
Abstract
In this report, we describe a case of atypical neuroleptic malignant syndrome (NMS) presenting with an isolated lesion in the splenium of the corpus callosum (ILSCC). There is a paucity of information regarding this topic within the literature and only 7 previous case reports have been published at the time of writing. To our knowledge, this case report is also the first to describe an atypical NMS variant in the context of an ILSCC. In this report, we describe the important considerations in formulating differential diagnosis for ILSCC and are the first report to propose a possible pathophysiological mechanism relating ILSCC with NMS.
Introduction
Isolated lesions in the splenium of the corpus callosum (ILSCC) are an uncommon radiographic entity with an estimated prevalence between 0.6% and 3.0%.1,2 ILSCCs are most commonly associated with a clinical presentation of delirium and have a broad differential diagnosis. 2 With regard to neuroleptic malignant syndrome (NMS), recent literature has suggested a disease spectrum model with emphasis on identifying prodromal and atypical NMS variants in order to improve disease outcomes.3-5 Considering the estimated incidence of NMS is between 0.01% and 0.02%, the co-occurrence of ILSCC and NMS is either exceedingly rare or an underrecognized clinical phenomenon. 6 At the time of writing, only 7 publications exist documenting ILSCC in the context of NMS, the first of which was published in 2009.7-13 In this report, we are the first to describe a case of atypical NMS presenting with an ILSCC. We are also the first to publish a case report to postulate a possible pathophysiological relationship between the development of ILSCC and NMS.
Case Presentation
The patient was a 45-year-old male with a past medical history of intermittent asthma, hypertension, and type 2 diabetes mellitus who presented to the emergency department (ED) via ambulance status post fall in the context of phencyclidine (PCP) intoxication. Initially in the ED the patient was urinating on the floor, attempting to fight staff members, and uncooperative with examination. Intravenous haloperidol 5 mg and midazolam 4 mg were administered for agitation, after which the patient was able to tolerate medical evaluation and management. Additional history was limited at this time given the patient’s intoxicated state. The patient was unable to participate in a formal review of systems given his altered mental status (AMS). Initial vital signs were blood pressure 146/83 mm Hg, pulse 104 beats per minute, temperature 98.4 °F, respiratory rate 18 breath per minute, and oxygen saturation 98%. Physical examination was grossly normal aside from a 3 cm stellate forehead laceration. Apart from a leukocytosis of 15 K/mm3, complete blood count, and comprehensive metabolic panel were within normal limits. Pertinent normal laboratory test results included a sodium of 140 mmol/L, blood urea nitrogen of 15, and a creatinine of 0.87 mg/dL. Urine drug screen was positive for benzodiazepines and PCP. Urinalysis was positive for only bacteria and nitrites along with 6 to 9 epithelial cells per high-power field suggesting possible contamination. Urine cultures were not obtained. Computerized tomography (CT) imaging demonstrated left zygomaticomaxillary complex fractures without acute intracranial pathology. CT imaging of the patient’s cervical spine did not demonstrate any acute pathology. While in the ED, the patient’s forehead laceration was sutured. The patient was admitted to an inpatient medicine unit for further management of his AMS and facial fracture.
On admission, the patient was somnolent, oriented only to self, and unable to engage with the admission assessment. An extensive AMS workup was completed, which included ammonia, vitamin B12 and folate levels, thyroid-stimulating hormone, blood cultures, C-reactive protein, repeat comprehensive metabolic panel/complete blood count, syphilis screen, and repeat head CT. Aside from a mildly elevated C-reactive protein of 2.6 mg/dL and leukocytosis of 14.2 K/mm3 the remainder of the patient’s laboratory test results was within normal limits. Specific laboratory tests of interest pertinent to a delirium workup returned within normal limits as follows: ammonia 15 µmol/L, thyroid-stimulating hormone 0.4, vitamin B12 576 pg/mL, and folate 22.9 ng/mL. The differential diagnosis for the patient’s AMS remained wide, so he was placed on the Clinical Institute Withdrawal Assessment for Alcohol protocol and started on intravenous thiamine as a history of alcohol use could not be ruled out. The patient was also given a 3-day course of intravenous ceftriaxone considering equivocal urinalysis findings. Plastic surgery was consulted and recommended nonemergent elective repair of the facial fractures, but treatment was deferred as the patient remained altered and could not consent to the procedure.
Per family collateral, the patient worked part-time as a mechanic, lived alone, performed all activities of daily living independently, and did not have any history of neurologic or psychiatric disease. Family was unable to provide any additional information regarding the patient’s substance use. The patient did not receive any additional lorazepam per Clinical Institute Withdrawal Assessment for Alcohol protocol or for vital sign abnormalities consistent with alcohol withdrawal. Aside from his tachycardia on initial presentation in the ED, the patient did not demonstrate tachycardia after admission to the inpatient medicine unit. On the third hospital day, the patient’s AMS persisted, and neurology was consulted and evaluated the patient for additional causes of encephalopathy.
On the consulting neurologist’s initial examination, the patient remained lethargic, oriented only to self, unable to follow complex commands, and hypophonic with increased speech latency. No focal cranial nerve deficit was appreciated; however, the patient exhibited hypertonicity with significant oppositional paratonias in all 4 extremities along with bilaterally upgoing plantar reflexes. Magnetic resonance imaging (MRI) and electroencephalography (EEG) were ordered per neurology recommendations. EEG did not demonstrate epileptiform activity or generalized slowing. However, MRI revealed a restricted diffusion/focal hyperintensity within the splenium of the corpus callosum on diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR) images, respectively. MRI findings on FLAIR, DWI, and ADC (apparent diffusion coefficient) are highlighted in Figure 1. In consideration of the patient’s recent exposure to neuroleptics, persistent encephalopathy, and significant oppositional paratonias, the possibility of an atypical variant of NMS contributing to the patient’s delirium was likely. Despite the likelihood of atypical NMS, in considering the wide differential diagnosis of callosal lesions the probability of the MRI lesion representing a new infarct remained. Therefore, the patient was placed on standing aspirin 325 mg along with atorvastatin 40 mg daily. CT angiography of the head and neck was completed and was unremarkable. The patient was also started on standing benztropine 1 mg twice daily for atypical NMS. Of note, lorazepam was not used as there was concern for additional central nervous system depression in an already somnolent and delirious patient.

Images A, C, and E represent DWI, FLAIR, and ADC results, respectively, on initial imaging. Images B, D, and F represent DWI, FLAIR, and ADC results, respectively, 11 days after initial imaging. FLAIR, fluid-attenuated inversion recovery; DWI, diffusion-weighted imaging; ADC, apparent diffusion coefficient.
By the seventh hospital day, the patient became more alert, had improved orientation, was able to complete 2 step commands with prompting, and had reduced cogwheeling on examination. Additionally, the patient’s leukocytosis had down-trended to 13.2 K/mm3. The scheduled benztropine was also discontinued. The patient did not require any physical restraints or tranquilizers for agitation after admission. The patient’s MRI was repeated 11 days after initial imaging, which redemonstrated the corpus callosum splenium hyperintensity on FLAIR imaging and without restricted diffusion on DWI. The patient was instructed to repeat imaging as an outpatient to confirm the diagnosis of subacute callosal infarct versus transient splenial lesion of another etiology. The patient was recommended to be discharged to a rehabilitation facility to further manage his physical deconditioning and was subsequently lost to follow-up.
Discussion
At the time of writing, this is only the eighth documented case demonstrating concurrent ILSCC and NMS pathology.7-13 NMS has phenotypic heterogeneity and should be viewed on a disease spectrum rather than as a discrete syndrome. 3 Fever and autonomic instability are usually late findings in NMS, which can make identifying early presentations of NMS especially challenging. 14 Consequently, a common disease variant lacking core malignant features has been conceptualized in the literature as atypical NMS. 5 However, there is considerable uncertainty whether atypical NMS represents a distinct pathology or a prodromal phase destined to evolve with malignant features. Some authors have even proposed a multi-staged disease model of NMS in order to better account for atypical presentations. 4 Of note NMS is a clinical diagnosis and specific laboratory or imaging results are not required to confer a diagnosis. 15 For instance, our patient’s EEG was without epileptiform activity or generalized slowing, but positive EEG findings are not required to diagnose NMS or delirium. In fact, a recent review suggested EEG testing may have a false positive and false negative rate as high as 20% when evaluating delirium. 16 Therefore, despite being afebrile during this hospitalization, the diagnosis of atypical NMS can still be rendered in our patient considering significant oppositional paratonias and altered mental status in the context of recent neuroleptic exposure. Given our patients atypical NMS variant, an intensive care unit level of treatment including dantrolene was not required, especially in the absence of malignant features. Also, while benztropine is not a common therapeutic in the armamentarium for NMS care, mechanistically it functions similarly to alternative treatments like amantadine and bromocriptine. A core pathway within NMS pathophysiology is a depletion of basal ganglia dopaminergic neurotransmission secondary to neuroleptic exposure. 17 Dopaminergic drugs like amantadine and bromocriptine can be used to target this aberrant neurotransmission; however, in addition to its anticholinergic properties benztropine can also promote dopamine neurotransmission, making it a reasonable therapeutic in cases of atypical NMS. 18
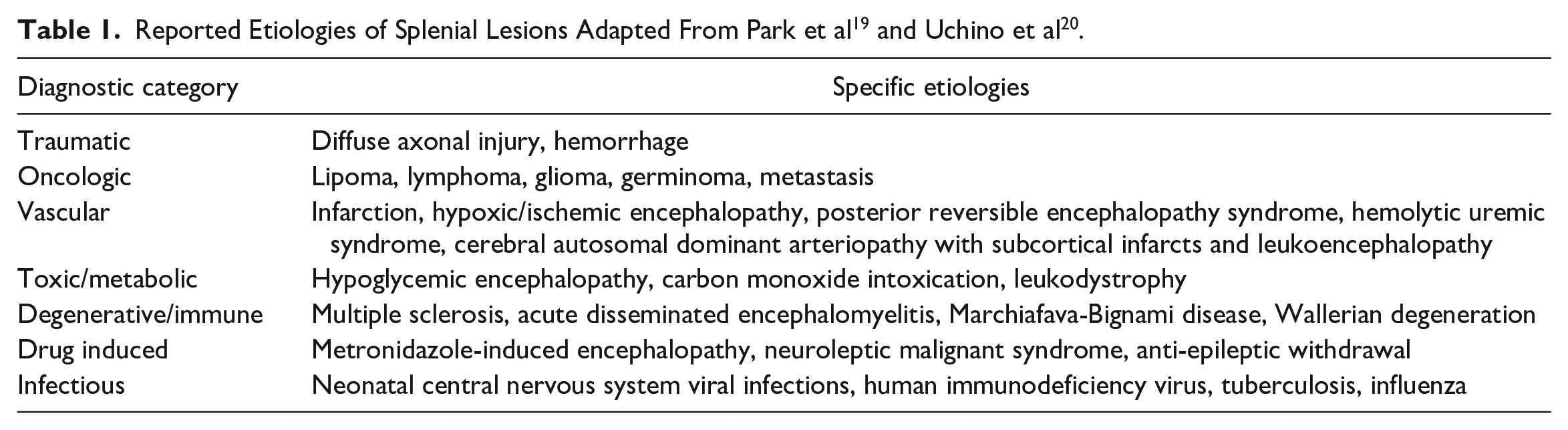
There remains some diagnostic uncertainty regarding the precise etiology of our patient’s ILSCC. A wide differential diagnosis exists for splenial lesions, which we have outlined in Table 1.19,20 For our patient, the differential included the following: ischemic lesion, oncologic lesion, traumatic lesion, transient splenial lesion secondary to NMS, and Marchiafava-Bignami disease. With regard to ischemic etiologies, callosal infarcts are rare and unlikely to be isolated, as in our patient, due to a rich vascular supply emanating from both the anterior and posterior circulations.21,22 Additionally, our patient had an unremarkable CT angiogram of the head/neck, is young, did not have a history of infarct associated drug use, and was without a previous history of atrial fibrillation or stroke, making an infarct less likely. Similarly, the possibility of an oncologic cause is unlikely given our patient did not have any systemic symptoms of cancer, did not have a family history, did not have a chronic prodrome of symptoms, and did not have imaging findings consistent with a space occupying lesion. It is feasible that our patient’s lesion was traumatic in origin considering his head injury prior to arrival and the high axonal density within the corpus callosum predisposing it to shearing forces. 19 However, axonal injury is rarely found in spatial isolation and would likely have a diffuse distribution given the severity of our patient’s injury as evident by the extent of his facial fractures. 23 The probability of Marchiafava-Bignami disease is doubtful given our patient did not have a history of alcohol abuse, had normal vitamin B12 and folate levels, had unremarkable liver function tests, and received prophylactic intravenous thiamine on admission.
Within previously published case reports documenting ILSCC in the context of NMS, the MRI lesion was characterized as midline symmetric ovoid, which matches the distinct morphology of our patient’s lesion. 19 Prior reports have shown a complete resolution of the MRI lesion within 2 to 12 weeks.7-13 In this case, imaging at 11 days showed a persistent lesion. Consequently, it remains possible that if reimaged later on, our patient’s lesion may have been found to be transient as in the previously documented cases. Therefore, the possibility of an NMS associated lesion seemed plausible given our patients unique clinical picture without other compelling etiologies. Despite being first described over a decade ago by Al-Edrus and colleagues, 8 the pathophysiology of ILSCC associated with NMS remains elusive, and none of the existing case reports postulate an explanation.7,9-13 Further exploration of the mechanistic underpinnings of ILSCC related to NMS may have utility in developing a more thorough understanding NMS pathophysiology, which might have diagnostic and treatment implications.
Despite the dearth of pathophysiologic postulates explaining the relationship between ILSCC and NMS within psychiatric publications, it is possible to synthesize a possible mechanism from existing findings within the basic science literature. Transient callosal cytotoxic edema has been extensively reviewed by Starkey and colleagues 24 and defined as a common etiology of ILSCC. They suggest a cytokine-mediated glutamate-induced N-methyl-D-aspartate receptor (NMDAR) excitotoxic process is central to the pathophysiology of cytotoxic edema within the corpus callosum. 24 With regard to NMS, Zhuravliova and colleagues 25 demonstrated that haloperidol interactions with NMDAR resulted in glutamate-independent cytochrome-C-dependent cytotoxicity. This is especially pertinent to ILSCC as there is a higher density of callosal Aquaporin-4 channels, relative to other brain regions, which are involved in cytochrome-C mediated cytotoxic pathways leading to localized edema.26,27 Additionally, PCP has been shown to cause upregulation of central NMDARs, which may have theoretically predisposed our patient to an NMS associated ILSCC. 28 This proposed mechanism may be sufficient to explain the pathophysiology of these localized lesions in the context of NMS; however, additional case reports and confirmatory research are necessary. Additionally, it is unclear if other antipsychotics mentioned in the previous case reports (risperidone, olanzapine, clozapine, and quetiapine) have similar contributions to the disease mechanism as haloperidol.
Conclusion
We have presented the first published case of an ILSCC in the context of atypical NMS, outlined the differential diagnosis for this rare finding, and postulated a neurobiological mechanism of disease. Given the widespread use of neuroleptics and availability of MRI, it is likely there are identified but unreported occurrences of these lesions. Conversely, a greater number of patients presenting with a NMS-associated ILSCC without imaging unbeknown to their clinicians is also possible. Regardless, discussions of ILSCC and NMS expand the intellectual scaffold for a richer understanding of antipsychotics, NMS, clinical neuroscience, and potentially medical decision making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because of the patient’s altered mental status. The patient’s age and other personal identifiers were anonymized for this case report.