
Abstract
A 79-year-old Caucasian male was referred to cardiology clinic because the electrocardiogram showed premature atrial complexes and pre-excitation (delta waves) thought to be consistent with Wolff-Parkinson-White (WPW) syndrome. He did not report symptoms of palpitations or syncope. Careful analysis of the electrocardiogram revealed a fascicular-ventricular pathway (FVP) responsible for pre-excitation. Differentiating FVP from WPW syndrome is essential as the risk profile is different with each. Electrocardiographic observations that could help identify the presence of an FVP and its diagnostic, prognostic, and therapeutic implications are presented.
Clinical Presentation
The patient is a 79-year-old Caucasian male with a history of hypertension, asthma, gout, gastroesophageal reflux, hyperthyroidism (treated), hypercalcemia, and bilateral hip replacement, who was seen by his primary-care physician for evaluation of left hip pain. He had no history of heart disease and denied palpitations, syncope, chest pain, and shortness of breath.
On physical examination, he was noted to have an irregular heart rhythm. The cardiovascular examination was otherwise unremarkable. An electrocardiogram showed pre-excitation (delta wave) and premature atrial complexes (PACs; Figure 1). He was referred to the cardiology clinic for further evaluation of Wolff-Parkinson-White (WPW) syndrome.

12-lead electrocardiogram. Sinus rhythm, PACs, pre-excitation, delta wave (red arrow), and right bundle-branch block.
Analysis of the Electrocardiogram
The 12-lead electrocardiogram shows sinus rhythm, and the QRS complexes show pre-excitation and right bundle-branch block morphology. Two PACs are also present. The first PAC, which has a short coupling interval of 480 ms, has a longer PR interval than the sinus rhythm, yet the pre-excitation does not change. The second PAC which has a longer coupling interval of 560 ms, has a shorter PR interval with no change in pre-excitation (Figure 2). The P waves are fully inscribed, and there is a PR segment prior to the onset of the delta wave. These observations suggest a diagnosis of fascicular-ventricular pathway (FVP).

Leads V1-V6. The coupling interval of the first PAC (A) is 480 ms. The PR interval is prolonged (translucent circle) and pre-excitation persist without any change in QRS width. The second PAC (B) coupling interval is 560 ms, and the delta wave is unchanged. The QRS duration during sinus rhythm and following the PAC is 120 ms.
The width of the QRS complex is the same after the sinus beats and the PACs. The absence of an S wave following the PACs and an increase in amplitude of the QRS complexes gives an impression that the QRS is wider following PACs. However, the width of the QRS complex is 120 ms within both sinus rhythm and following PACs.
Discussion
Fascicular-ventricular pathways originate from the fascicles—such as the His bundle or bundle-branch—and insert into ventricular myocardium 1 (Figure 3). On the surface electrocardiogram, the P waves are generally complete before the pre-excitation begins because the pre-excitation occurs after His bundle activation. The pre-excitation (delta wave) begins after the P wave is fully inscribed. In pre-excitation (WPW syndrome) due to an antegrade conducting atrioventricular (AV) accessary pathway that connects the atrial and ventricular myocardium across the AV ring, the electrical impulse travels through the accessory pathway and reaches the ventricle before the PR segment is fully inscribed. 2
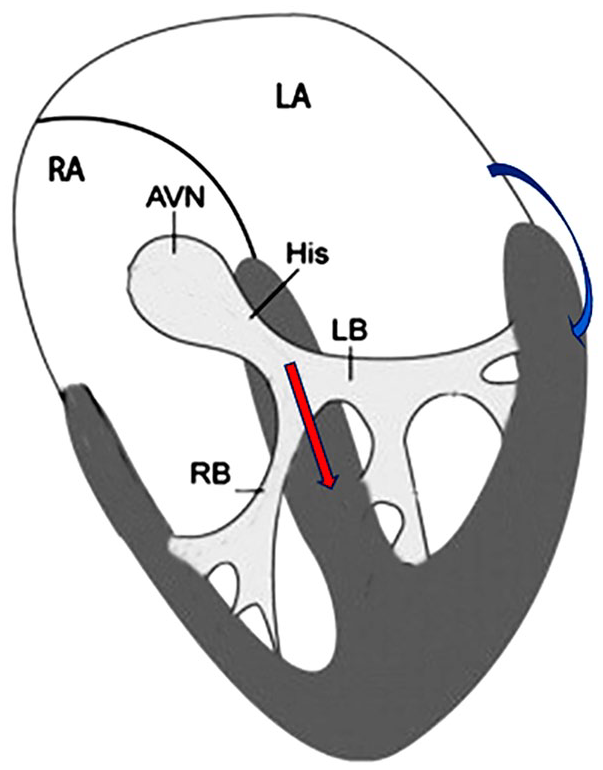
Fascicular-ventricular connections (red arrow) connects one of the fascicles of the conduction system to the ventricular myocardium thus resulting in delta waves (pre-excitation). As this connection is distal to the AV node the P wave and the PR interval are fully inscribed before the delta wave begins. The AV connections responsible for WPW are from atrium to the ventricular myocardium (blue arrow).
Differentiating Pre-excitation Due to Fascicular-Ventricular Connections From Wolff-Parkinson-White
A feature of FVP which is not seen in typical AV accessory pathway is the same degree of pre-excitation with a longer PR interval. 3 In our patient, an increase in the PR interval as seen in the first PAC is not compatible with pre-excitation due to accessory pathway across the AV ring. This can only be seen in connections distal to the AV node and His bundle. The FVP, due to its location, shares some electrocardiographic similarities with midseptal or anteroseptal AV accessory pathways. 4
Diagnostic Maneuvers
Adenosine testing can be used to differentiate if pre-excitation is a result of FVP or AV accessory pathway (WPW syndrome). During sinus rhythm, rapid adenosine infusion (i.e., 0.3-0.4 mg/kg intravenous bolus, maximum dose 12 mg) with continuous 12-lead electrocardiographic monitoring a diagnosis of WPW syndrome is established if the QRS morphology changes due to full pre-excitation without a change in the PR interval or AV block. Conversely, FVP is established if AV block occurs resulting in nonconducted P waves with no change QRS waveform, or if the PR interval is prolonged by ≥40 ms with no change in QRS morphology.
If PACs are detected, as in our patient, a diagnosis can be established based on the change in the QRS waveform; a wider QRS complex is indicative of WPW syndrome, whereas the QRS complex is unaltered with FVP. In addition, with WPW syndrome, the delta wave becomes more prominent when the heart rate is slower as a result of decreased AV conduction. Hence the QRS waveform varies with heart rate in WPW syndrome, whereas it is not affected by heart rate with conduction through an FVP.
Ambulatory electrocardiographic monitoring for 24 to 48 h may help identify the change in pre-excitation or lack thereof, with changes in the heart rate or occurrences of PACs.
Prognostic and Therapeutic Implications
Differentiating FVP from WPW syndrome is essential as the risk profile is different with each. Fascicular-ventricular pathways usually do not participate in re-entrant tachycardia; therefore, the patient remains asymptomatic. There is no risk of tachycardia episodes or sudden death in patients with delta waves due to FVP. Conversely, the presentation and prognosis of WPW syndrome depends on the conduction properties of the accessory pathway. A rapid antegrade conduction through the accessory pathway, bypassing the AV node which is responsible for rate control, may result in ventricular rates in excess of 240 bpm resulting in ventricular fibrillation and sudden cardiac death.
Children are often engaged in school-based cardiovascular programs in which an electrocardiogram is obtained. Those who are “diagnosed” as having WPW syndrome and have a QRS width ≤120 ms are likely to have FVP rather than WPW. Adenosine testing should be considered to clarify the diagnosis. Children with pre-excitation due to FVP do not require restrictions of physical activity nor do they require electrophysiologic studies or radiofrequency ablation. 5
Conclusion
This patient has clinical and electrocardiographic manifestation of pre-excitation suggestive of FVP. No further evaluation or treatment, for this pre-excitation, is warranted.
Footnotes
Author Contributions
The authors participated in various stages of this project by collecting clinical information, data, and preparation of the illustrations, research, and writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.