary care unit for cardiothoracic surgery consultation. Transthoracic echocardiography showed mildly reduced biventricular function (left ventricular ejection fraction: 40% to 45%), with a basal inferior wall aneurysm and small VSR with left-to-right shunt (Supplementary Videos 4 and 5, available online). Cardiac magnetic resonance imaging was recommended by cardiothoracic surgery. It showed a wide-mouthed aneurysm in the base of the inferior wall, measuring 5.2 × 5.3 × 4.4 cm with an associated mural thrombus (Figure 4). There was a small-sized VSR in the inferior and basal aspect of interventricular septum, causing left-to-right shunt (Qp/Qs: 1.7; Table 2). Transmural delayed enhancement, involving mid and basal inferior septum, was suggestive of nonviable myocardium (Figure 5). No evidence of mitral regurgitation was present. Coronavirus testing via nasopharyngeal swab was negative.
Patient Laboratory Values on Admission and During Hospitalization.


Twelve-lead electrocardiography at presentation. A 12-lead electrocardiogram shows ST elevation in inferior leads (II, III, AVF) with reciprocal ST depressions in lateral leads (I, AVL, V4-V6).

Angiography of right coronary artery (RCA) in left anterior oblique projection. It demonstrates complete occlusion of the mid vessel with the reconstitution of distal RCA from right to right collaterals.
Left ventriculogram. Left ventriculogram in anterior oblique (RAO) projection demonstrating an inferobasal wall true aneurysm.
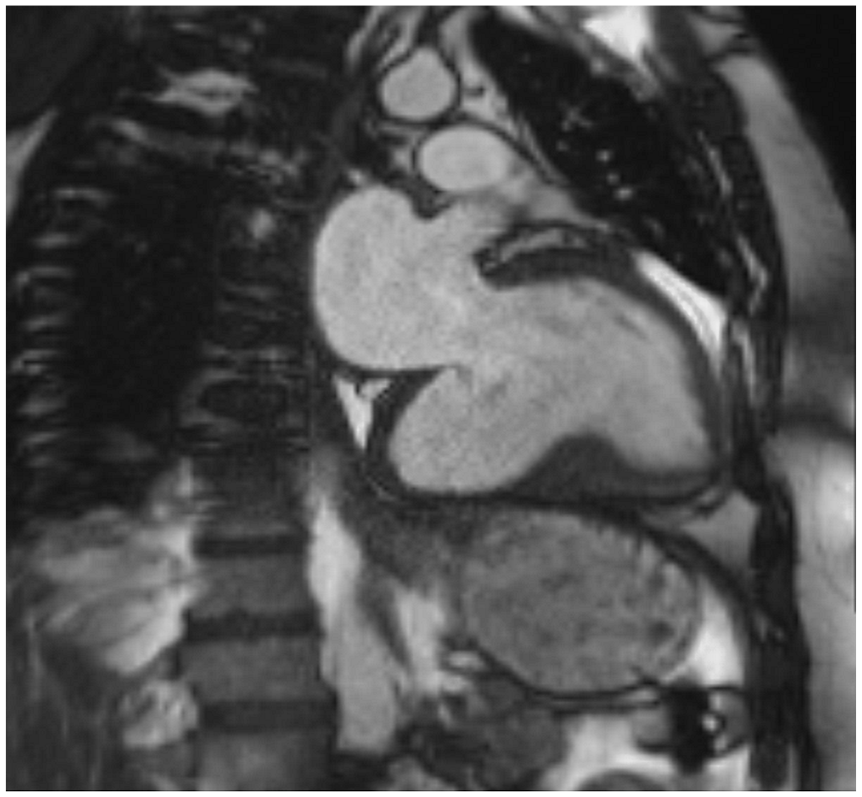
Cardiac magnetic resonance (CMR) imaging. CMR imaging in sagittal view (2-chamber view) demonstrating left ventricular true aneurysm.
Right Heart Catheterization Measurements.


Cardiac magnetic resonance (CMR) imaging. Short-axis view of heart on CMR imaging showing ventricular septal rupture at inferobasal left ventricle.
Management
After multidisciplinary team discussion, cardiothoracic surgery planned curative resection. The patient remained hemodynamically stable and was started on heparin infusion. He underwent an uneventful removal of mural thrombus, aneurysmectomy, and VSR patch repair. The step-wise approach to the aneurysmectomy procedure is outlined in the flowchart (Figure 6). Furthermore, he also underwent 3-vessel coronary artery bypass grafting (CABG) for his multivessel disease. He tolerated the procedures well.

The step-wise approach to the aneurysmectomy procedure. LVA, left ventricular aneurysm; PP, polypropylene; IVMS, interrupted vertical mattress sutures; IMS, interrupted mattress sutures.
Clinical Outcome and Follow-up
His hospital course was uncomplicated. After 5 days of postoperative monitoring, he was discharged from the hospital in a stable condition. At the 6-month follow-up, he did not report any chest pain or shortness of breath, and his surgical wounds appeared well-healed. The patient continues to do well to date.
Methods
In order to study trends of mechanical complications following delayed presentation of acute MI amid COVID-19 pandemic, we conducted a systematic search of medical databases, including MEDLINE (PubMed and Ovid), Embase, Scopus, and Cochrane. Furthermore, we reviewed conference papers from major cardiology scientific meetings. A comprehensive search strategy was constructed in order to identify relevant articles, using a combination of keywords. Search terminologies such as “mechanical complications,” “acute myocardial infarction,” “STEMI,” and “delayed presentation” were combined using the Boolean operators “AND” and “OR” with the terms “COVID-19,” “SARS-CoV-2,” “Coronavirus,” and “pandemic,” with all associated permutations. English-only articles were considered, without an application of a defined time filter. Two of the authors independently reviewed the titles and abstracts of the articles obtained from the initial search. For the eligibility of each study, full-text versions of potentially relevant articles were independently retrieved and reviewed by the other 2 authors. Concerns regarding the eligibility of individual studies were resolved after joint reassessment and consensus. The final inclusion of an article into quantitative analysis was based on a discussion headed by the senior author. The descriptive data are presented as mean ± standard deviation, range, or percentage, as applicable.
Results
Initial database search yielded a total of 217 articles. A vast majority of articles were excluded as they were redundant (n = 102), duplicate (n = 28), reported pre-COVID-19 results (n = 19), did not describe individual patient data (n = 16), or the language was other than English (n = 12). A total of 40 studies were accessed in the full-version form in order to determine eligibility. It resulted in the further exclusion of irrelevant studies (n = 19). Finally, a total of 21 articles were identified to be pertinent with regard to the scope of this study and were included in the final quantitative analysis.
Mechanical complications following delayed MI presentations were described in a total of 26 case reports only (level of clinical evidence: IV) in 21 selected articles included in this study, dating from June 2020 to May 2021.7-27 No gender predominance was noted as the male-to-female ratio was 1:1). The age of patients ranged from 37 to 87 years (mean ± standard deviation = 64.12 ± 53.70 years). Notably, 24 (92%) of 26 patients were over 50 years of age. This observation may facilitate enhanced suspicion of mechanical complications in elderly patients (50 years and over) admitting with delayed MI presentations. In terms of the temporal relationship between the MI occurrence and onset of aforementioned complications, 20 (77%) of 26 patients developed symptoms within the first week after MI. Chest pain 18 (69%), dyspnea 13 (50%), and lightheadedness 4 (15%) were among the frequently encountered clinical presentations. On cardiac catheterization, a variety of underlying coronary artery lesions were identified. With regard to the detection of post-MI mechanical complications, transthoracic echocardiography was usually the first investigation employed to identify the type, location, and subsequent hemodynamic sequelae. These patients may require prompt hemodynamic stabilization, which may necessitate a combination of medical therapy and mechanical circulatory support such as intra-aortic balloon pump 5 (19%), extracorporeal membrane oxygenation 2 (8%), and Impella 5.0 support 1 (4%). Surgery was performed in 17 (63%) patients. However, the optimal timing for surgical intervention remains to be determined in this setting. Notably, percutaneous therapeutic approaches were applied in 7 (27%) patients, denoting them as an emerging alternative treatment option for patients at prohibitive surgical risk. Of 26 patients for whom clinical outcomes were reported, a total of 8 (31%) patients died, whereas 2 (8%) patients remained under critical care. Notably, 16 (62%) patients recovered from these serious complications. The data regarding patient demographics, presenting symptoms, time from symptom onset to presentation, electrocardiographic features, anatomic findings, nature of mechanical complications, left ventricular ejection fraction, treatment, and clinical outcomes are summarized (Table 3).7-27
Literature Review of Mechanical Complications After Delayed Presentations of Acute MI During COVID-19 Pandemic.

Abbreviations: CABG, coronary artery bypass grafting; CAD, coronary artery disease; CHF, chronic heart failure; COVID-19, coronavirus disease 2019; CPR, cardiopulmonary resuscitation; DES, drug-eluting stent; ECMO, extracorporeal membrane oxygenation; ER, emergency room; IABP, intra-aortic balloon pump; ICU, intensive care unit; LAD, left anterior descending; LCA, left coronary artery; LCx, left circumflex; LHC, left heart catheterization; LV, left ventricular; LVA, left ventricular aneurysm; LVEF, left ventricular ejection fraction; MI, myocardial infarction; MR, mitral regurgitation; PCI, percutaneous coronary intervention; RCA, right coronary artery; STEMI, ST-elevation myocardial infarction; TIMI, thrombolysis in myocardial infarction; VSD; ventricular septal defect; VSR, ventricular septal rupture.
Discussion
Acute STEMI is an established cause of significant mortality worldwide. Early detection followed by urgent management using PCI is effective in achieving optimal clinical outcomes. 28 In recent times, the COVID-19 pandemic has overwhelmed health care systems categorically, often masking the presence of other serious medical emergencies, including cardiac pathologies. 29 As per the data from several European nations, 25% to 40% decreased STEMI admissions were noted amid the pandemic.3,30,31 A similar trend has also been noted in the United States.32-34 An international study performed by the European Society of Cardiology demonstrated a significant reduction of >40% in the gross number of STEMI admissions. 35 Furthermore, a study from Hong Kong revealed an increase in the total time elapsed before the presentation of STEMI from 82.5 to 318 minutes due to excessive wariness surrounding the pandemic. 36 Imperatively, a dilatory presentation of MI may result in grave mechanical complications that were once considered extremely rare. 37 The present patient had no other deterrents to seeking medical attention, except for his fear of contracting COVID-19 from the hospital.
LVA is an established complication in patients with massive MI who have a delayed presentation. Currently, the incidence of this complication has been significantly decreased. As per the analysis of the National Inpatient Sample from 2000 to 2017, LVA complicated 0.2% of 11 622 528 admissions for acute MI. 38 It may pose a diagnostic challenge, particularly in its differentiation from a pseudoaneurysm. 39 Multimodality cardiac imaging is frequently required for accurate detection, which also helps in selection of the appropriate treatment. 38 After a significantly delayed presentation due to COVID-19, this patient’s workup also included cardiac magnetic resonance imaging that not only confirmed the LVA but also helped in the assessment of the myocardial viability. In patients with small-to-moderate size asymptomatic LVAs, medical therapy can be considered with an estimated 5-year survival of up to 90%. 40 The medical therapy should target afterload reduction using an angiotensin-converting enzyme inhibitor and anticoagulation in cases with a thrombus within the aneurysmal sac or left ventricle or if there is a remarkable left ventricular dysfunction. Surgical intervention such as aneurysmectomy in conjunction with CABG, as in this case, can be performed in LVA patients with ventricular arrhythmic and/or pump function failure refractory to medical and minimally invasive treatments. 41
VSR is also a serious post-MI complication, with a mortality rate bordering 50%. It has become exceedingly rare in the current era of PCI, with an incidence ranging from 0.17% to 0.31% following STEMI.42,43 This patient had a Becker type III VSR, which is predominantly caused by late presentation of acute MI and is not commonly attributed to reperfusion damage. This type of VSR lesions frequently occurs in the subacute phase, 3 to 5 days following acute MI. 43 In this patient, the exact timing of the VSR lesion could not be ascertained due to his significantly delayed initial presentation. Most of these lesions, as evidenced by the present case, occur after RCA infarction. VSRs are an established cause of left-to-right shunting, leading to pressure and volume overload in the right ventricle. Transthoracic echocardiography plays a vital role in detection, measurement of dimensions, and impact of the VSR as well as exclusion of probable etiologies. Furthermore, left ventriculography can aid in confirming the presence of VSR in cases with unexplained hemodynamic instability while undergoing primary PCI. On pulmonary artery catheterization, the Qp/Qs can be calculated using right ventricular step-up oxygen saturation. 43 In terms of management, surgical patch repair is the treatment of choice. 43 This patient showed excellent recovery after surgical intervention.
The present case is rare and unique in multiple ways. It has several pertinent clinical implications. First, aneurysms in the inferoposterior wall are uncommon. Second, VSR after MI rarely occurs in the inferior and basal portion of the interventricular septum. Third, the concurrent presence of a true LVA and VSR is an extremely rare clinicopathologic entity that can be particularly serious. Fourth, our patient presented a rare case of post-MI mechanical complications with chronic heart failure symptoms such as worsening shortness of breath and lower extremity edema. Fifth, this case demonstrates the clinical effectiveness of CABG, removal of mural thrombus, aneurysmectomy, and VSR patch repair for a favorable outcome despite late presentation. Sixth, it highlights the fear of patients to contract COVID-19 from hospitals that has led to reduction in hospitalization rates due to MI, resulting in re-emergence of life-threatening mechanical complications.
As indicated by the results of the literature review, severe post-MI mechanical complications are being reported across the globe now. With regard to the public awareness of these mechanical complications, several international organizations, such as the American Heart Association, the European Society of Cardiology, and a number of independent clinicians, have written opinion pieces in print media.44-47 Similarly, individual patient experiences regarding contracting severe mechanical complications after acute MI continue to be broadcasted.48,49 Due to the ongoing situation, it is exceedingly important to start mass information campaigns.50-53 All possible barriers in making first medical contact in MI patients need to be eradicated with comprehensive and urgent programs. The use of telemedicine has now proved to be effective in order to improve the MI prognosis and clinical outcomes during the ongoing COVID-19 pandemic. 42 Telemedicine should also be further studied in relation to the re-emergence of severe mechanical complications of MI that are missed due to delayed initial presentation. Eventually, innovative programs should be immediately launched for prompt detection of MI and to possibly circumvent serious mechanical complications amid the commotion elicited by the COVID-19 pandemic.
Learning Objectives
While acute MI presentations have considerably decreased during COVID-19 pandemic, delayed PCI presents a therapeutic dilemma after re-emergence of anachronistic post-MI complications. Clinicians should remain cognizant of rare mechanical complications, including simultaneous LVA and VSR in patients with delayed presentation of acute MI in order to institute prompt and appropriate treatment.
The COVID-19 pandemic and patients avoiding hospitals are causing detrimental effects in late presentation of acute MI, and leading to the resurging of catastrophic mechanical complications.
It is imperative to start educating the community about the formidable clinical value of making the first contact early in individuals with any concerning symptoms and signs despite the fear of acquiring COVID-19.
Footnotes
Author Contributions
All authors contributed equally to the conception and design of the work; the acquisition, analysis, and interpretation of data for the work; and drafting the work or revising it critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.