
Abstract
Secundum atrial septal defect (ASD) is the most common type of ASD. Symptoms including dyspnea on exertion usually manifest in the third and fourth decade of life. The transcatheter closure is the treatment of choice for secundum ASD. The transfemoral venous approach has been the mainstay. However, this approach can be challenging or impossible in patients with congenital absence or interruption of the inferior vena cava (IVC). The latter has been reported in patients with situs ambiguus and inversus. In this patient population, other forms of venous access such as the transjugular or transhepatic approach are used. We present a unique case of symptomatic secundum ASD in a patient who was incidentally found to have situs ambiguus with a left-sided intact IVC. An initial attempt at the ASD closure via the transfemoral approach was unsuccessful due to acute angulation. A repeat attempt was successful via the transhepatic approach with the guidance of real-time ultrasound, transesophageal echocardiogram, and the involvement of an interventional radiologist. The procedure was well tolerated without any complications. Repeat transthoracic echocardiogram with agitated saline the day after the procedure was negative for interatrial shunting.
Introduction
Secundum atrial septal defect (ASD) accounts for 75% of all ASD cases. 1 Patients are usually asymptomatic until the third and fourth decade of life when significant left-to-right atrial shunting overwhelms the right side of the heart and pulmonary circulation. 1 The indications for ASD closure include significant right heart enlargement regardless of symptoms, a net left-to-right shunt sufficiently large enough to cause physiologic sequelae (such as a total pulmonary blood flow that is at least 1.5 times systemic flow) without cyanosis at rest or during exercise, a pulmonary vascular resistance that is less than one-third of the systemic vascular resistance, and a systolic pulmonary artery pressure that is less than 50% of systemic vascular resistance. 2
Transcatheter closure mostly via the transfemoral approach is considered the treatment of choice for secundum ASD.3-6
Situs ambiguus (also known as heterotaxia) refers to an abnormal distribution of the thoracic and/or abdominal viscera organs in a manner that does not totally conform with situs inversus. 7 It has an incidence of 1:10 000 births and it is associated with congenital heart defects (CHD) with a coincidence as high as 100%. 7 Commonly associated CHDs include ASD, partial anomalous pulmonary venous return, and a common atrioventricular canal. 7
Patients with situs ambiguus commonly have an interrupted IVC with azygous or hemiazygous continuation. 7 However, we present a unique case of secundum ASD in a patient who has situs ambiguus with a left-sided intact inferior vena cava (IVC). This warranted the transhepatic approach due to technical difficulties encountered during the transfemoral approach.
We present a case of symptomatic secundum ASD in a patient who was incidentally found to have situs ambiguus with a left-sided intact IVC. It was presented as a virtual poster at the American College of Cardiology Conference 2020 and the abstract was published in the Journal of the American College of Cardiology in March 2020. 8
Case Presentation
The patient is a 45-year-old woman with a reported past medical history of asthma due to recurrent chest tightness and dyspnea on exertion. Laboratory investigation was notable for an elevated brain natriuretic peptide of 621 pg/mL. Chest radiograph was remarkable for prominent pulmonary interstitium and vasculature. Electrocardiogram revealed normal sinus rhythm with nonspecific ST-T wave changes. A transthoracic echocardiogram (TTE) showed moderately enlarged right atrium (RA), right ventricle (RV), an elevated right ventricular systolic pressure (RVSP), and diastolic flattening of the interventricular septum consistent with RV volume overload. The RA area was 18.76 m2 and the RVSP was approximately 32 mm Hg. The right atrial pressure, right ventricular systolic function (evaluated objectively by the tricuspid annular plane systolic excursion [TAPSE]), left atrial, ventricular volumes, and pressures were within normal limits. A bubble study with agitated saline was remarkable for severe left-to-right interatrial shunting indicating an ASD. A subsequent transesophageal echocardiogram (TEE) confirmed a secundum ASD measuring 2.2 by 1.8 cm (Figure 1). A computed tomography chest pulmonary embolism (CT-PE) was obtained to evaluate for the presence of PE due to her elevated RVSP and enlarged RV. This was negative for PE; however, it was remarkable for the presence of a situs ambiguus abdominal anatomy. The liver was in the left upper quadrant while the spleen and stomach were in the right upper quadrant. The patient was scheduled for an outpatient ASD closure. However, she was lost to follow-up for approximately 3 years. During this period, she presented to multiple EDs due to similar symptoms and was repeatedly treated for asthma exacerbation.

From left to right, mid-esophageal and bicaval views of transesophageal echocardiogram revealing the ASD (arrows), mid-esophageal view after deployment of the ASO device (arrows) without residual shunting, and a 3D view (far right image) of the ASO device (arrow) occupying the ASD defect.
She presented to our cardiology clinic due to persistent symptoms, and an ASD repair was planned. During the procedure, there was difficulty advancing the guidewire from the right femoral vein through the IVC into the RA. A subsequent venogram (Figure 2) at the level of the femoral vein was notable for a left-sided IVC that reconnected with the RA at the hepatic level. A Cobra catheter was successfully advanced into the RA via the left-sided IVC and crossed the ASD with a Rosen wire positioned into the right upper pulmonary vein. However, due to acute angulation, the Amplatzer septal occluder (ASO) could not be advanced into the left atrium, and the procedure was aborted. The procedure was rescheduled with a plan for an alternative venous access. However, the patient was yet again lost to follow-up for a year after which she again presented to our ED with worsened symptoms.

From left to right, venogram of the initial transfemoral approach revealing the anomalous course of the inferior vena cava and its connection with the right atrium from the left side indicated by the trajectory of the guidewire (arrows) which in turn courses through the atrial septal defect into the right upper pulmonary vein.
On repeat TTE, her RA area and RVSP had further increased to 27.42 m2 and 44 mm Hg, respectively. Right ventricle area at end diastole was 35.60 m2. On repeat TEE, the ASD measured 2.5 by 1.6 cm. This time, the procedure was performed under TEE guidance. Percutaneous transhepatic venous access was obtained by interventional radiology via real-time ultrasound guidance. The right hepatic vein (Figures 3 and 4) was accessed using a 21-gauge needle. A 10 French sheath was then placed under fluoroscopic guidance over an Amplatz stiff guidewire. The sheath was upsized to 12 French. Heparin was then administered to keep the activated clotting time >250 seconds. The left upper pulmonary vein was accessed using a multipurpose (MP) catheter and the Amplatz wire. The 12 French sheath was then advanced over the catheter and wire into the left atrium. After careful 3D sizing of the ASD, a 28-mm ASO was loaded onto its delivery cable and sheath, was flushed of air, and advanced into the left atrium. The left-atrial and right-atrial disks were then released in standard fashion. Once an appropriate and secure position was assured by TEE and fluoroscopy, the ASO was released from its delivery cable. At the conclusion of the procedure, heparin was reversed with protamine, and the transhepatic tract was closed using a vascular plug by interventional radiology. The patient tolerated the procedure well with no immediate complications. Repeat echocardiogram with agitated saline the day after the closure was negative for interatrial shunting.
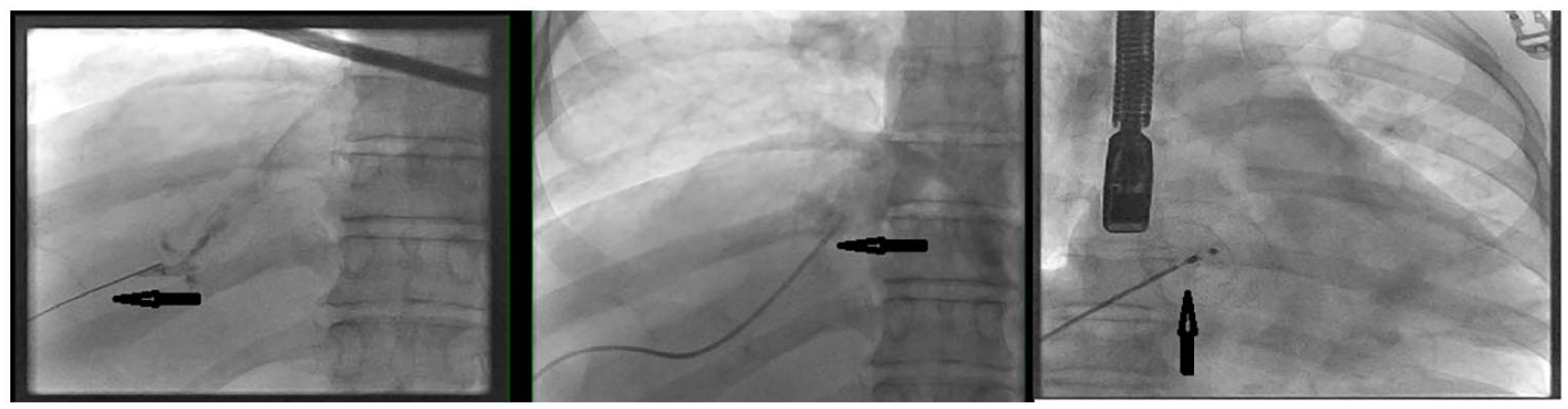
From left to right, venogram of the subsequent transhepatic approach showing the guidewire access into the inferior vena cava from the hepatic vein (arrows) and eventual deployment (third image) of the Amplatzer septal occluder device (arrow) within the atrial septal defect.
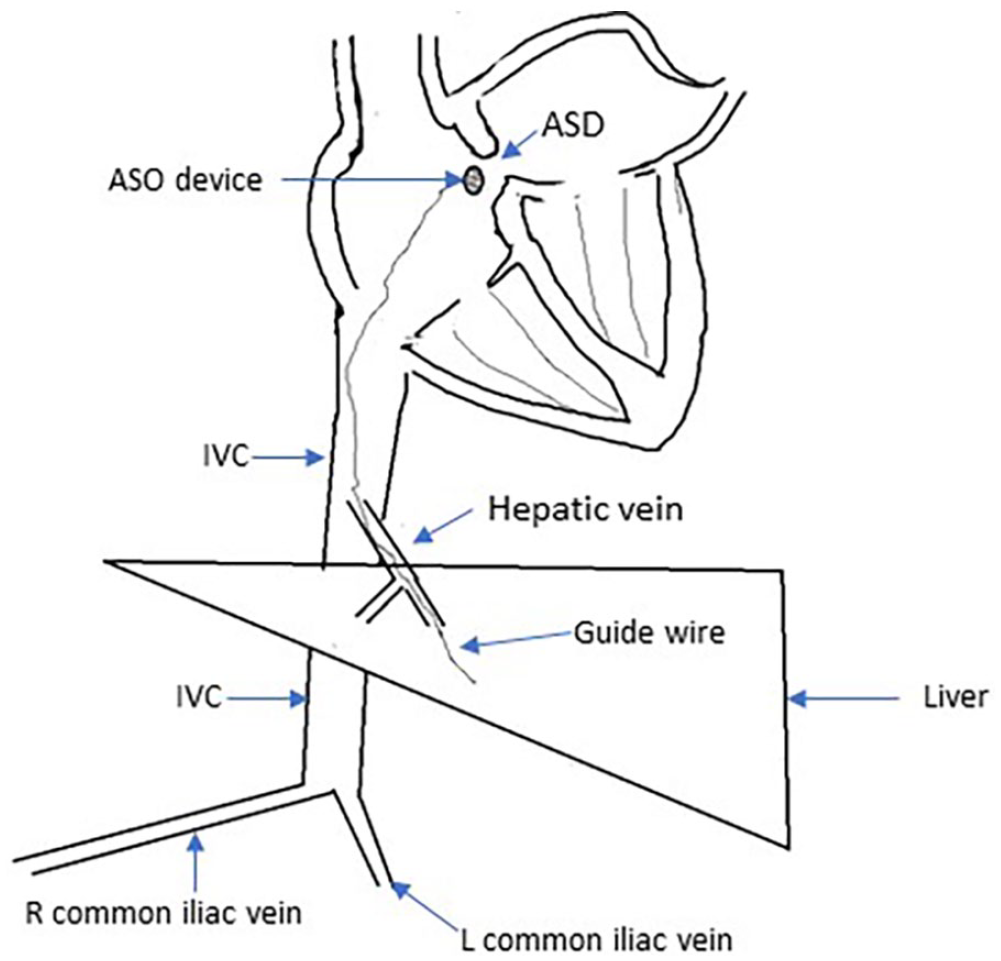
Pictorial depiction of the transhepatic access demonstrating a left-sided liver and IVC, a longer right common iliac vein, and the guidewire access to the IVC via the hepatic vein.
Discussion
The indications for ASD closure in this patient include her worsening functional capacity and the echocardiographic evidence of RA and RV volume overload listed above.
Congenital abnormalities of the IVC that have been reported in some patients undergoing transcatheter secundum ASD repair are IVC absence and interruption with azygous continuation.1,5,6,9 However, to the best of our knowledge, a similar case of transcatheter secundum ASD closure in a patient with situs ambiguus and a left-sided IVC has rarely been reported in the literature.
The transfemoral access of the IVC is the mainstay in percutaneous ASD closure.3-6 This is because of the shorter procedural time and a lower risk of procedural complication compared with other types of venous access. 5 However, this form of vascular access becomes challenging or impossible in patients with congenital anatomic defects of the IVC.3-6 In this patient population, other forms of venous access including the transjugular or transhepatic access are preferred.1,4,6,10 Although there is paucity of data comparing these forms of venous accesses in terms of efficacy, procedural time, and safety,1,4,6,10 we opted for the transhepatic approach because it offers a less complicated path for the guidewire navigation and delivery of the ASO device. 5 In addition, difficulties maintaining the guidewire in the left upper and lower pulmonary veins and the possibility of air embolism as a complication are associated with the transjugular approach.5,6,10
Complications of the transhepatic approach such as retro/intraperitoneal bleeding, haemobilia, gall bladder perforation, and pneumothorax have been reported.1,6,10 We were able to limit the possibility of these with the guidance of real-time ultrasound, TEE, and the involvement of an interventional radiologist.
Another option that we considered was surgical closure of the ASD; however, we decided for the transcatheter closure due to the shorter procedural time, lower length of stay, and risks of complication. 11 In addition, this patient did not meet any indications for surgical closure agreed by experts in the literature.12,13 These are ASD diameter >38 mm with or without deficient posteroinferior rim, ostium primum and sinus venosus ASD, associated cardiac defects such as the presence of an aneurysmal interatrial septum, and a total anomalous pulmonary venous return.12,13
Conclusions
This is the first case of the transhepatic approach to closing a secundum ASD in a patient with situs ambiguus with a left-sided intact IVC. With the use of real-time ultrasound, TEE guidance, and the expertise of an interventional radiologist, this approach is reliable and can be safe of complications in cases where the transfemoral approach becomes anatomically challenging or impossible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.