
Abstract
Endometriosis is a gynecological condition that can manifest in pelvic and extra-pelvic sites, including the gastrointestinal tract. Cecal and appendiceal involvement is rare and can present as anemia, mimicking malignancy. The discussed case is of a 50-year-old female who presented with symptomatic anemia. Imaging revealed a cecal and appendiceal mass with lymphadenopathy, raising concern for malignancy. Colonoscopy showed a suspicious tumor, but biopsy was inconclusive. Surgical resection revealed extensive endometriosis involving the cecum and appendix. Pathology confirmed endometriosis mimicking neoplasia. Postoperatively, the patient’s anemia improved. This case highlights that gastrointestinal endometriosis is often asymptomatic and difficult to diagnose. Its presentation as a colonic mass underscores the need for broad differentials. Surgical intervention is crucial when malignancy is suspected.
Introduction
Endometriosis is a chronic and often debilitating gynecological condition characterized by the presence of endometrial-like tissue outside the uterus. 1 It has a high prevalence of 8% to 10% with the highest incidence seen in women of childbearing age. 2 Despite its widespread occurrence, diagnosis of endometriosis has been particularly challenging with delays being noted of up to 11 years. 3
Despite predominantly involving the pelvic region, this condition can also manifest in extra-pelvic locations such as the colon. The presentation varies depending on location and can also manifest with symptoms of tenesmus, hematochezia, iron deficiency anemia, epigastric pain, or pneumothorax. These wide-ranging clinical manifestations further make the diagnosis of endometriosis challenging.
Although the gastrointestinal tract is the most common location of extra-pelvic endometriosis impacting up to 37% of the women diagnosed, 4 the rarest presentation among these sites is seen in cecum. Herein, we present this rare case of cecal and appendiceal endometriosis that was initially concerning for a malignancy given that it presented as colonic mass, gastrointestinal bleeding, and symptomatic anemia.
Case Report
A 50-year-old female with past medical history of migraines presented with symptomatic anemia. She initially presented for symptoms of fatigue, shortness of breath, and light-headedness. On physical examination, the patient was tachycardic with abdominal exam suggestive of epigastric tenderness. Laboratory evaluation revealed severe microcytic anemia with hemoglobin 4.2 g/dL, Mean Corpuscular Volume (MCV) 60.4 fL, and serum iron level of 12 µg/dL. Imaging of Computed Tomography abdomen and pelvis (Figure 1) was significant for appendiceal and cecal mass, concerning for neoplasm along with enlarged ileocolic and retroperitoneal lymph nodes. There was also a hypoattenuating mass lesion in the posterior wall of the lower uterine segment/cervix. No demonstratable suspicious or definitive metastatic lesions were noted in the abdomen or pelvis. This raised concern for an underlying gastrointestinal malignancy, and further workup was done for the same. Differentials included adenocarcinoma, hamartomas, colonic polyps, inflammatory bowel disease, neuroendocrine tumors, and infectious causes such as colonic tuberculosis or amebic colitis. Additional workup, such as tumor markers CEA and CA19-9, was within normal limits.
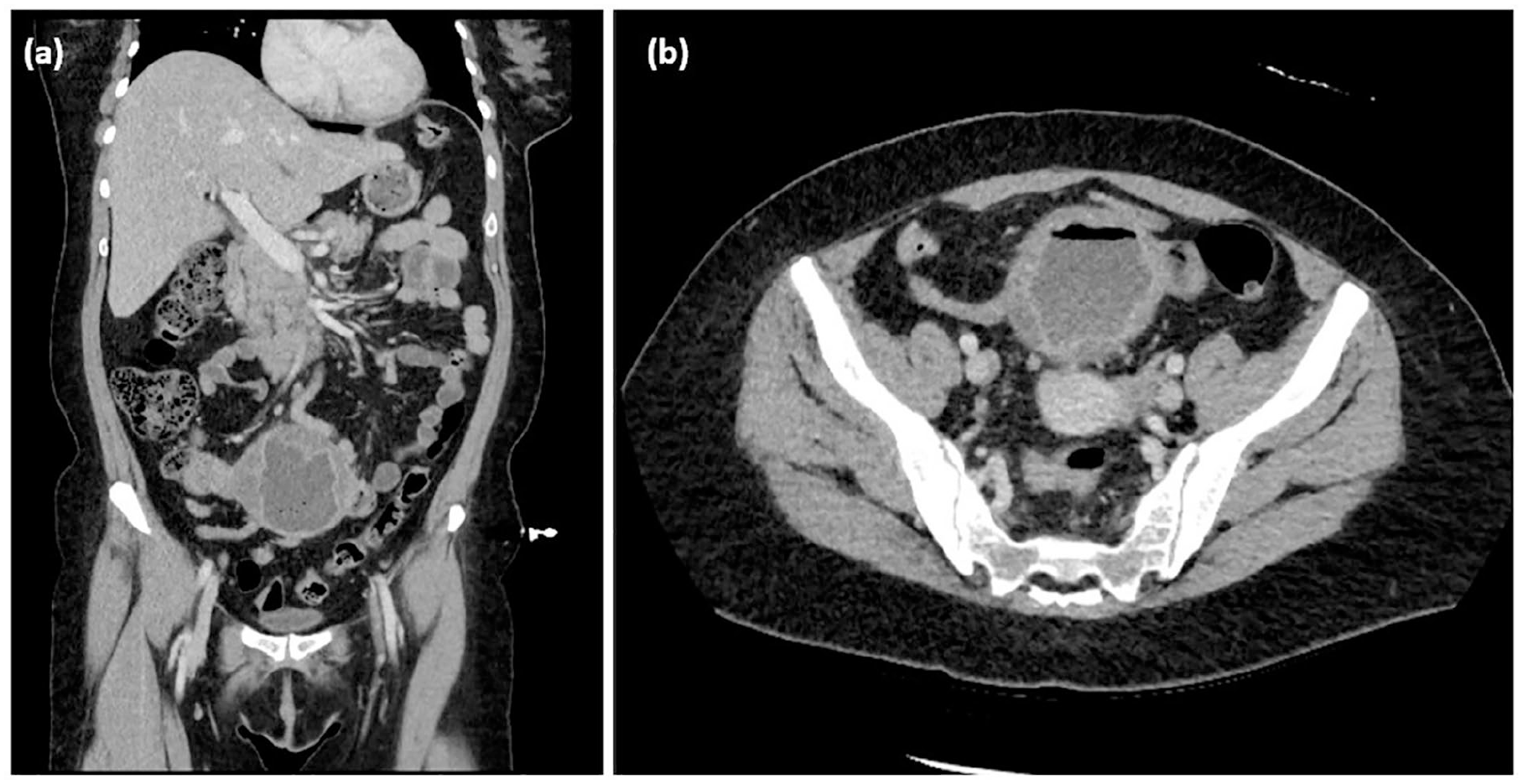
Large appendiceal neoplastic mass lesion in right lower quadrant abdomen with 3.7 solid enhancing component along the proximal aspect toward the cecal base and irregular wall thickening involving the distal appendix. (a) Coronal view (b) Axial view.
The uterine mass was further evaluated with ultrasound, which showed prominent Doppler vascularity and a central cystic/necrotic area. Differentials to be considered included a metastatic deposit in the pouch of Douglas or even an atypical myometrial cervical tumor. Gastroenterology was subsequently consulted for endoscopic evaluation and tissue sampling due to radiologic suspicion of malignancy. Colonoscopy demonstrated a malignant appearing tumor measuring ~3 cm in the cecum/near the appendiceal orifice (Figure 2). It was biopsied and pathology demonstrated some adenomatous changes, but no definitive invasive tumor. Multidisciplinary discussion with colorectal surgery and oncology was held, resulting in a consensus in favor of surgical management due to suspicious radiologic and endoscopic features in addition to severe microcytic anemia.

Malignant appearing tumor measuring ~3 cm in the cecum/appendiceal orifice. Overt extrinsic compression in the rectum. No endoscopic evidence of mass or large polyps in the rectum, sigmoid colon, descending colon, transverse colon, or ascending colon.
Patient underwent exploratory laparotomy; operative findings included a large cecal mass in the mid abdomen with a loop of small bowel and sigmoid colon tethered to the mass, for which a right hemicolectomy, small bowel resection, and sigmoid resection were performed. The findings from the laparotomy demonstrated extensive involvement of the appendiceal wall by endometriosis with formation of cystic lesions and protrusion of endometriosis through the appendiceal orifice to involve the cecum as well.
The pathology of the cecal polyp demonstrated a tubular adenoma and extensive involvement by endometriosis, with entrapped hyperplastic colonic glands in between. Appendiceal cystic mass also demonstrated extensive involvement by endometriosis. Postoperatively, the patient was monitored closely, and her hemoglobin levels gradually improved with iron supplementation and transfusions as needed. She was discharged with a plan for follow-up in the gynecology and gastroenterology clinics.
Discussion
Colonic neoplasms, both malignant (adenocarcinoma, neuroendocrine tumors, gastrointestinal stromal tumor, lymphoma) and benign (adenomatous polyps, hamartomas, hyperplastic polyps, lipoma, fibroma), present as a mass in the colon. 5 However, there are multiple other underlying causes of colonic mass, including infectious, that is, colonic tuberculosis, amebic colitis, actinomycosis, Cytomegalovirus (CMV) colitis, or inflammatory bowel disease. 6 Some other causes include endometriosis, schwannoma, diverticular diseases leading to mass-like inflammatory changes or even a foreign body reaction (Table 1). Although certain clinical presentations may strongly suggest a specific diagnosis, it is essential to consider all possible differentials to ensure a comprehensive evaluation and accurate diagnosis.
Differential diagnoses of a colonic mass.

Abbreviation: GIST, gastrointestinal stromal tumor.
Atypical endometriosis presents in extra-pelvic locations, with the gastrointestinal tract being a common site. The high incidence of endometriotic lesions in the gastrointestinal sites close to the uterus can be explained by the theory of implantation due to retrograde menstruation. 7 In the gastrointestinal tract, endometriosis typically involves the rectosigmoid colon. 8 Cecal and appendiceal endometriosis are exceedingly rare, making up a small fraction (~5%) of the gastrointestinal endometriosis cases. 9
In terms of clinical presentation, most cases of gastrointestinal endometriosis are asymptomatic. 10 Gastrointestinal endometriosis typically involves the serosa layer and hence presents without any overt clinical manifestations. Additionally, pathologies of the cecum often show very delayed clinical presentation, and if symptoms manifest, they tend to be generalized and nonspecific. All these factors add to the diagnostic complexities of extra-pelvic endometriosis based on clinical presentation. Further, gastrointestinal bleeding (as seen in the above case) is a very rare manifestation seen only if the mucosal layer is impacted 11 or due to severe bowel obstruction and ischemia. 12 This made the diagnosis in our patient even more challenging.
The gold standard for diagnosis of endometriosis is laparoscopy. 13 However, in our case, given that colorectal malignancy with occult bleeding was the primary differential, decision for surgical intervention was favored after a multidisciplinary meeting was held. Certain noninvasive modalities such as ultrasound and MRI are often utilized; however, the absence of remarkable imaging findings does not exclude the diagnosis. Extensive research has demonstrated that none of the imaging modalities were able to detect overall pelvic endometriosis with enough accuracy to replace surgery.14,15 Once diagnosed, the first-line management of endometriosis is medical with Non Steroidal Anti Inflammatory Drugs (NSAIDs) and hormonal therapies. However, for patients with contraindications to drug therapies or inadequate response, surgical treatment should be considered. 16
Although traditionally a gynecologic condition, endometriosis is being reframed as a multisystem disorder. 17 It especially becomes vital for gastroenterologists given the high incidence of extra-pelvic manifestations in the gastrointestinal tract. Our case highlights the importance of maintaining a broad differential diagnosis when evaluating patients with gastrointestinal symptoms and anemia. While malignancy should always be a primary consideration, other etiologies, including endometriosis, should be considered, especially in patients without clear risk factors for colorectal cancer. Awareness of the atypical presentations of endometriosis can facilitate timely and accurate diagnosis, avoiding unnecessary treatments and improving patient outcomes.
Footnotes
Authors’ Note
Prior Presentation of Abstract Statement: The abstract for this case was previously presented at American College of Gastroenterology’s Annual Scientific Meeting and Postgraduate Course on October 29, 2024 at Philadelphia, Pennsylvania. P3745—A case of atypical endometriosis presenting as a malignant appearing colonic mass.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.