
Abstract
Pancoast tumor is a rare and aggressive form of lung cancer; cardiac metastasis is very uncommon. We present a case of advanced Pancoast tumor, with extensive cardiac metastases and intracardiac thrombosis in a woman presenting with dyspnea, shoulder pain, and weight loss. A contrast-enhanced chest computed tomographic scan revealed an apical mass, metastatic thoracic nodes, and filling defects within both ventricles. Further imaging with cardiac magnetic resonance imaging revealed 2 left ventricular masses infiltrating into the myocardium suggestive of metastatic disease, and a multilobulated mass within the right ventricle suggestive of intracardiac thrombus. She was initiated on anticoagulation for intracardiac thrombosis. Surgical pathology of biopsied tissue samples was consistent with advanced metastatic lung adenocarcinoma. She was a poor candidate for surgical intervention. Given the patient’s goals of care, she was ultimately transitioned to comfort care.
Keywords
Background
Pancoast tumor is a rare and aggressive form of lung cancer and cardiac metastasis is very uncommon. First described by Dr Pancoast in 1924, 1 Pancoast tumors constitute less than 5% of all lung cancers, with survival rates as high as 55% for patients undergoing complete surgical resection.2,3 Classically, these tumors may be associated with symptoms of ipsilateral shoulder pain, Horner syndrome, and atrophy of hand muscles. 1 We present a case of advanced Pancoast tumor, with extensive cardiac metastases and intracardiac thrombosis in a 54-year-old woman presenting with dyspnea, shoulder pain, and weight loss.
Case Presentation
A 54-year-old woman presented to the emergency room in the context of dyspnea, right shoulder pain, and rapid unintentional weight loss, ongoing for a duration of 2 months. Her medical history was remarkable for coronary artery disease with prior ST-elevation myocardial infarction (status post percutaneous coronary intervention with drug-eluting stent placement in the right coronary artery, 1 year prior to this presentation) and ongoing tobacco use (25-pack-year smoking history). Her outpatient primary care provider had her complete a plain film radiograph of the chest for further evaluation of these symptoms the day prior to presentation, which showed concern for a new lung mass, and she was subsequently referred to the hospital for further evaluation. Her physical examination was largely unremarkable.
Initial laboratory diagnostics revealed leukocytosis (40.5 k/μL; reference range: 4.0-10.8 k/μL), anemia (hemoglobin 8.3 g/dL; reference range: 11.0-14.5 g/dL), thrombocytosis (869 k/μL; reference range: 145-400 k/μL), elevated creatinine (2.00 mg/dL; reference range: 0.52-1.04 mg/dL), elevated

Contrast-enhanced computed tomography scan of the chest revealing an 8.0-cm right apical mass involving the lung and chest wall.
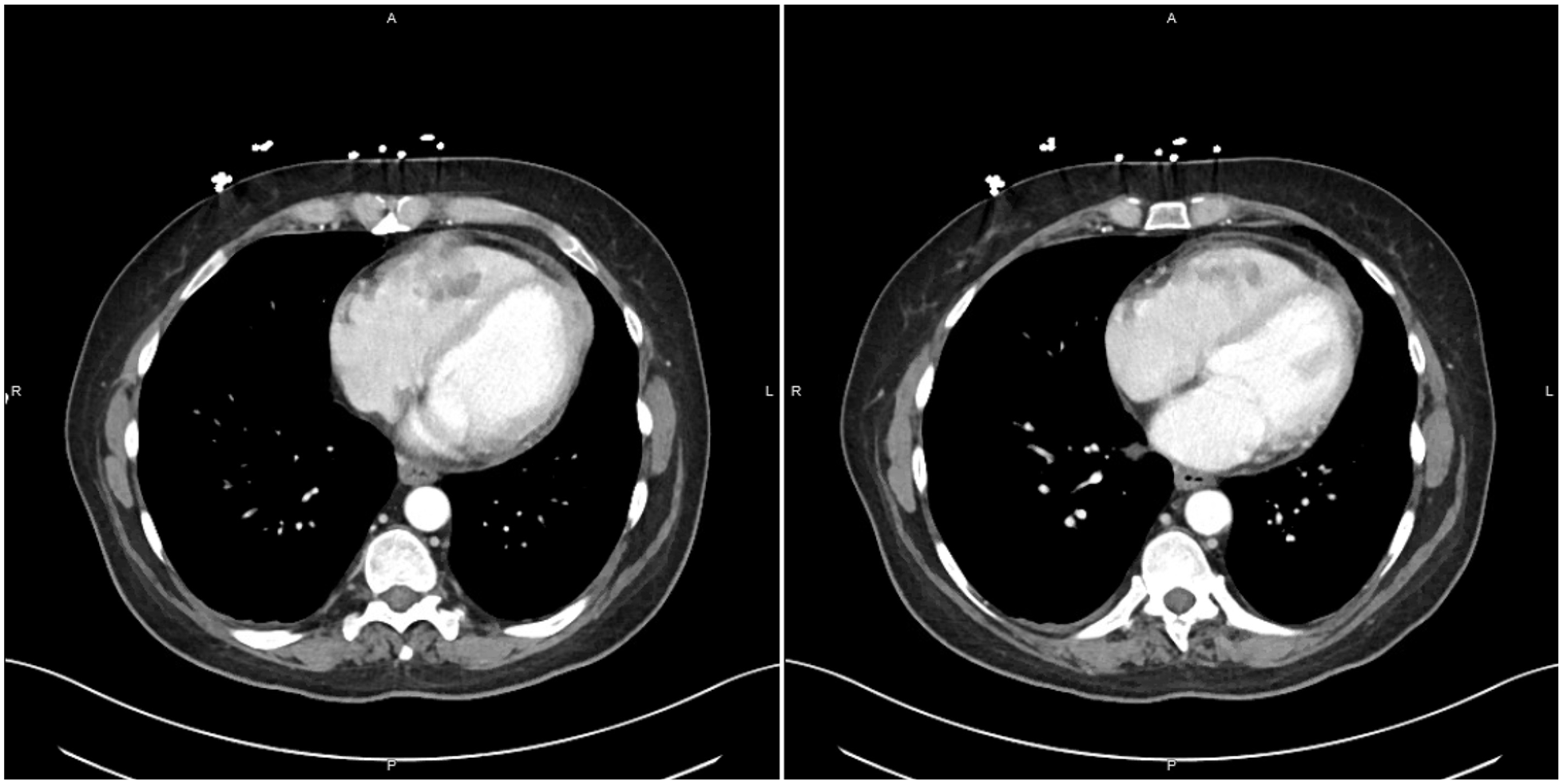
Contrast-enhanced computed tomography scan of the chest revealing 3.6-cm clustered hypodense filling defects in the right ventricle (RV) extending into the anterior ventricular wall with overlying soft tissue density, as well as a 3.0-cm heterogeneous soft tissue mass in the left ventricular (LV) apex appearing to involve pericardium, cardiac fat, and LV myocardium.
Further diagnostic imaging with cardiac magnetic resonance imaging (MRI; Figures 3 and 4) revealed 2 left ventricular masses (basal-mid lateral and apical lateral wall) infiltrating into the myocardium and extending into the pericardium suggestive of metastatic disease. In addition, a multilobulated mass within the right ventricle consisted of a portion invading the right ventricular wall suggestive of metastatic disease, and a portion within the right ventricular cavity suggestive of intracardiac thrombus. Infectious disease laboratory diagnostics including blood cultures, urinalysis, urine streptococcal antigen, and urine Legionella antigen were negative. Biopsy of the colonic mass revealed poorly differentiated carcinoma focally involving colonic mucosa. Biopsy of the chest wall mass revealed poorly differentiated adenocarcinoma. The patient was evaluated by oncology and cardiothoracic surgery and initiated on systemic anticoagulation with therapeutically dosed enoxaparin (1 mg/kg injected subcutaneously every 12 hours). Given advanced metastatic disease with poor prognosis as well as the patient’s decisions on goals of care, she was ultimately transitioned to comfort care.

Cardiac MRI with and without contrast revealing a multilobulated RV mass with a 1.5 cm × 1.6 cm portion attached to and invading the RV wall and a 1.6 cm × 3.0 cm free-floating portion within the RV cavity, as well as 2 LV masses (4.8 cm × 1.7 cm in basal-mid lateral wall and 1.9 cm × 2.7 cm in apical lateral wall), infiltrating into the LV myocardium and extending into the pericardium.
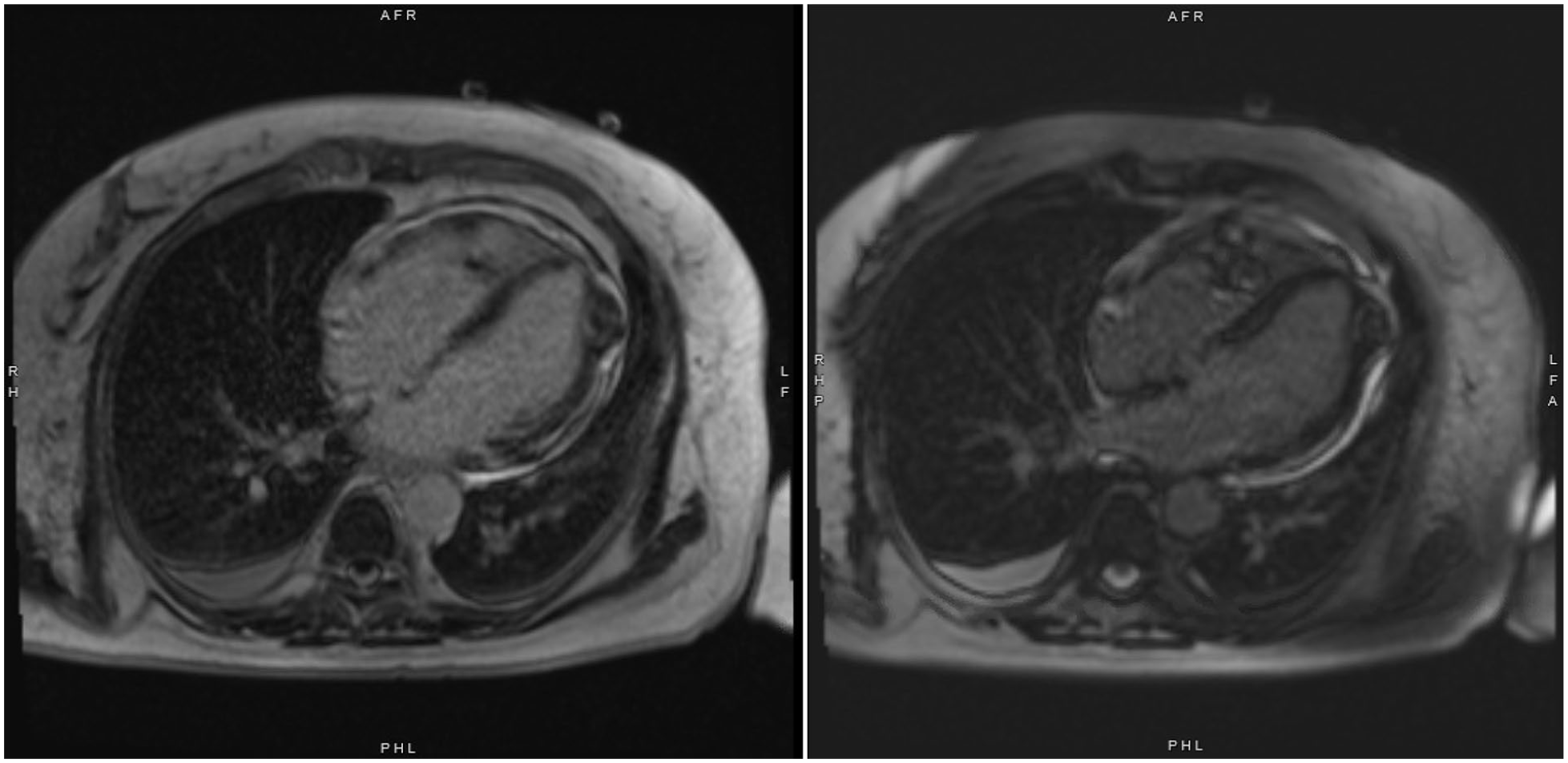
Cardiac magnetic resonance imaging with and without contrast revealing the biventricular masses and heterogeneous enhancement on late gadolinium enhancement imaging.
Discussion
Pancoast tumors are any tumor invading through the parietal pleura at or above the level of the first rib. They constitute less than 5% of all lung cancers. 3 Cardiac metastases from primary tumors outside the heart are 30 times more common than primary cardiac tumors. 4 The most common origin of cardiac metastatic tumors is lung carcinoma in both men and women. 5 To our knowledge, we present the first case report specifically of Pancoast tumor with metastasis to the heart, following an extensive Boolean search of the PubMed database and Google Scholar, using MeSH terms and headings directly applicable to the topic.
While Pancoast tumors are often first seen as radiographic shadow in the apex of the lung, tumors can be missed if it presents as a small apical cap or apical pleural thickening. Chest CT confirms the presence of a superior sulcus mass with invasion of the first 2 ribs and/or vertebral column and possible thoracic inlet invasion. 4 Echocardiography is the best diagnostic tool for intracavitary and mural cardiac tumors to determine localization and size prior to surgery. Computed tomography, MRI, and angiography may further add to diagnostic information. 5
Initially a fatal disease, Pancoast tumors may have survival rates at 5 years as high as 55% for patients who undergo complete resection. 4 This is owed partly due to the trimodality approach of neoadjuvant chemotherapy and radiation prior to surgery that was first introduced in the SWOG 9416 Intergroup 0160 trial in 2007. 2 In addition to the trimodality method, surgical intervention has improved with better approaches and the introduction of video-assisted thoracic surgery.4,6 A recent retrospective study investigating the clinical outcomes of 32 patients who underwent trimodality approach demonstrated similar survival rates at 5 years at 50.1% compared with the SWOG 9416 Intergroup 0160 trial, and 44% of patients had developed pathological clearance. Interestingly, no prognostic value was seen in patients with pathological clearance; however, this was likely a consequence of small sample size. 6 Cardiac metastasis of Pancoast tumor is rare and warrants prompt detection with imaging as well as a multidisciplinary team approach.
Footnotes
Authors’ Note
This case was previously presented as a flatboard complex clinical case abstract at the American College of Cardiology ACC.22 Annual Scientific Session in Washington, D.C. on April 4, 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Consent
Consent for publication has been obtained and the individual who is being reported on is aware of the possible consequences of that reporting.