
Abstract
Lipoma of the interventricular septum involving the tricuspid valve is a rare entity. A 50-year-old woman presented with exertional dyspnea. She was found to have a large right interventricular septal mass in the initial transthoracic echocardiography. This mass was further investigated by transesophageal echocardiography, cardiac gated CT, and cardiac magnetic resonance imaging. It was found to be lipomatous and embedded into the septal leaflet of the tricuspid valve. The diagnosis was confirmed by biopsy. Surgical exploration revealed that the mass was deeply embedded in the interventricular septum and septal leaflet of the tricuspid valve. The mass was resected along with sections of the interventricular septum and tricuspid valve. She underwent bioprosthetic tricuspid valve placement and patch reconstruction of the interventricular septum. We also searched case reports from MEDLINE and studied pathological and epidemiological characteristics of the published cases of cardiac masses in the past year. Cardiac lipoma although a benign tumor can cause serious hemodynamic complications. Initial transthoracic echocardiography followed by multimodality imaging is the cornerstone of the diagnosis.
Background
Cardiac tumors are very rare with a reported prevalence of 0.15%.1,2 Secondary cardiac tumors were found to be more than 100-fold more common than primary cardiac tumors. 3 It can be classified as neoplastic and nonneoplastic. Neoplastic tumors can be further classified as primary benign, malignant, or metastatic. Ninety percent of primary cardiac tumors are benign. In order of decreasing frequency, benign cardiac tumors in adults include myxoma, lipoma, papillary fibroelastoma, rhabdomyoma, fibroma, and cardiac paraganglioma. 2 The remaining 10% of primary cardiac tumors are malignant and include angiosarcoma, leiomyosarcoma, rhabdomyosarcoma, osteosarcoma, undifferentiated sarcoma, primary cardiac lymphoma, and mesothelioma. Cancers that metastasize to the heart include melanomas, breast, lung, esophagus, midgut, liver, head, and neck. 2 The prognosis of primary malignant cardiac tumors is poor. Clinical presentation depends upon their location in the heart. Most benign tumors are clinically silent and are observed over time. Some benign cardiac tumors may have significant hemodynamic complications depending on their location. Cardiac lipoma is a nonneoplastic benign entity. It is typically located in the right atrium and right ventricle, and is asymptomatic. It is usually diagnosed incidentally and does not require any surgical treatment. We report a rare case of lipoma of the interventricular septum, engulfing the septal leaflet of the tricuspid valve, and causing significant right ventricle (RV) inflow tract obstruction. We describe an atypical presentation of a cardiac lipoma and the role of multimodality imaging in the workup of cardiac mass.
Case Presentation
A 50-year-old woman with a past medical history of class II obesity and obstructive sleep apnea presented with months of exertional dyspnea. The physical examination was remarkable for a body mass index of 37. The labs, electrocardiography (ECG), and chest radiography were normal. Transthoracic echocardiography (TTE) demonstrated a large and hyperechoic right ventricular inflow tract mass, a thickened interventricular septum, and normal left ventricular systolic function. Transesophageal echocardiography (TEE) showed that the mass obstructed the right ventricular inflow tract, obscured the septal leaflet of the tricuspid valve (Video 1), and the interventricular septum was hypertrophic (Video 2). A gated cardiac CT (CCT) demonstrated a large fatty mass involving the interventricular septum, right ventricle, and septal leaflet of the tricuspid valve (Images 1-5). The mass had fat attenuation (Hounsfield unit of −79) and was not encapsulated. Cardiac magnetic resonance (CMR) imaging further demonstrated that the mass was hyperintense in T1W and hypointense in T2W fat suppression sequences and lacked early and late gadolinium enhancement, suggestive of lipoma (Images 6-10). She underwent percutaneous endomyocardial biopsy and the pathology was consistent with lipoma.
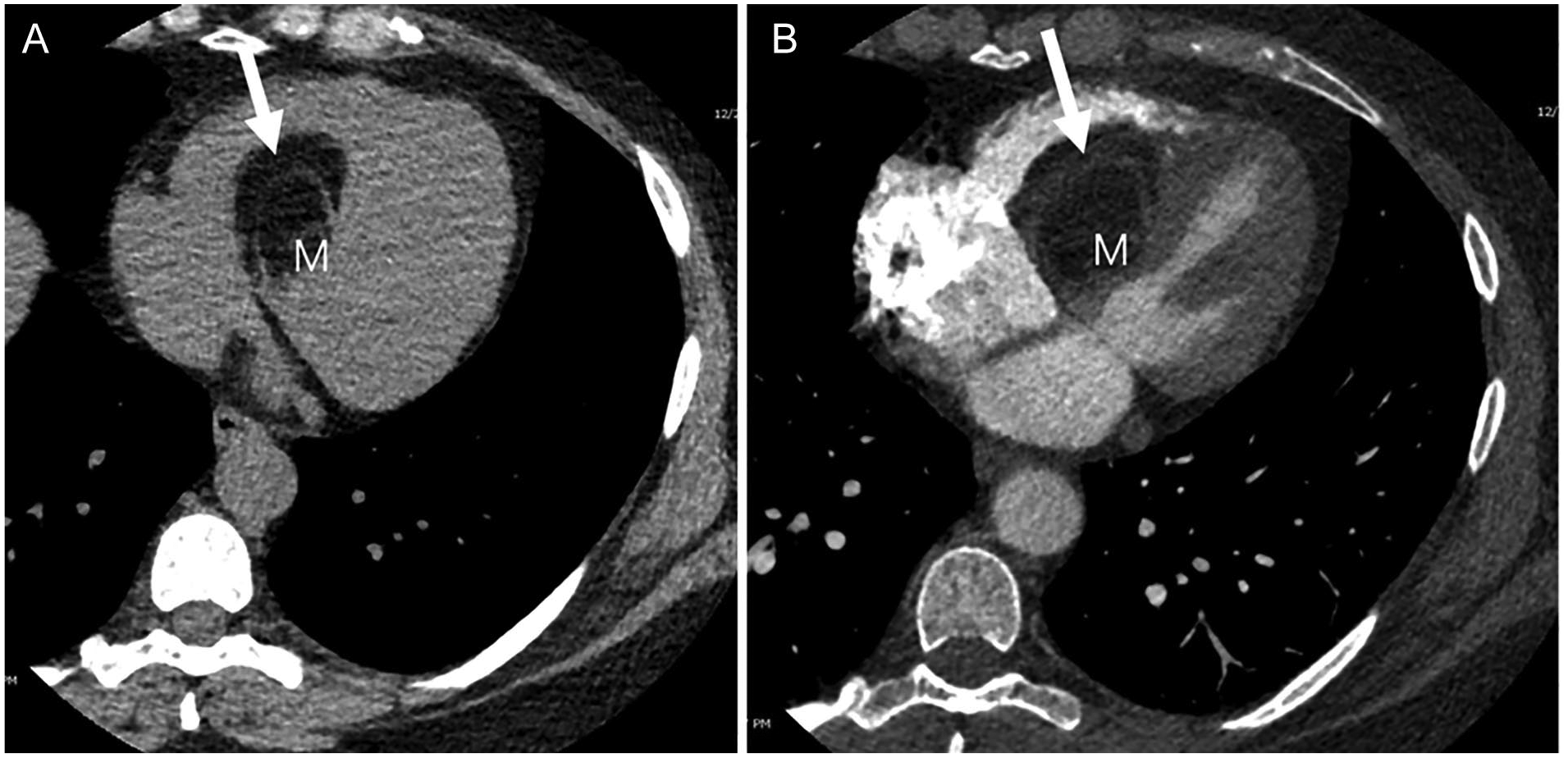
(A) Initial cardiac gated axial acquisition obtained prior to intravascular contrast administration demonstrates a fat attenuation mass (M, Hounsfield unit of −79) with nonenhancing soft tissue strands (arrow) within the heart. (B) Prospective cardiac gated CT angiography with timing over the left atrium at 40% of the cardiac cycle shows that the soft tissue strands within the mass (M) are nonenhancing (arrow).

Cardiac gated CT angiogram, post-contrast coronal reconstruction shows that the fat attenuation mass (M, Hounsfield unit of −79) arises from the interventricular septum between the RV and LV.

Cardiac gated CT angiogram, post-contrast sagittal reconstruction shows the unencapsulated contour of the fat-attenuation mass (M).

Cardiac gated CT angiogram, enhanced 4-chamber reconstruction at end-systole before the opening of the mitral valve (*) shows that the mass (M) involves the tricuspid valve (arrow).

Cardiac gated CT angiogram, 3D reconstruction shows the mass (M) projecting into the RV.

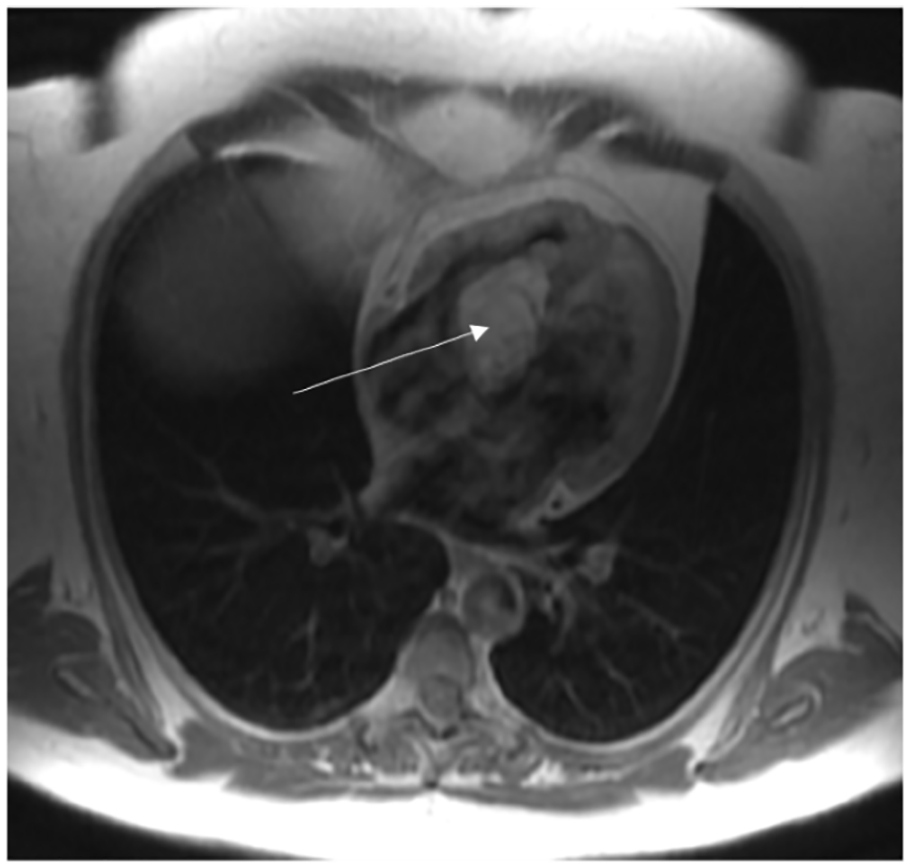
Non-gated axial FIESTA CMR demonstrating hyperintense mass in the interventricular septum (arrow) protruding into the right ventricle. The mass demonstrates mixed intensity regions within and hypointense wall which is of similar intensity and in continuation with the tricuspid valve as well as interventricular septum. The mass has similar intensity to skeletal muscle.

Axial ECG-gated T1-weighted 4-chamber CMR demonstrates the hyperintense mass with heterogenous areas and septations within (arrow).

T2-weighted triple inversion recovery fast spin echo sequence demonstrates markedly suppressed mass with the application of fat suppression (arrow). Note equivalent suppression of signal in the mass and in the mediastinal and subcutaneous fat.
Immediate post-gadolinium-enhanced axial ECG-gated T1-weighted SE image shows no enhancement of the mass as well as no enhancement of heterogeneous regions within the mass (arrow).

Axial gadolinium-enhanced ECG-gated T1-weighted SE CMR acquired after 3 to 5 minutes of contrast administration shows no enhancement of the mass as well as no enhancement of heterogeneous regions within the mass (arrow).
Given symptoms and the size of the mass, she underwent open-heart surgery under cardiopulmonary bypass. The mass was found to obstruct the RV inflow tract. It firmly adhered to the septal leaflet of the tricuspid valve, septal chordae, and subvalvular attachments and was deeply embedded in the interventricular septum. As the mass was dissected, it was found that the mass was unencapsulated, had formed no plane, and was intermixed with the muscle fibers of the septum. It was removed in sections, along with the tricuspid valve septal leaflet and chordal attachments. The interventricular septum was very thin and redundant at the end of the surgery as a portion of septal tissue had to be excised along with the mass. It was reconstructed and closed with patches and a bioprosthetic tricuspid valve was placed. A bioprosthetic valve was used because the patient opted for a tissue valve. Post-procedure TEE revealed good RV function and normal functioning bioprosthetic tricuspid valve, no residual tumor, and no ventricular septal defect (Videos 3 and 4). The excised tan-yellow rubbery fragmented fibro-fatty tissue was sent for histopathology. The histopathology revealed benign adipocytes in the background of cardiac myocytes. Immunohistochemical stain for MDM2 (Mouse double minute homolog) was negative, thus excluding liposarcoma. The overall findings were consistent with lipomatous tissue (Image 11). Her symptoms subsided after surgery. She is being followed up in the clinic with surveillance echocardiography and is free from recurrence.

H&E stain of the interventricular septal mass showing admixed adipocytes (arrow) and cardiac muscle fibers (arrow head), 10×3 magnification.
Discussion
Lipoma of the interventricular septum is rare. In contrast to a typical lipoma, invasive lipoma in our patient was unencapsulated, lacked well-defined borders, infiltrated deep into the myocardial fibers, and caused obstructive symptoms. Nonencapsulated lipomas have been only described in the literature with lipomatous hypertrophy of the interventricular and interatrial septum. 4 Surgery is not indicated in asymptomatic patients with typical lipoma as the risk of malignancy is low. After our patient presented with exertional symptoms, initial echocardiography found right ventricular inflow tract obstruction and tricuspid valve involvement. The pathology and extent of the tumor were further investigated by multimodality imaging (CMR and CCT) and finally confirmed by biopsy. Our case was very atypical of a lipoma as it deeply embedded into the interventricular septal myocardial fibers and involved the septal leaflet of the tricuspid valve and chordal structure, thus requiring surgical resection along with the removal of the tricuspid valve and sections of the interventricular septum, followed by prosthetic tricuspid valve replacement and interventricular septum reconstruction.
Multimodality imaging plays a vital role in the investigation of suspected cardiac masses assessing location, size, and hemodynamic consequences. Multimodality imaging followed by percutaneous endomyocardial biopsy, like in our patient gives clues to the diagnosis. The TEE and 3-dimensional echocardiogram can better evaluate the anatomical relationships and dynamic complications. CMR, cardiac gated CT, and positron emission tomography (PET) can further characterize the lesion and help identify and plan further diagnostic tests and management. 2 CMR is the gold standard for the work-up of the suspected fat tumor as it helps differentiate the pure adipose tissue from the mixed adipose and nonfatty masses by fat suppression sequences. The fat appears dark in suppression imaging. CMR additionally helps in evaluating its malignant potential by assessing its situation, dimensions, extent, local invasion, pre- and post-contrast T1W, pre-contrast T2W images, and delayed gadolinium-enhancement. 5 The tumors showing first-pass perfusion (FPP) and delayed gadolinium-enhancement are likely malignant.5,6 Malignancy cannot be ruled-out by multimodality imaging alone and tissue biopsy is confirmatory. Immunohistochemical stains help characterize the nature of adipocytic tumors. Atypical lipomatous tumor/well-differentiated liposarcoma (WDL) and dedifferentiated liposarcoma (DDL) are known to overexpress MDM2 and CDK4 cell cycle oncogenes and cell cycle regulator p16 while benign adipocytic tumors are not. 7 Invasive lipoma should be differentiated from liposarcoma. Liposarcoma is known to demonstrate spindle cells, hyperchromatic nuclei, and multivacuolated lipoblasts embedded in a loose myxoid to dense fibrous stroma on histopathological examination. 8
Epidemiologic and Pathological Review
We searched case reports from MEDLINE and studied pathological and epidemiological characteristics of the published cases of cardiac masses in the past year, from July 2020 to June 2021. A MEDLINE search yielded 227 case reports and abstracts about different types of cardiac masses in the past 1 year. We compiled the demographics, clinical features, pathology, mass location, and imaging modalities used for the different cardiac masses (Table 1). Our study showed that cardiac tumors, although rare can have a myriad of clinical presentations, even when benign. The time of presentation can range from early fetal age to the 10th decade of life. Clinical presentation of primary cardiac mass varies from no symptoms to shortness of breath, non-ACS chest pain, pericardial effusion, cardiac tamponade, cardiac arrhythmias, stroke/TIA, congestive heart failure, LVOT/RVOT obstruction, and valvular obstruction.
Epidemiologic and Pathological Review of the Published Cases of Cardiac Masses.
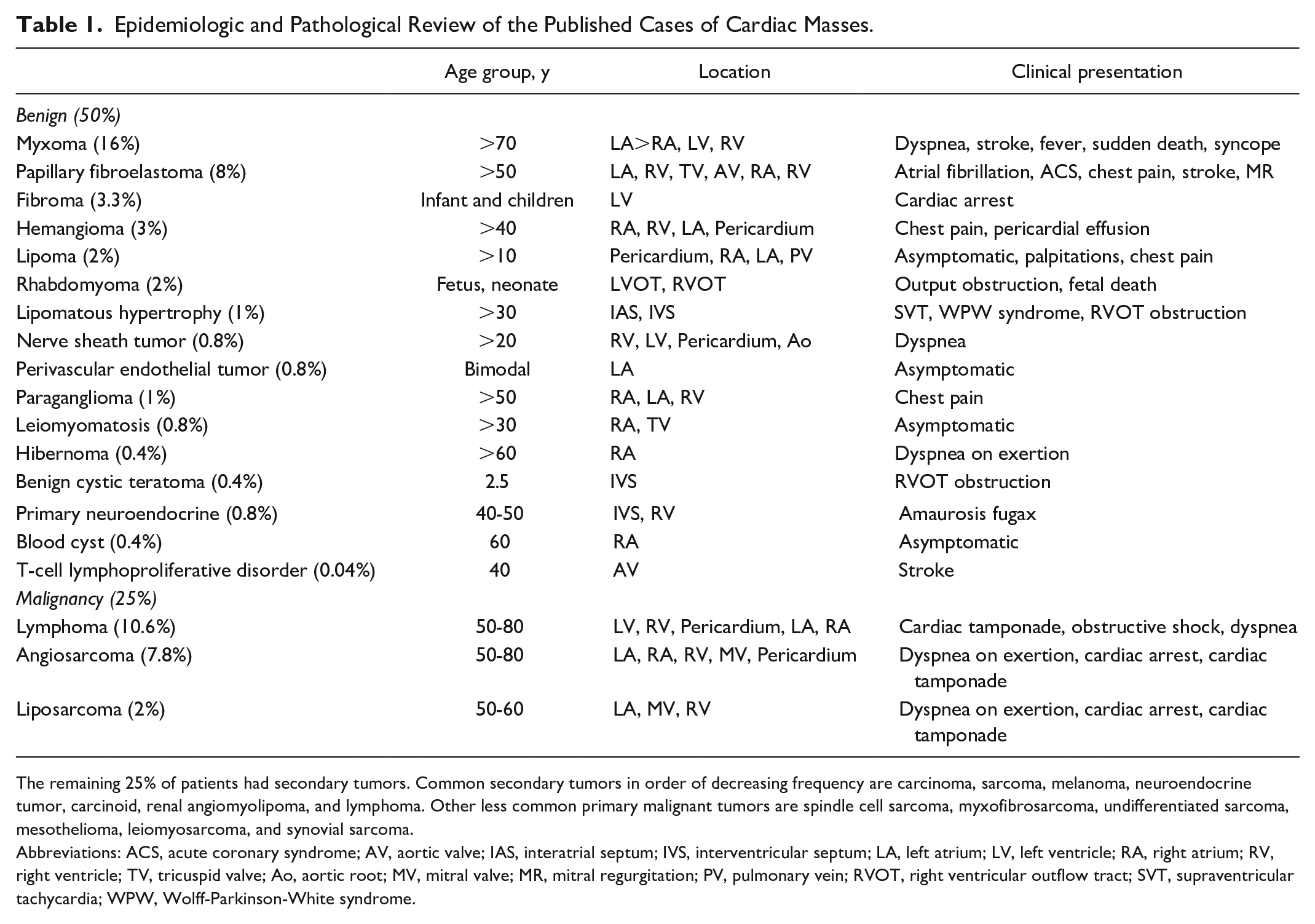
The remaining 25% of patients had secondary tumors. Common secondary tumors in order of decreasing frequency are carcinoma, sarcoma, melanoma, neuroendocrine tumor, carcinoid, renal angiomyolipoma, and lymphoma. Other less common primary malignant tumors are spindle cell sarcoma, myxofibrosarcoma, undifferentiated sarcoma, mesothelioma, leiomyosarcoma, and synovial sarcoma.
Abbreviations: ACS, acute coronary syndrome; AV, aortic valve; IAS, interatrial septum; IVS, interventricular septum; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TV, tricuspid valve; Ao, aortic root; MV, mitral valve; MR, mitral regurgitation; PV, pulmonary vein; RVOT, right ventricular outflow tract; SVT, supraventricular tachycardia; WPW, Wolff-Parkinson-White syndrome.
Conclusion
Although cardiac lipoma is a rare benign cardiac mass and can be followed over time, it can cause hemodynamic consequences and require surgery if unusually large and involves a valve. An early diagnostic evaluation of the cardiac masses by TTE followed by multimodality imaging (TEE, CMR, contrast-enhanced CT, and PET-CT) can better characterize anatomic extent and hemodynamic significance, predict a histologic diagnosis, and guide medical and surgical management. A biopsy is the gold standard for diagnosis. Regular follow-up with surveillance echocardiography should be done after surgery to assess for recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual case report.
Informed Consent
Informed consent for patient information to be published was not obtained because no patient identifiers were used in the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.