
Abstract
Colonic diverticular bleeding is an established cause of painless acute lower gastrointestinal hemorrhage. Colonoscopy, performed within 24 hours of presentation, is the usual initial diagnostic procedure in such patients. In order to improve the diagnostic and therapeutic yield of urgent colonoscopy, adequate colon cleansing is required in patients with signs and symptoms of ongoing bleeding. We hereby delineate the importance of rapid bowel preparation with a very-low-volume novel 1 L polyethylene glycol ascorbate solution in the setting of acute severe colonic diverticular bleeding. The 1-L regimen may demonstrate similar efficacy to that of traditional higher volume preparations and it can substantially reduce the time for bowel preparation. Therefore, it can be considered for bowel purge when colonoscopy has to be rapidly planned in critical patients. This article further illustrates that the endoscopic technique using epinephrine followed by direct hemoclipping may be added to the armamentarium for acute colonic diverticular hemorrhage as the first treatment, especially in elderly patients with multiple comorbid conditions. While ample evidence surrounding the efficacy of the clipping method persists in the literature, rapid bowel preparation with 1 L polyethylene glycol ascorbate solution’s imperativeness to achieve hemostasis with direct hemoclipping remains elusive.
Keywords
Introduction
Diverticular bleeding is one of the common causes of lower gastrointestinal hemorrhage, with an estimated prevalence ranging from 20% to 41.6%.1,2 After initial assessment and hemodynamic stabilization, colonoscopy is performed in these patients. 2 Adequate bowel preparation remains the cornerstone of an efficacious colonoscopy procedure. It lends the possibility of appropriate endoscopic visualization, detection, and treatment, and it may reduce the risk of procedural adverse events. Inadequate colon cleansing frequently leads to a failed colonoscopy in the inpatient setting, culminating in a prolonged hospital stay and increased cost. 3 The European Society of Gastrointestinal Endoscopy guidelines currently recommend the use of high- or low-volume polyethylene glycol preparations as well as otagents in a split-dose regimen for routine bowel preparation. 4 However, the tolerability of higher volume solutions may pose problems, resulting in a suboptimal bowel preparation in up to 33% of patients.5-7 Conversely, the low-volume preparation can improve patient compliance, the willingness to repeat the same regime, acceptability, and it can decrease the overall adverse events while offering similar efficacy as traditional regimens. 8 Recently, a very-low-volume 1 L polyethylene glycol ascorbate solution has been introduced in order to improve patient compliance by decreasing the total volume of liquid intake. It creates an enhanced laxative effect with an increased dose of ascorbate, which permits delivery of the solution in a smaller volume. 9 Based on this rationale, this novel preparation can also facilitate urgent colonoscopy for early identification of the bleeding lesions, potentially avoiding hemodynamic complications. While low-volume regimens have been used in colorectal cancer screening, endoscopists have not extensively adopted them in clinical practice mainly due to perceptions of low efficacy. 10 Therefore, the use of 1 L polyethylene glycol ascorbate solution for urgent colonoscopy in patients with lower gastrointestinal hemorrhage remains exceedingly rare.
With regard to endoscopic treatment, several techniques have been employed with varied efficacy and safety profiles. Direct endoscopic hemoclipping in patients with diverticular hemorrhage may have a theoretical hemostasis benefit over other endoscopic methods as it causes less damage to adjacent tissues. 11 However, the accurate hemoclip placement for severe diverticular bleed remains relatively difficult due to poor visualization. The present report is unique as it signifies the importance of rapid bowel preparation using 1 L polyethylene glycol ascorbate solution facilitating direct endoscopic hemoclipping for a severely bleeding mid-ascending colonic diverticulum, resulting in successful long-term hemostasis.
Case Presentation
This case study involves an 85-year-old male hospitalized for hemodynamic compromise and orthostatic changes, secondary to massive lower gastrointestinal bleeding. His medical history was significant for type 2 diabetes mellitus, coronary artery disease status post coronary artery bypass grafting, and cerebrovascular accident. In addition to the standard medical treatment for his chronic illnesses, he received ongoing anticoagulant therapy with aspirin 150 mg/day. There was no history of gastrointestinal bleeding events, abdominal and/or vascular surgeries, peptic ulcer disease, inflammatory bowel disease, or abdominopelvic radiation therapy. In the emergency department, initial resuscitation was performed with intravenous fluids and packed red blood cell transfusions. Physical and abdominal examinations were unremarkable. The patient had a favorable geriatric performance status. A multidisciplinary team with expertise in surgery, interventional radiology, and advanced endoscopy recommended endoscopic therapy after risk assessment and stratification. He was informed about the benefits and risks of potential complications associated with this treatment modality.
Investigations
Laboratory parameters revealed posttransfusion hemoglobin level of 9.4 g/dL (normal = 12.0-15.5 g/dL). His international normalized ratio was 2.5 (normal = 2.0-3.0). The metabolic and renal profiles were normal. The testing results for liver function and urinalysis were also within normal limits. A hepatitis panel was negative. For cardiac clearance, echocardiography was undertaken. It revealed a left ventricular ejection fraction of 56% with no valvular abnormalities. After achieving the hemodynamic stability with normalization of blood pressure and heart rate, a nasogastric tube was passed. The nasogastric aspirate was negative, potentially excluding an upper gastrointestinal bleeding source. In order to avoid aspiration due to the altered mental status of the patient, the nasogastric tube was retained in place for subsequent administration of rapid bowel preparation. The antiemetic agent was given immediately prior to initiating the colon preparation to decrease nausea and facilitate gastric emptying. For a rapid bowel purge, 1 L polyethylene glycol ascorbate solution (Plenvu; Salix Pharmaceuticals) was rapidly instilled through the nasogastric tube followed by 1 L water, over 2 hours. Radiographic investigations were not performed as the patient adequately responded to hemodynamic resuscitation and tolerated the bowel preparation well, with no fluid and electrolyte abnormalities.
Diagnosis and Treatment
Urgent colonoscopy was performed 2 hours after the end of the solution administration, with the patient in stable but critical clinical condition. Rapid instillation of polyethylene glycol ascorbate solution permitted excellent bowel preparation (Boston Bowel Preparation Scale 9). Colonoscopy revealed severe right-sided diverticulosis with wide-mouthed diverticula, having the starting point at the hepatic flexure. An actively bleeding artery, originating from a mid-ascending colonic diverticulum, was identified after careful irrigation and gentle endoscopic manipulation. The patient was diagnosed with severe acute colonic diverticular hemorrhage. With regard to the therapeutic endoscopic technique, a total of 8 mL of epinephrine in a 1:10 000 concentration was initially administered at the bleeding vessel. The bleeding slowed but continued. Subsequently, 3 metallic hemoclips (HX-610-090L; Olympus Medical Systems) were gently and carefully inserted into the diverticulum neck followed by their direct application at the actively spurting artery (Supplementary Video 1, available online).
Clinical Outcome and Follow-up
The endoscopic intervention resulted in successful hemostasis. The postprocedure clinical course was unremarkable, and the patient remained stable. Due to his established cardiovascular disease, the secondary prophylaxis with aspirin was resumed. He was educated to avoid non-aspirin nonsteroidal anti-inflammatory drug use after his acute lower gastrointestinal bleeding. He was discharged home a few days later with no evidence of recurrent diverticular bleeding or any adverse events. At the 1-week follow-up, he showed excellent recovery and he did not experience another bleeding episode. At the end of 1 and 6 months after direct hemoclip treatment, the patient developed no symptoms or signs of a recurrent diverticular bleed. At the subsequent long-term follow-up visits, the colonic diverticular hemorrhage did not recur, without the need for a repeat endoscopic intervention, transcatheter arterial embolization, or surgery.
Discussion
Colonoscopy is routinely considered the first-line investigation in patients presenting with acute diverticular bleeding. 12 Poor colonic visualization not only hampers accurate detection of the lesion site but also leads to inadvertent delays in management. Therefore, a rapid and effective method of bowel preparation carries paramount importance for the clinical outcomes and decreasing the risk of rebleeding, particularly in patients with evidence of ongoing hemorrhage after initial resuscitation.13,14 The American College of Gastroenterology clinical guidelines traditionally recommend rapid purge for urgent colonoscopy in high-risk patients using 2 to 6 L of polyethylene glycol or another similar solution, administered over 3 to 4 hours. 15 However, it is notable that the high-volume preparations delay the procedure and are poorly acceptable to patients. 15 For elective colonoscopy, the new 1 L polyethylene glycol ascorbate (NER1006) bowel preparation has shown non-inferiority compared with 2 L polyethylene glycol ascorbate, trisulfate, and sodium picosulfate with magnesium citrate.16-18 In the meta-analysis of 3 clinical trials, NER1006 showed a significantly higher overall cleansing success in comparison to traditional preparations both when evaluated with Harefield Cleansing Scale and Boston Bowel Preparation Scale, as well as a significant greater high-quality cleansing of the right colon when assessed with the Harefield Cleansing Scale (Table 1). 19 Notably, the lower volume or alternative bowel preparations have previously been evaluated for colon cancer screening and surveillance in elective colonoscopy but their use is uncommon in the setting of acute lower gastrointestinal bleeding.20,21 To the best of our knowledge, the use of 1 L polyethylene glycol ascorbate solution in severe acute colonic diverticular bleeding remains extremely rare.
Characteristics of Studies Evaluating the Efficacy of 1 L Polyethylene Glycol (NER1006) in Patients Undergoing Elective Colonoscopy.

Abbreviations: RCT, randomized controlled trial; HCS, Harefield Cleansing Scale; BBPS, Boston Bowel Preparation Scale; TEAEs, treatment-emergent adverse events; PEG, polyethylene glycol; mFAS, modified full analysis set analysis; PP, per protocol analysis.
In our case, rapid bowel preparation with a very-low-volume 1 L polyethylene glycol ascorbate solution over 1 hour helped achieve clear visualization (Boston Bowel Preparation Scale 9). Colonoscopy was performed 2 hours after the completion of the solution administration, which was before the commonly recommended 8-hour duration. The effectiveness of a transparent hood attached to the colonoscope tip for bleeding site identification has been reported. However, we did not have a transparent cap available at the time of the procedure. Moreover, simethicone was not used during colonoscopy, resulting in frequent intraluminal bubbles. Despite these factors, a clear and unmistaken localization of the bleeding diverticular lesion enabled us to apply the endoscopic treatment directly to the lesion. A few reports in the literature may also support urgent colonoscopy without preparation. However, the European Society of Gastrointestinal Endoscopy guidelines vehemently argue against unprepared sigmoidoscopy in the setting of acute diverticular hemorrhage. 4 In such circumstances, cecal intubation rates remain concerningly low, and inept or inadequate delineation of the lesions might also lead to an increased risk of perforation. 22 While rapid bowel preparation remains focal in yielding favorable outcomes, patients with poor mentation may aspirate such preparations. In such situations, a nasogastric tube can be employed to minimize the risk of aspiration. In prior studies regarding urgent colonoscopy, up to one third of patients required a nasogastric tube to instill rapid bowel preparation. 23
Patients presenting with acute severe hematochezia should undergo prompt assessment concurrently with initial resuscitation.15,23 The exclusion of an upper gastrointestinal bleeding source is warranted in cases of hemodynamic compromise. In high-risk patients and ongoing hemorrhage, urgent colonoscopy is performed following a colon purge. The patients with ongoing bleeding and stigmata of recent hemorrhage can be safely and effectively managed with endoscopic therapy. 23 The approach to manage high-risk patients is outlined (Figure 1). Endoscopic techniques such as thermocoagulation, epinephrine injection, banding, endoscopic detachable snare ligation, topical hemostatic agents, hemoclipping, and over-the-scope clip have recently been proposed for colonic diverticular bleeding.12,24 However, no consensus exists due to inherent limitations of colonoscope reinsertion and the high cost associated with each technique. In a meta-analysis of cumulative evidence, Nagata et al demonstrated that endoscopic ligation therapy was more effective compared with hemoclipping in reducing short- and long-term recurrence. 25 However, Kishino et al supported direct hemoclipping as the first treatment over indirect hemoclipping and endoscopic band ligation for diverticular bleeding. 26 It is notable that band ligation and coagulation modalities manifest an increased risk of perforating thin-walled diverticula. 27 In this context, direct endoscopic hemoclipping yields the added benefit of facilitating a safer procedure with a minimal vessel-wall injury.28,29 Furthermore, clipping offers a relatively better technical feasibility for effective hemostasis. The improved hemoclip design shows higher tensile strength and it enables appropriate positioning before application. Pertinently, direct hemoclipping can sometimes be complicated due to endoscopic observation, clip insertion into the diverticula, and/or stability of the endoscope. 25 However, water immersion observations, placing an open clip in the endoscope, and using a longer tip hood may help in circumventing the aforementioned problems. 28

Summary of the algorithm for the management of high-risk patients presenting with acute lower gastrointestinal bleeding. UGI, upper gastrointestinal; EGD, esophagogastroduodenoscopy; NGT, nasogastric tube.
The bleeding lesion in this patient was located in the diverticular neck. It did not self-resolve and resulted in an unremitting hemorrhage. In order to curb the bleeding and prevent the onset of hemodynamic instability, 8 mL of epinephrine was initially injected. It not only slowed down the bleeding but also helped in specifically localizing the culprit bleeder. Direct clipping was then undertaken, which resulted in prompt hemostasis. Generally, direct hemoclipping is not recommended for a massive active diverticular bleed due to the poor visual field. However, in our case, the patient’s postprocedure recovery was uneventful, with no adverse events or recurrent bleeds. Notably, diverticular pathologies are established to be the most common cause of readmission secondary to rebleeding episodes, constituting a pressing concern. 30 Therefore, rapid bowel preparation followed by an effective endoscopic technique may help in avoiding recurrent diverticular hemorrhage.
With pertinence to the benefits of urgent colonoscopy, prior research has demonstrated more definite diagnoses, reduced rebleeding rate, and fewer subsequent surgeries (Table 2).23,31,32 Furthermore, it can decrease the length of hospital stay, which may lower associated hospital expenditures.33,34 It can also help in improving diagnostic yield by offering prompt and better detection of bleeding source, resulting in early discharge of low-risk patients.34,35 Consequently, the risk of nosocomial infections and adverse events can also be decreased. In a meta-analysis, Kouanda et al showed that the length of hospitalization was 4.8 ± 2.7 days in the urgent colonoscopy group, whereas it was 6.4 ± 3.2 days in the elective colonoscopy group. 36 In addition, the hospital cost was also lower in the urgent colonoscopy group at $24 866 versus $27 691 in the elective group. 36 Therefore, an urgent colonoscopy may facilitate the provision of high-quality and safe patient care with the containment of valuable hospital resources. Thus, rapid bowel preparation, coupled with an effective endoscopic technique in urgent colonoscopy, may help in further optimizing the management algorithm for patients with acute lower gastrointestinal bleeding.
Prospective Studies of Urgent Colonoscopy for Acute Lower Gastrointestinal Bleeding.
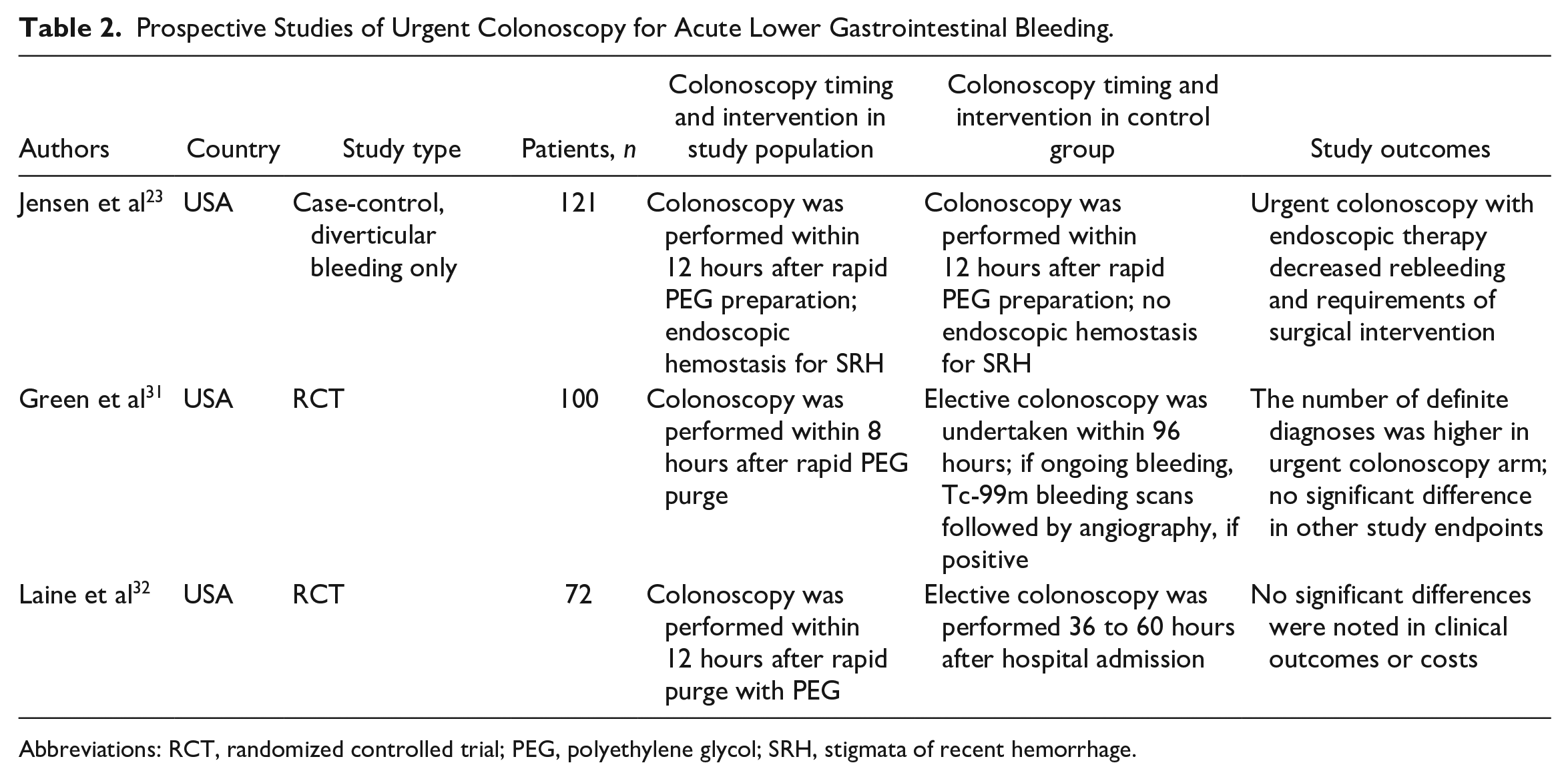
Abbreviations: RCT, randomized controlled trial; PEG, polyethylene glycol; SRH, stigmata of recent hemorrhage.
Learning Points
For urgent colonoscopy, rapid bowel preparation using the new 1 L polyethylene glycol ascorbate solution over 1 hour can be considered in a critical patients with severe acute diverticular hemorrhage.
The 1-L regimen may demonstrate similar efficacy to that of higher volume preparations, with a significant decrease in time required for bowel preparation. It is clinically important to improve diagnostic and therapeutic yields of urgent colonoscopy.
After adequate colon cleansing with rapid bowel preparation, endoscopic technique using initial epinephrine administration can further help to pinpoint the exact location of the bleeder within the diverticulum.
The relatively easier endoscopic application and reduced risk of diverticular perforation, direct hemo clipping can afford a convenient and relatively safe procedure. It may also promise favorable long-term clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.