
Abstract
Plasmacytosis is the abnormal proliferation of plasma cells in tissue, bone, blood, or exudates. Mucous membrane plasmacytosis is a rare form of plasmacytosis that is usually idiopathic in nature. A 68-year-old female underwent a diagnostic and therapeutic esophagogastroduodenoscopy, which revealed a friable antral erythematous gastric fold and a gastric polyp. Subsequent pathological testing was positive for diffuse polyclonal plasma cell proliferation, which was suggestive of a gastric plasmacytosis. In this article, we report a rare presentation of mucous membrane plasmacytosis.
Introduction
Plasmacytosis is a condition in which there is an unusually large proportion of plasma cells in tissues, exudates, or blood. Mucous membrane plasmacytosis is a rare entity and is usually idiopathic in nature. It consists of a dense plasma-cell infiltrate of the mucous membranes. 1 Plasmacytosis can progress to plasma cell neoplasms, which are classified as mature B-cell neoplasms.
According to the World Health Classification, plasma cell neoplasms include multiple myeloma, plasma cell leukemias, solitary plasmacytomas of the bone, and extramedullary plasmacytomas. 2 The plasma cell infiltration may be so expansive and diffuse that one may suspect an extramedullary plasmacytoma (EP). 3 EP are solitary lesions composed of monoclonal plasma cells that are found in soft tissues without further systemic involvement. EPs are responsible for <5% of all plasma cell neoplasms and are more frequently found in the head and neck region, otherwise known as the upper aerodigestive tract with the stomach being the second most common location.2,4 Similarly, mucous plasmacytosis is also found in the aerodigestive tract; however, to date, no cases of gastric mucosa plasmacytosis has been described. 1
Symptoms of mucous plasmacytosis and plasmacytomas both tend to be nonspecific. They can range from constitutional symptoms such as weight loss, dysphagia, oral and abdominal pain to more severe symptoms such as gastrointestinal bleeding. Radiology and imaging studies are also usually inconclusive; thus, pathological testing is often necessary to diagnose and distinguish between plasmacytosis and plasma cell neoplasms.
Case Report
A 68-year-old female with a past medical history of iron deficiency anemia presented to the emergency department at our institution due to shortness of breath at rest and on exertion. On admission, her hemoglobin was found to be 3.7 g/dL, mean corpuscular volume of 67 fL, ferritin of 2 µg/L, and a transferrin saturation of 2%. Subsequently, she was admitted to the medical intensive care unit due to symptomatic iron deficiency anemia and the gastroenterology team was consulted. On further questioning, the patient denied hematemesis, melena, hematochezia, and nonsteroidal anti-inflammatory drug use. Her fecal occult blood test was negative, and a direct rectal examination was negative for blood, melena, and stool on a gloved finger. The hemoglobin stabilized to 8.2 g/dL after receiving a total of 3 units of packed red blood cells. An esophagogastroduodenoscopy (EGD), push enteroscopy, and colonoscopy were performed. The colonoscopy was positive for internal hemorrhoids, and no polyps or other abnormalities were seen. A friable antral erythematous gastric fold and 2-mm gastric polyp were observed on EGD and push enteroscopy. Pathological examination revealed severe chronic inactive gastritis with diffuse plasma cell infiltration of the lamina propria consistent with plasmacytosis. Immunohistochemistry staining was performed and was consistent with diffuse polyclonal plasma cell proliferation, which was suggestive of a chronic inflammatory process and gastric plasmacytosis as seen in Figures 1 and 2. Further antibody testing was performed and was found to be positive for CD20 in the follicles, CD38 and CD138 in the lamina propria, as well as kappa and lambda positive as seen in Figures 3 and 4.

Demonstrates the gastric mucosa, lamina propria is expanded with lymphoplasmacytic infiltrates (40×).
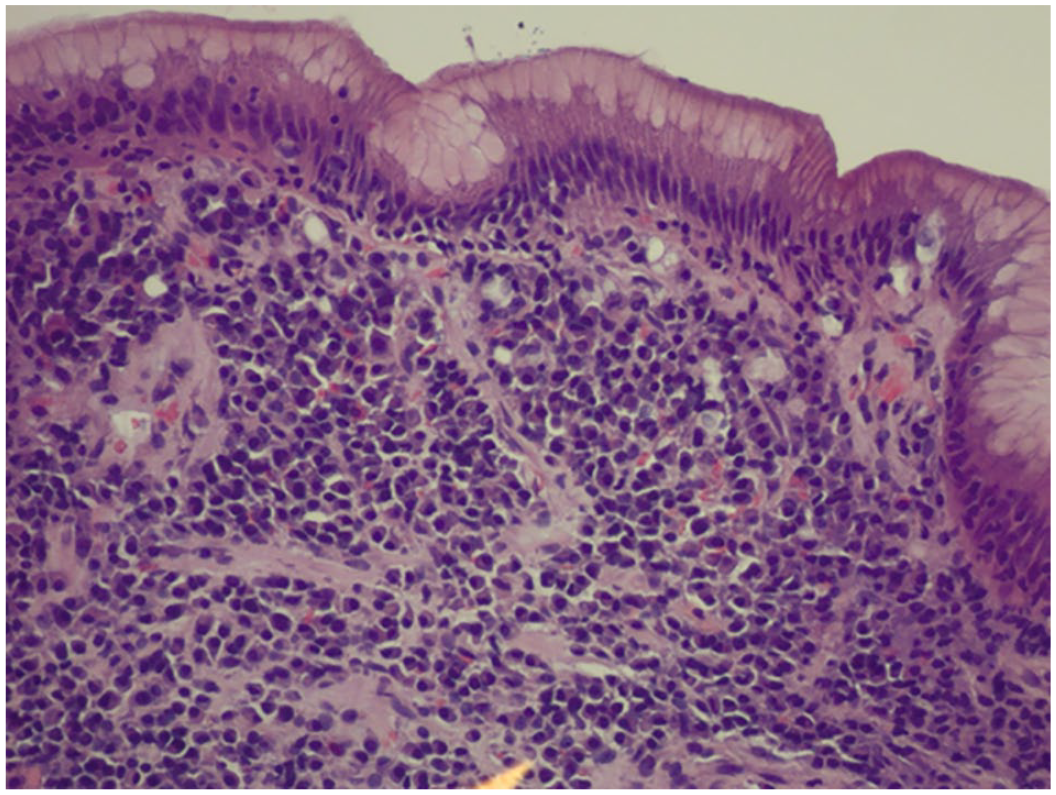
Demonstrates the gastric mucosa, lamina propria is expanded with lymphoplasmacytic infiltrates (200×).

Demonstrates the predominant plasma cells highlighted by CD138 immunostain.
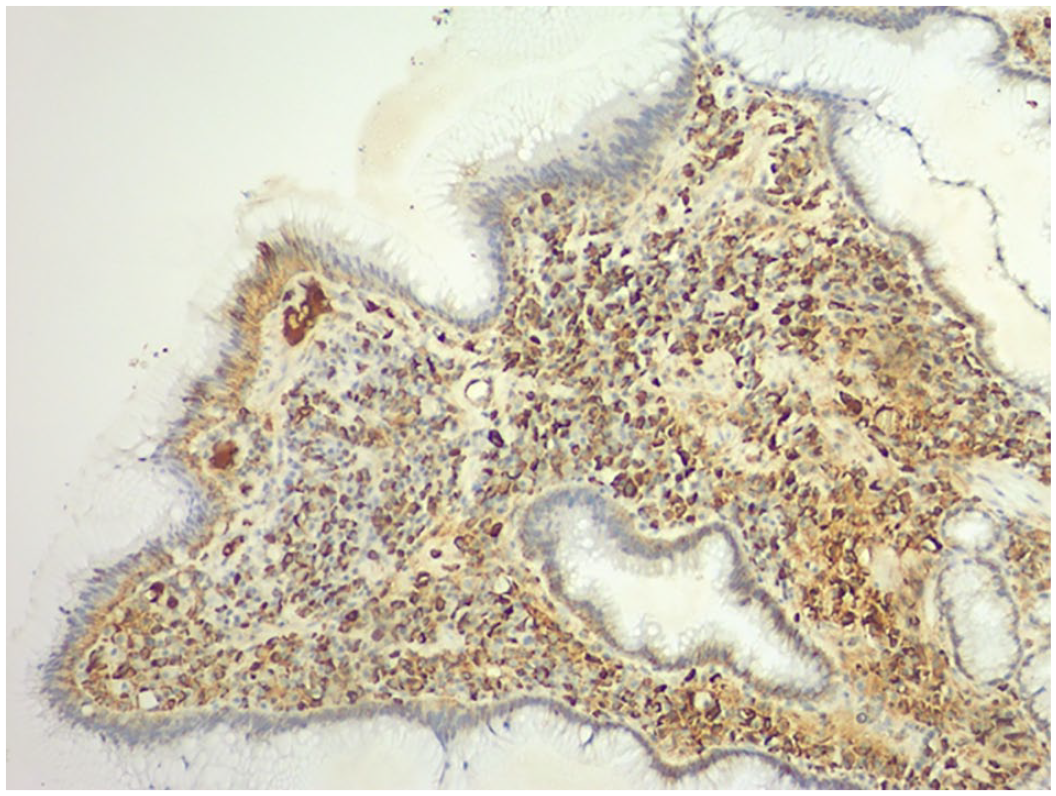
Plasma cells are highlighted by both kappa and lambda immunostains, implying gastric plasmacytosis.
Discussion
Mucous plasmacytosis is rare but is usually benign and tends to have a good prognosis. Since they usually present with nonspecific clinical and radiographic findings, it often leads clinicians to a different diagnosis. On imaging, a polypoid lesion or homogeneous concentric gastric wall thickening can be seen in some instances, which is commonly read as a gastrointestinal stromal tumor or lymphoma. Even on endoscopy, one may only see a thickened and bulging gastric wall since the origins are mucosal. This often leads to a diagnosis of gastric adenocarcinoma. Similarly in our case presented here, the tumor was observed as an erythematous protruding gastric fold and 2-mm gastric polyp. Thus, pathological examination and an immunohistochemistry panel are needed to make the diagnosis, like in our case. 2
The tumor morphology on biopsy was described as “sheets of mature and immature plasmocytes in the lamina propria, with high mitotic count and absence of lymphoepithelial lesions.” This pathology will bring clinicians to 2 diagnoses: neoplasms, such as plasmacytomas and lymphomas, versus plasmacytosis. In our case, the pathology was exactly that with severe chronic inactive gastritis and diffuse plasma cell infiltration of the lamina propria consistent with plasmacytosis. The morphological findings along with an immunohistochemistry panel further supports the diagnosis. Commonly, immunohistochemistry for plasmacytomas will be negative for CD20, CD79a, CD10, and Bcl-2 and positive for CD138, EMA, MUM1, and lambda chains. 5 However, in plasmacytosis, as it is polyclonal in nature, immunohistochemistry is usually positive for both Kappa and lambda chains. 1 Further supporting our diagnosis as our patient was positive for CD20 along with CD138, CD38, Kappa, and lambda chains. If immunochemistry is still inconclusive, gene arrangement therapy can be performed to distinguish between mucous membrane plasmacytosis and plasmacytomas. 1
Mucous membrane plasmacytosis is more common in men; however, in our case, we present a 68-year-old female.3,5 Furthermore, the average age of GPs found in men is 54 to 55 years. 3 Ferreiro et al conducted a case series of 9 patients with mucous membrane plasmacytosis. Although different from our case, as all 9 patients had plasmacytosis within the oral mucosa, they reported that 7 out of the 9 had no progression or regression of the disease. 3 They observed the long-term survival to be good, with one patient living for 16 years after diagnosis. However, Fogarty et al discussed a few cases in which the disease progressed to the larynx from the oral mucosa. Some cases even got so severe that it resulted in airway obstruction requiring a tracheostomy. 6
The etiology of plasmacytosis is still unknown, and to date, there is no reported effective treatment modality. In the case described by Fogarty et al, the plasmacytosis progressed despite the patient receiving both chemotherapy and radiation. 6 In study previously described by Ferreiro et al, treatment with antibiotics, steroids, and surgical resection were all ineffective in eradicating the disease with again 2 of the patients requiring tracheostomy. 3 In contrast, Jones et al described a case of 52-year-old woman with oral mucous membrane plasmacytosis who, much to their surprise, responded rapidly to topical clobetasol propionate treatment. 7
Gastric plasmacytosis is a rare form of mucous membrane plasmacytosis, as most known cases occur in the oral cavity or the larynx. This type of proliferation is significant not only for its rarity but also in its risk of progressing to plasma cell neoplasms and that the etiology and appropriate medical management is still unknown. Hence, it is imperative for it to be on a physician’s differential along with the gastric tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures were performed in accordance with the ethical standards established in the 1964 Declaration of Helsinki and its subsequent amendments.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article. This study does not contain identifying information of the patients.