
Abstract
Pneumoconiosis is associated with coal dust particles depositing within the lung causing nodules coalesce to form progressive massive fibrosis (PMF). Cavitary lesions can develop in these PMF areas for concerns of tuberculosis and aspergillosis. We present a 59-year-old patient who had coal workers pneumoconiosis and PMF presenting with chronic dyspnea and hemoptysis with an upper cavitary lesion noted on chest imaging. He notes dyspnea with walking very short distances with associated productive cough. He admits to occasional wheezing, paroxysmal dyspnea, hemoptysis, and orthopnea but denies chest pain. He is an everyday smoker. His physical examination was only remarkable for bronchial breath sounds. On review of his prior imaging, he had a right upper lobe infiltrate as far back as 2012. As the years progressed, a new cavitary lesion developed in the PMF area which progressively got larger with a thick wall and no eccentric region noted inside the cavity. Tuberculosis test was negative. He underwent a transbronchial biopsy with methenamine silver stain which showed acute angle branching and septation suggestive of Aspergillus species. He was diagnosed with pulmonary aspergillosis and treated with voriconazole for 1 year. With pneumoconiosis and evidence confirming aspergillosis, the presence of a new lung infiltration with progression into a cavitary lesion leads to a diagnosis of chronic cavitary pulmonary aspergillosis (CCPA). With follow-up imaging showing extensive lung fibrosis, he had chronic fibrosing pulmonary aspergillosis (CFPA), a late-stage manifestation of CCPA.
Keywords
Background
Aspergillus is found ubiquitous in nature. 1 Aspergillosis is generally seen in middle-aged people more commonly in men. Aspergillosis manifests systemically in multiple organs with the lung being the most common site of infection. 2 The immune system of the host plays a major role with the infection consisting of a wide spectrum of illnesses ranging from a mild allergy to invasive disease. 3 Acute invasive pulmonary aspergillosis (IPA) is generally seen in severely immunocompromised patients. 2 In immunocompetent patients, there are no symptoms seen. Other presentations include acute IPA, subacute IPA, aspergilloma, and Aspergillus nodule. 2 Chronic forms of Aspergillus infection of the lung with systemic symptoms can be subclassified as subacute IPA/chronic necrotizing pulmonary aspergillosis (CNPA), chronic cavitary pulmonary aspergillosis (CCPA), and chronic fibrosing pulmonary aspergillosis (CFPA). 2 Chronic necrotizing pulmonary aspergillosis is typically seen in those with some degree of immunocompromise who presented with progressive features over 1 to 3 months. 2 Chronic cavitary pulmonary aspergillosis is more common in immunocompetent as formation and expansion of pulmonary cavities over months. 2 Chronic fibrosing pulmonary aspergillosis is a late-stage manifestation of CCPA with extensive lung fibrosis due to noncompliance with treatment. 2
Case Presentation
A 59-year-old man with a past medical history significant for coal worker pneumoconiosis with progressive massive fibrosis (PMF), coronary artery disease with stent placement in the mid-Left anterior descending artery (LAD), chronic obstructive pulmonary disease (COPD), hypertension, and hyperlipidemia presented to the clinic with chronic dyspnea for the last 6 years, which has progressively worsened in the last 8 months. He had associated dysphagia with unintentional weight loss of 30 pounds, which contributed to chronic abdominal pain. He, also, had a chronic cough with clear or yellow phlegm and wheezing but denied any hemoptysis, fever, chills, night sweats, nausea, vomiting, or chest pain. He noted copious black phlegm with on and off dark hemoptysis. His home management included albuterol nebulization twice a day, an albuterol rescue inhaler at least 3 to 4 times a day, and 2 L/min home oxygen. He did admit that he did not use his home oxygen as he should. He is an active smoker smoking 2 packs a day for the last 40 years. He used to be an underground coal miner for 28 years and wore protective equipment at times. Physical examination was only remarkable for bronchial breath sounds with normal respiratory effort.
Chest x-ray imaging (Figure 1) showed a 7.8 mass-like lesion with cavitation in right suprahilar region and the computed tomography (CT) chest showed a right upper lobe 5.4 cm mass with a central cavity with the eccentric region with thick walls (Figure 2). In comparison with previous imaging, he did have a history of a lung infiltrate in the right upper lobe as early as 2012, CT chest from 2012 (Figure 3) showing a large conglomerate mass in the right upper lobe consistent with progressive massive fibrosis which got larger as the years progressed. He had a CT-guided biopsy which was complicated by a pneumothorax needing a chest tube placement. A positron emission tomography (PET) scan was ordered, which showed mild to moderate F-fluorodeoxyglucose (FDG) activity of the pulmonary mass lesion with concerns for malignancy with a standardized uptake value (SUV) of 5.6 to 7.1 and mild to moderate FDG uptake in the mediastinal lymph nodes. He underwent endobronchial ultrasound with right upper lobe transbronchial biopsy with silver stain showing acute angle branching and possible septation making the diagnosis of aspergillosis. He was treated with voriconazole based on infectious disease’s recommendation for 1 year. He had an echocardiogram (ECHO) which showed a normal ejection fraction of 55% to 60%. After 1 year, repeat imaging showed (Figure 4) chronic fibrotic changes involving large portions of the middle, lateral, and basilar portions of the right lung. With further workup, he was found to be an alpha-1 antitrypsin carrier with

A 7.8 mass-like lesion with cavitation in right suprahilar region (circle).
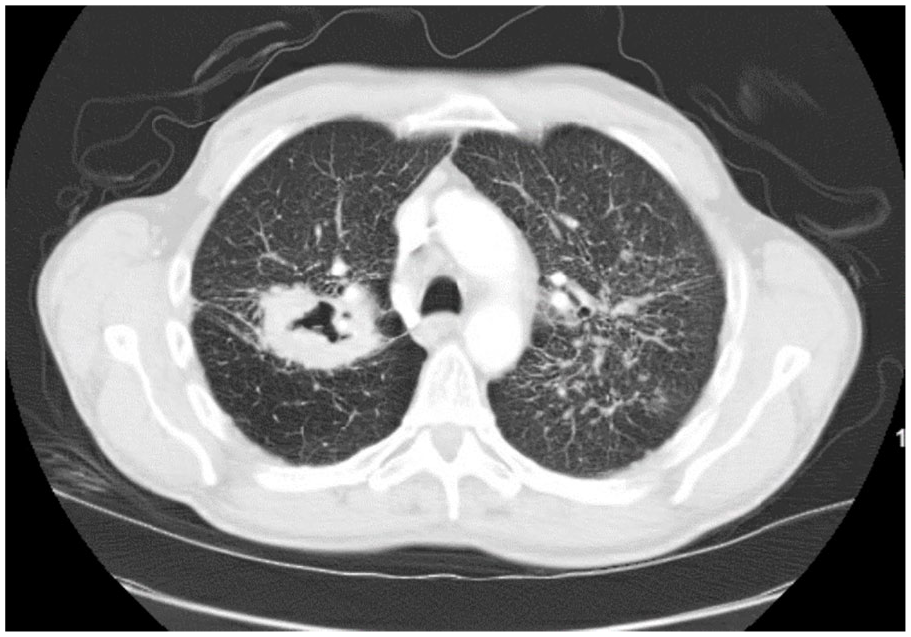
Right upper lobe 5.4 cm mass with a central cavity with the eccentric region with thick walls.

CT chest from 2012 showing a large conglomerate mass in the right upper lobe consistent with progressive massive fibrosis (red arrow).

One year later CT showed chronic fibrotic changes involving large portions of the middle, lateral, and basilar portions of the right lung.
Discussion
Although patients with chronic pulmonary aspergillosis (CPA) are generally immunocompetent, most patients have prior pulmonary damage or disease.2,4-6 It is usually seen in underlying conditions of COPD, sarcoidosis, prior or concurrent tuberculosis (TB) treatment, and non-TB mycobacterial infections.5,6 Given the prognosis of TB, TB needs to be ruled out in those with CPA. Prevalence is often seen in those who are middle-aged and men.2,5 Our patient did have a history of COPD which predisposed him to lung disease. This may have been exacerbated by his coal worker’s pneumoconiosis with PMF which further damages his lungs. Our patient had TB ruled out with the gamma interferon test. There is no set duration of when aspergillosis starts as Heppleston and Gloyne 1 study showed 2 patients diagnosed postmortem with aspergillosis who stopped working in the coal mines 5 and 3 years, respectively. 1 In CPA, pulmonary cavities can sometimes be colonized by a ball of fungal mass known as aspergilloma. 2 In cavities greater than 2 cm in diameter, the risk of developing an aspergilloma is 15% to 20%, as seen in multiple studies. 5 With our workup, our patient did not have any colonization concerning aspergilloma.
Patients typically present with several months of weight loss, chronic cough, hemoptysis of variable severity, fatigue, and/or shortness of breath.2,4-7 Our patient did have a chronic cough, weight loss, and shortness of breath; however, years previously, he had episodes of dark intermittent hemoptysis. Given these constitutional symptoms, CPA is a slowly progressive disease that can often be a silent condition. Therefore, it is typically low on the differential, which leads to late manifestations making it harder to treat. Relapse is common with long-term or lifelong treatment needed if no side effects occur or if resistance has not developed. 5 Diagnosis of CCPA includes a large cavity or, 2 or more cavities on chest imaging with or without aspergilloma in 1 or more of the cavities for at least 3 months with at least one of the following symptoms: fever, weight loss, fatigue, cough, sputum production, hemoptysis or shortness of breath; and a positive Aspergillus IgG with or without a positive lung culture.2,5-10 Several patients with CPA have shown elevated levels of galactomannan and 1,3 beta-D glucan in their serum.6,9,10 They can also have elevated inflammatory markers like C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR) but are not specific. 2
Chronic cavitary pulmonary aspergillosis is generally treated with antifungals such as voriconazole, itraconazole, and posaconazole.3,5 In Bhopalwala et al 11 study, they treated a patient who had COVID-19 with pulmonary aspergillosis with itraconazole due to insurance requirements and fewer side effects, and the patient’s symptoms improved. 11 Side effects of antifungals include liver injury and neuropathy.5-7 Itraconazole can cause edema, heart failure, and hypertension while voriconazole can cause photosensitivity.2,5-7 Voriconazole is the most effective treatment for aspergillosis which our patient received with noted improvement in his symptoms.3,5 Amphotericin B and micafungin, which are salvage therapy, are generally used in patients in whom azoles are contraindicated. 12 In Ouchi et al 3 study, their patient had CNPA which was refractory to both itraconazole and voriconazole but was controlled with micafungin and voriconazole combination before transitioning to voriconazole as maintenance therapy. 3 Medical therapy is usually 4 to 6 months at least and can extend up to 12 months depending on the patient’s response to treatment. The goal of treatment is to minimize the progression of the disease and prevent further damage to the lung. 8 When fibrosis is present, indefinite treatment is recommended to prevent further damage to the lung. 5 Our patient was treated with voriconazole for 1 year after consulting with an infectious disease specialist. Surgery like lobectomy is the last resort as surgical outcomes for CCPA are not as good as they are for a single aspergilloma.2,4-7 For those with hemoptysis, embolization is generally used if there is > 300 mL of blood within 24 hours.6,13 As our patient’s hemoptysis was intermittent and before his diagnosis was made, he was not a candidate for embolization.
Conclusion
Our case shows that patients with pneumoconiosis causing PMF and new-onset cavitary lesions would need further workup to rule out TB and aspergillosis. Aspergillosis is rare but not uncommon in pneumoconiosis with PMF due to the damage to the lungs. Early diagnosis and treatment with antifungals can help improve patients’ symptoms and mortality by preventing the development of CCPA and CFPA which are harder to treat.
Footnotes
Authors’ Note
The case was presented as an abstract at AFMR—Southern regional meeting as a poster, on February 10, 2022, in New Orleans.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient has expired.