
Abstract
Dopamine agonists are generally well tolerated and represent the first-line therapy for prolactinomas. We report a case of a 20-year-old man with a macroprolactinoma who developed recurrent priapism with cabergoline and bromocriptine. Transsphenoidal pituitary adenoma resection was done with normalization of the prolactin level. Priapism is a rare side effect of dopamine agonists that warrants discontinuation of therapy. Patients should be educated about this potential side effect at the time of prescribing the medication.
Introduction
Prolactinomas are the most frequently occurring secretory pituitary adenoma and the only one for which the first-line therapy is medical. Dopamine agonists are the first-line therapy in prolactinomas and lower the prolactin level, shrink the adenoma, and restore gonadal function. There are 3 dopamine agonists used for the treatment of prolactinoma—cabergoline, bromocriptine, and quinagolide—of which only cabergoline and bromocriptine are available in the United States. Cabergoline is the preferred agent due to a more favorable side effect profile and greater efficacy. Priapism is a rare side effect of dopamine agonists, which warrants discontinuation of therapy.
We report a patient with prolactin-secreting pituitary macroadenoma who developed priapism with both cabergoline and bromocriptine. His subsequent clinical course was complicated by the development of pituitary apoplexy requiring transsphenoidal pituitary surgery.
Case Presentation
A 20-year-old African American man was diagnosed with a macroprolactinoma after presenting to his primary care physician with complaints of worsening headaches, erectile dysfunction, gynecomastia, and nipple discharge for the past 6 months. Initial investigation revealed an elevated prolactin level of 550.8 ng/mL (reference range = 2.0-18.0). He also had hypogonadotropic hypogonadism with a low total testosterone of 26 ng/dL (250-11 000) and inappropriately normal luteininzing hormone level of 1.6 mIU/mL (1.6-9.3) and follicle-stimulating hormone level of 2.3 mIU/mL (1.6-8.0). The rest of the pituitary axis was normal (Table 1). A pituitary protocol magnetic resonance imaging study (MRI) showed a 17 mm × 12 mm pituitary gland adenoma with extension into the medial aspect of the left cavernous sinus, with rightward displacement of infundibulum (Figure 1). A visual field examination interpreted by a neuro-ophthalmologist did not reveal any deficits.
Pituitary labs at diagnosis and following apoplexy.

Denotes that a laboratory value is not available.
Magnetic resonance imaging images of the pituitary adenoma at diagnosis.
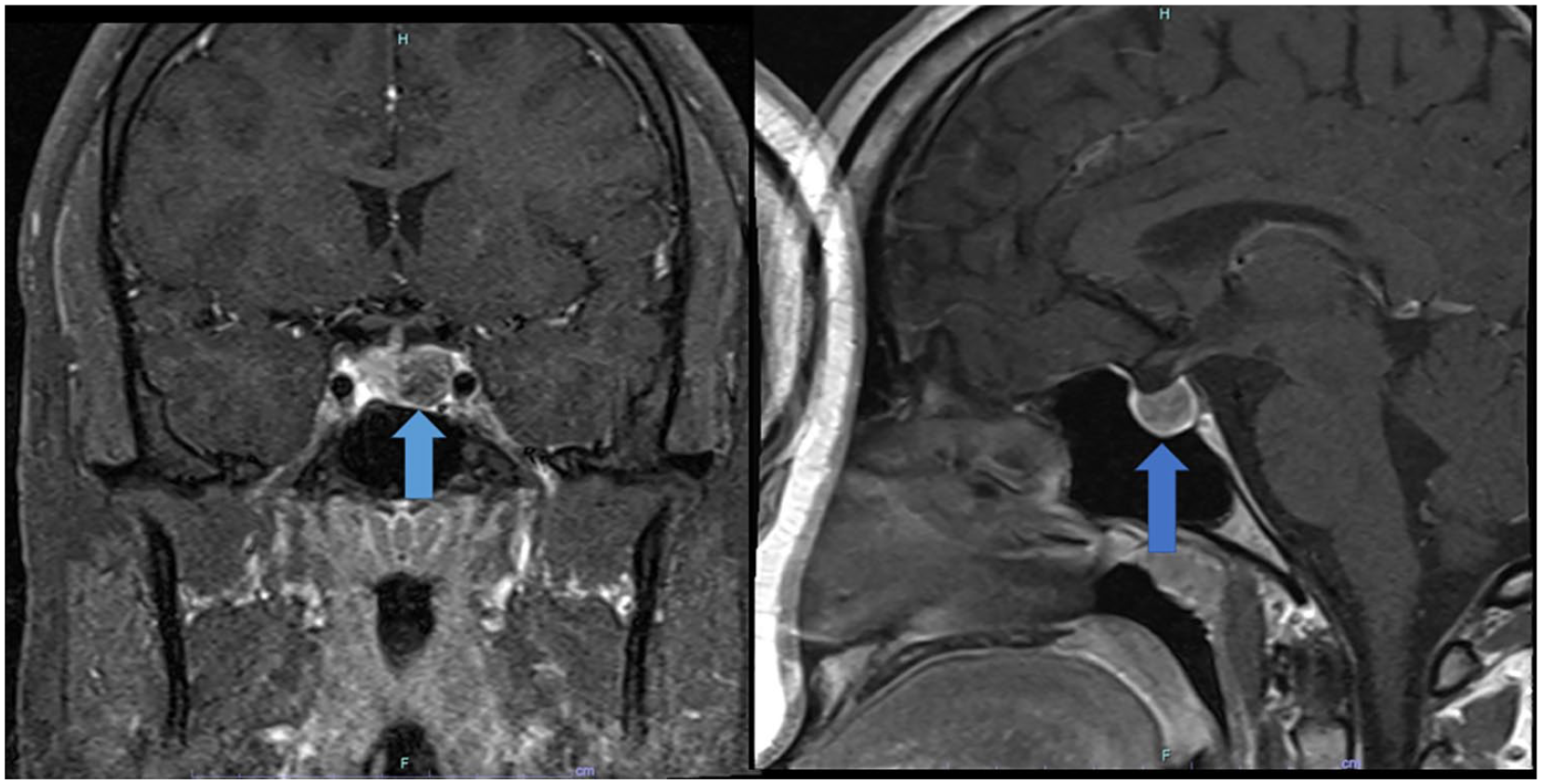
He was subsequently started on dopamine agonist therapy, cabergoline at a dose of 0.5 mg weekly. His prolactin levels responded well, decreasing to 58 ng/mL (2.0-18 ng/mL) 4 months after initiating therapy. However, around this time he experienced 2 episodes of priapism. The first episode lasted 2 hours and the second episode occurred a few days later and lasted 5 hours, prompting a visit to the local emergency department. The patient stopped taking cabergoline after learning of its association with priapism, a rare side effect. A few weeks later, he developed an episode of severe headache associated with sudden loss of vision and dizziness. Laboratory evaluation revealed elevated adrenocorticotrophic hormone level of 56 pg/mL (6-50 pg/mL) and concurrent low cortisol level of 6.3 µg/dL (6.7-22.6 µg/dL). MRI showed a new focus of T1 hyperintensity within left lateral aspect of mass, compatible with intratumoral hemorrhage, which was a new finding since the initial MRI (Figure 2). He was evaluated by a neurosurgeon at this time due to concern for apoplexy but the patient declined surgical intervention. He subsequently missed appointments with his endocrinologist for 5 months. At follow-up, his endocrinologist prescribed bromocriptine at a dose of 2.5 mg daily as his prolactin levels had risen to 195 ng/mL (2.0-18.0 ng/mL). After 2 months of taking bromocriptine, he experienced an episode of priapism lasting 2 hours. Due to intolerance of both types of dopamine agonists and persistent growth of prolactinoma, the decision was made to proceed with transsphenoidal pituitary adenoma resection 3 months later. Postoperative course was uncomplicated and final pathology confirmed prolactin producing pituitary adenoma with Ki67 proliferation index estimated at <3%.

Magnetic resonance imaging images of the pituitary following apoplexy.
Discussion
This patient did not have any risk factors for priapism such as perineal trauma, sickle cell disease, or diabetes. He was not on phosphodiesterase inhibitors or other medications associated with priapism. The episodes of priapism occurred within 2 to 4 months of starting bromocriptine or cabergoline. He did not have recurrence of priapism after withdrawal of dopamine agonist therapy. The Naranjo Adverse Drug Reaction Causality Score was 10 (definite ≥ 9), which supports a causative role for the dopamine agonists. 1
Hyperprolactinemia inhibits gonadotropin-releasing hormone secretion leading to decreased pulsatile secretion of luteininzing hormone and follicle-stimulating hormone and consequent low testosterone level. 2 Dopamine agonists are the mainstay of therapy for the treatment of prolactinomas. Prolactin secretion is regulated by the tonic inhibitory action of dopamine acting via the dopamine D2 receptors on lactotrophs. Activation of the D2 receptors by dopamine agonists lead to inhibition of prolactin secretion, late inhibition of prolactin synthesis, and eventual development of perivascular fibrosis and partial cell necrosis. 3 Cabergoline caused normalization of prolactin level in 95% of patients with microadenomas and 81% of patients with macroadenomas.4,5 It is well tolerated with the most common side effects being nausea, headache, dizziness, and drowsiness. 6 Discontinuation due to intolerance occurred in less than 3% of the patients. 6 Bromocriptine caused normalization of the prolactin level in 80% to 90% of patients with microadenomas and 70% of patients with macroadenomas. 7 It is not as well tolerated as cabergoline with the most common adverse effects being nausea, vomiting, postural hypotension, and headaches. Surgical resection of prolactinoma is warranted in case of intolerance to dopamine agonist. Testosterone level normalized in 60.9% of patients with prolactin-secreting macroadenoma following cabergoline therapy. 8 The persistence of low testosterone level following normalization of prolactin suggests damage to the gonadotrophs from mass effect, especially if associated with other pituitary hormone deficiencies.
Priapism due to cabergoline therapy for prolactinoma was first reported in 2010. 9 A subsequent report notes the occurrence of priapism 60 days after the initiation of cabergoline. 10 Priapism has also been reported with the use of transdermal rotigotine, a nonselective dopamine agonist, at a dose of 4 mg per 24 hours for the treatment of Parkinson’s disease. 11
Priapism can occur secondary to medications with the most commonly implicated medications being antidepressants, antipsychotics, and antihypertensives. The mechanism is thought to be related to the blockade of α receptors in the corpora cavernosa. 12 Bromocriptine and cabergoline display α1 and α2 adrenergic receptor antagonism in addition to their D2 receptor agonist activity. 13 Alpha-1 adrenergic blockage may be responsive for the priapism. Dopaminergic pathways in the brain and spinal cord are also involved in the control of erectile function and activation of these pathways by dopamine agonists may result in priapism. 14
Priapism has been reported in Kallman’s syndrome treated with testosterone replacement, which suggests that exposure to testosterone following a prolonged period of deprivation can be a trigger. 15 It is unclear how long our patient had been hypogonadal, but his testosterone level was markedly low at the time of his diagnosis. The episodes of priapism occurred after a sufficient interval to allow for the normalization of testosterone. Our experience with this patient suggests priapism is likely to recur even with switching to a different kind of dopamine agonist and that patients who experience this side effect are best treated with surgical resection of the adenoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for his anonymized information to be published in this article.