
Abstract
Systemic lupus erythematosus is an autoimmune disease that affects multiple organs and organ systems, subsequently requiring an elaborate regimen for management. We present the case of a 63-year-old female who developed unrelenting symptoms of drug-induced lupus, which persisted even after the offending agent was withdrawn, unmasking her underlying systemic lupus erythematosus. She continued to develop neuropsychiatric symptoms, including mania and hallucinations, which complicated the management of her disease. After exhausting the bank of anti-inflammatory and immunomodulators recommended by current guidelines, we found that a combination of rituximab infusions with thiothixene, an antipsychotic agent, significantly improved our patient’s neuropsychiatric symptoms. Further research should be conducted to determine the efficacy of rituximab in the treatment of resistant lupus cerebritis, and to validate the use of thiothixene in the management of neuropsychiatric symptoms secondary to lupus.
Keywords
Background
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that virtually affects all organs. The production of antinuclear antibodies (ANA) is a prominent feature of the disease. 1 Approximately 15 000 to 30 000 cases of drug-induced lupus (DIL) are reported every year in the United States. 2 The most common clinical features include fever, myalgias, rash, arthralgias, arthritis, and serositis.
Symptoms of DIL will often resolve on discontinuation of the drug; however, that was not the case in our patient. The ensuing neuropsychiatric symptoms that were present in our patient posed a challenge to manage. Our case highlights the importance of prompt treatment and the use of rituximab in resistant lupus cerebritis. Thiothixene was initiated for the management of neuropsychiatric symptoms in our patient, which led to significant improvement.
Case Presentation
We present the case of a 63-year-old female with past medical history of inflammatory bowel disease, DIL, and hypertension, who comes in with chief complaints of altered mental status, aphasia, and new-onset mania, including tangential speech, fleeting thoughts, and delusions.
Prior to this admission, our patient was initially treated with infliximab for inflammatory bowel disease. She soon developed inflammatory arthritis, serositis, and mucosal ulcers with a positive speckled pattern ANA on staining. She was thought to have DIL secondary to infliximab treatment. Inflammatory symptoms persisted despite withdrawal of infliximab. She was tried on hydroxychloroquine, transitioned to mycophenolate mofetil, and eventually was placed on cyclosporine, with minimal symptomatic relief.
During this admission, laboratory tests were significant for a lactic acid dehydrogenase of 334 U/L, C3 of 49 mg/dL, and C4 of 10 mg/dL. Immunology workup is shown below (Table 1).
List of Antibody Titers.

Abbreviations: dil, dilution; ANA, antinuclear antibody; SSA, anti–Sjögren’s-syndrome type A; SSB, anti–Sjögren’s syndrome type B; RNP, ribonucleoprotein; SCL, scleroderma; Ig, immunoglobulin; Ab, antibody.
Findings on magnetic resonance imaging (Figure 1) showed mild multifocal white matter hyperintensities unchanged from previous studies. Lumbar puncture did not yield significant results. Ammonia level was within normal limits.
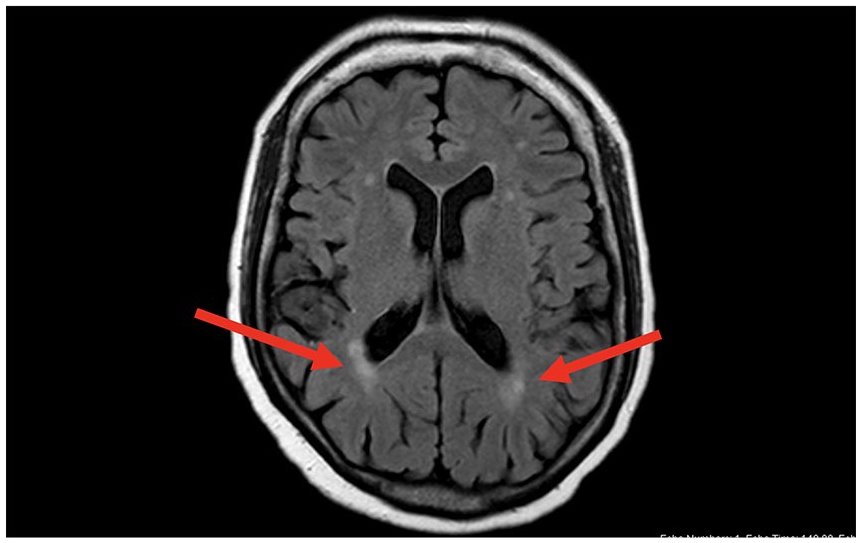
Magnetic resonance imaging showing mild multifocal white matter hyperintensities (arrows) unchanged from previous studies.
In light of decreased C3 and C4, rheumatology recommended pulse dose methylprednisolone, plasmapheresis, and mycophenolate mofetil 1 g twice daily. For her manic symptoms, psychiatry initially recommended steroid therapy and close monitoring.
Due to the persistence of pressured speech and new onset of visual hallucinations, olanzapine 10 mg twice daily was added to the regimen.
After the first week of treatment, plasmapheresis was discontinued, due to minimal improvement. We started the patient on rituximab infusions weekly and noticed improvement in her inflammatory symptoms including serositis, mucosal ulcers, and polyarthritis. Laboratory test values were repeated at this time, which showed a C3 of 133 mg/dL and a C4 of 27 mg/dL.
During this time, our patient continued to have waxing and waning episodes of mania. Olanzapine was titrated up to a dose of 30 mg daily, and was then cross tapered with risperidone 2 mg daily. However, her psychiatric symptoms persisted.
Thiothixene was then initiated, which helped improve her symptoms. After 1 week of thiothixene 2 mg nightly, we noticed resolution of visual hallucinations, delusions, and pressured speech. She was then discharged to a rehabilitation center on prednisone 20 mg daily, mycophenolate mofetil 1 g twice daily, and thiothixene 2 mg twice daily.
Discussion
Drug-induced lupus is a rare manifestation of lupus-like symptoms associated with a variety of drugs. It is insidious in onset, usually after months of using the offending agent, and symptoms regress n removal. 2 Anti–tumor necrosis factor drugs, chemotherapeutic agents, along with procainamide, isoniazid, and hydralazine are responsible for triggering an inappropriate autoimmune response. 1 Common clinical features include fever, myalgias, rash, arthralgias, arthritis, and serositis. 2
According to literature, there is no universally accepted diagnostic criteria for DIL; however, at least one symptom that overlaps with idiopathic SLE, no prior history of idiopathic SLE, and resolution of symptoms on removal of offending agent point toward the diagnosis of DIL. Positive ANA, and perinuclear ANCA (P-ANCA) tests are found in 92% and 83% of patients, respectively. 3 Anti-histone antibodies are seen in more than 95% of DIL. 4 Medications such as hydroxychloroquine, which are effective in idiopathic SLE, are also effective in patients with resistant DIL. It is used temporarily for constitutional, cutaneous, and musculoskeletal symptoms. 5
In our patient, infliximab was thought to be the agent responsible for the development of DIL. However, prompt discontinuation of infliximab did not alleviate our patient’s inflammatory symptoms. She was tried on multiple immunomodulators, without significant success. On review of the immunology results, our patient had a positive ANA titer, as well as a positive speckled pattern. Anti–double stranded DNA antibodies and anti-histone antibodies were negative on admission. We propose that our patient’s presenting lupus-like symptoms were a manifestation of her underlying SLE, which was exacerbated by her DIL. Unfortunately, once her SLE was activated, this led to the subsequent complications of lupus cerebritis and neuropsychiatric symptoms.
Central nervous system involvement is seen in idiopathic SLE producing a wide range of symptoms including encephalopathy, coma, depression, psychosis including bipolar disorder, stroke, and seizures. 6 Diagnosing lupus cerebritis can be challenging, since it is difficult to differentiate it from other complications that arise from metabolic disorders, infections, and hypertension. 7 Lupus cerebritis is treated empirically with anti-inflammatory agents and immunosuppressive therapy.
Rituximab is a monoclonal antibody that targets CD20 antigen and is a biologic disease-modifying antirheumatic drug frequently used in rheumatoid arthritis. 8 According to literature, minimal research has been done in the use of rituximab in SLE. The EXPLORER trial was a randomized, double-blinded study that tested the efficacy and safety of rituximab in patients with extrarenal SLE.
Our patient primarily presented with symptoms of psychosis, which occurs in approximately 5% of patients with idiopathic SLE. 7 The nonspecific findings on brain magnetic resonance imaging and insignificant result on lumbar puncture led us to the diagnosis of lupus cerebritis. Trials of prednisone, hydroxychloroquine, cyclosporine, and mycophenolate mofetil were used with minimal response. Our patient was started on rituximab infusions, which greatly improved the clinical outcome. We propose that the use of rituximab should be explored for patients with severe, extensive lupus cerebritis refractory to guideline-directed therapy.
Our patient required the initiation of an antipsychotic regimen, in addition to an anti-inflammatory regimen, to control her manic symptoms. Thiothixene is a first-generation typical antipsychotic medication that has been used since the 1950s to treat psychosis. According to a case series, thiothixene was used in the management of patients with delirium with favorable results. Very few clinical trials have been done with thiothixene in the management of psychosis due to delirium, let alone thiothixene in lupus cerebritis. 9
The synergistic effect of rituximab infusion along with thiothixene led to significant improvement in our patient’s neuropsychiatric symptoms secondary to SLE.
Conclusion
We report a rare case of treatment-resistant lupus cerebritis. This case details an innovative approach to manage lupus cerebritis with the combination of immunomodulators and antipsychotic drugs. It is imperative that further research and multicenter clinical trials are conducted to establish the efficacy of rituximab in the treatment of resistant SLE, and to explore the use of thiothixene in the management of consequent neuropsychiatric symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.