
Abstract
Inflammatory pseudotumor (IPT) of the kidney is a rare benign disorder with unknown etiology. In IPT patients, some nonspecific symptoms might present, such as fever, hematuria, and back pain. As it can appear on computed tomography and magnetic resonance imaging as a hypovascular mass with surrounding fat stranding, IPT can be misdiagnosed as a primary tumor. Since the clinical symptoms, radiographic features, and preoperative findings can be inconsistent, it is imperative to confirm IPT based on histopathological assessment. In the present study, we describe a case of renal IPT in a 13-year-old girl. The patient was treated with nephrectomy of the right kidney since the preoperative diagnosis was renal carcinoma. Pathological examination revealed an IPT. This article emphasizes the importance of preoperative definitive diagnosis in avoiding unnecessary nephrectomy.
Introduction
Inflammatory pseudotumor (IPT), a benign condition with unknown etiology, affects multiple organs such as the lung, mediastinum, liver, and skin. Renal IPT is quite rare.1-3 Other names for IPT include inflammatory myofibroblastic tumor, xanthomatous pseudotumor, plasma cell granuloma, inflammatory myofibroblastic proliferation, and myofibroblastoma. 4 Most patients with IPT have nonspecific symptoms, such as flank pain, hematuria, and fever. 5 Imaging characteristics may also be atypical, making IPT difficult to distinguish from a malignant lesion. 1 In this case, histopathological examination of the lesion revealed spindle-shaped cells, myofibroblasts, and mixed inflammatory cells such as plasma cells, lymphocytes, and histiocytes.1,5 Understanding the symptomatic, radiological, and pathophysiologic features of IPT is essential to prevent unnecessary surgery. In this article, we present a case of renal IPT that resulted in an unnecessary nephrectomy.
Case Description
A 13-year-old girl was sent to the hospital due to right flank pain lasting 2 months. On admission, her body temperature was normal (37 °C). Laboratory studies showed a normal white blood cell count and neutrophils and normal creatinine serum level (0.6 mg/dL). The urine was yellow. Urinalysis showed no red blood cells and 2 to 4 white blood cells per high-power field (HPF); the normal range of white blood cells is <5 cells per HPF. 6 An abdominal computed tomography (CT) scan was performed. Pre-contrast images showed right renal enlargement with homogenous renal parenchyma (Figure 1). The arterial phase of the abdominal CT images revealed a heterogeneously low-enhancing mass with ill-defined borders situated in the right kidney (Figure 2A). There were some intratumoral hypodense areas, and the lesion extended beyond the renal capsule into the perirenal space (Figure 2B). The mass showed a slightly elevated level of enhancement in the venous phase (Figure 3). The mass measured 43 × 45 × 52 mm. The average density of the mass was 35 Hounsfield (HU) in the pre-contrast phase, 72 HU in the arterial phase, and 85 HU in the venous phase. The mass extended into the perirenal fat space and stranding of the surrounding fat extended into the perirenal fat space was noted (Figure 3). None of the other abdominal mass presented. CT scanner images suggested a renal carcinoma that extended into the perirenal fat. A nephrectomy was performed after the initial diagnosis. Macroscopically, gross examination revealed a well-circumscribed mass measuring 4 cm. The cut surface was yellow and homogeneous without hemorrhage. The lesion extended into the perirenal fat tissue (Figure 4). Microscopically, there was an absence of renal structure (Figure 5A) with inflammatory infiltration into the perirenal fat tissue (Figure 5B). The renal tubules were destroyed (Figure 5C), and there was infiltration of lymphocytes and plasma cells (Figure 5D). Some necrotic areas with neutrophils infiltration were also detected. The patient received no further treatment and was discharged from the hospital 2 weeks after surgery.

Axial precontrast abdominal computed tomography image revealed that the right kidney was enlarged, homogenous, and slightly low density when compared with the left kidney.
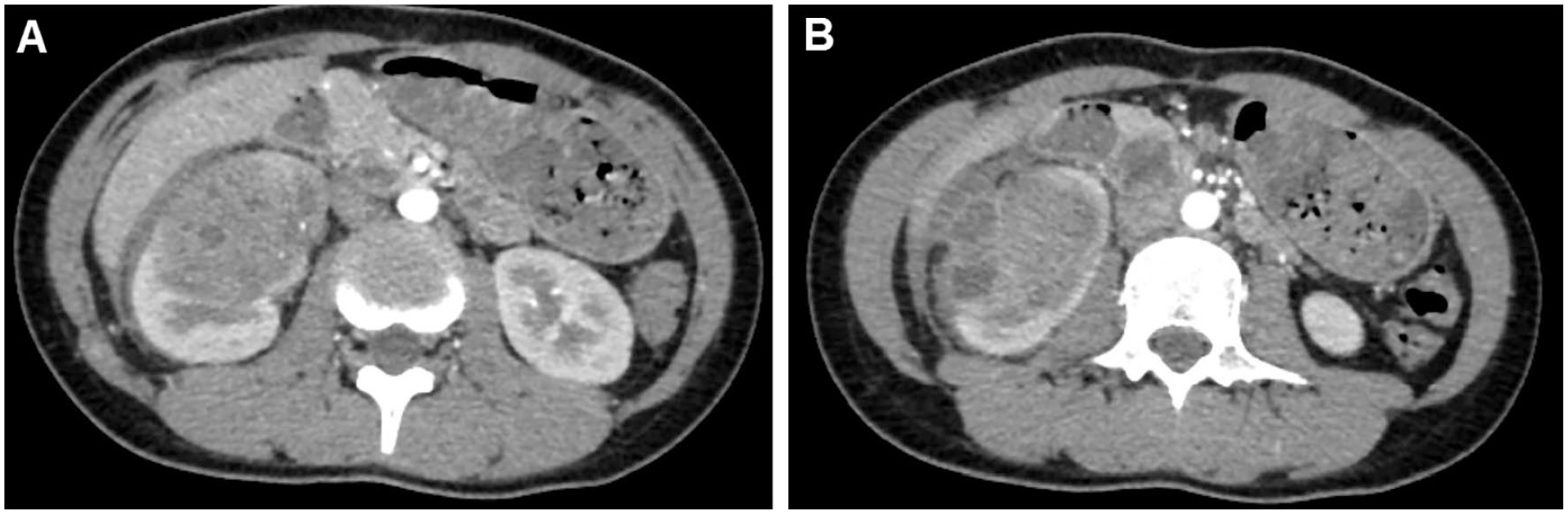
The mass in the right kidney was heterogeneously low-enhancing with ill-defined margins (A). Some hypodense portions of the mass extended beyond the renal capsule into the perirenal space (B).

The lesion showed an elevated level of enhancement in the venous phase (A and B). The lesion was in the lower renal pole and extended into the perirenal fat space (C).

Gross examination revealed a wedge-shaped, well-circumscribed mass with a pale-yellow cut surface occupying most of the lower renal pole and extending into perirenal fat tissue.

(A) The lesion area showed a loss of renal structure (right) compared with the normal parenchyma (left; hematoxylin-eosin [HE] ×40). (B) Inflammatory infiltration into perirenal fat tissue (HE ×40). (C) Renal tubules were destroyed or filled with cell debris, and several intact glomeruli were observed (HE ×100). (D) Renal parenchyma was replaced by mixed inflammatory infiltration (HE ×400).
Discussion
Renal IPT, a rare kidney disorder with no sex predilection, affects a wide range of ages. 4 Currently, the etiology of IPT is uncertain; possibilities include trauma, surgery, calculous pyelonephritis, and autoimmune disease.5,7 Patients with renal IPT usually complain of abdominal pain, hematuria, fever, and urinary tract infections. 8 A diagnosis based solely on imaging characteristics might overlook IPT. The borders of a lesion can be well-circumscribed or ill-defined. 9 On CT images, lesions may have low, homogeneous, or heterogeneous density. Intratumoral vascularity could be present.
In the current case, the mass demonstrated variable contrast enhancement.10,11 On magnetic resonance imaging, the lesion had low signal intensity on T1-weighted images but was hyperintense on T2-weighted images. The enhancement of the lesion could have been delayed due to fibrosis within the mass. 11 The distinctions between clinical and radiological characteristics of renal IPT and renal carcinoma are not effectively definite. Macroscopic samples manifested a well-circumscribed, nonencapsulated, homogenous mass with yellow cut surfaces.3,12 Histological evaluation found both acute and chronic inflammation cells in the IPT lesion, including lymphocytes, plasma cells, myofibroblastic spindle cells, and variable amounts of fibrosis.1,7
Some IPTs are associated with immunoglobulin (Ig) G4-related disease. 13 This is a systemic disease with extensive IgG4-positive plasma cell and T-cell infiltration of affected organs. As clinical symptoms and imaging findings are not specific, settling on a precise preoperative diagnosis is complicated. In addition, IPT often mimics a malignant tumor; therefore, carrying out a histological examination to establish the diagnosis is mandatory. Beside preoperative biopsy, elevated serum IgG4 is also helpful for the diagnosis of IgG4-related IPT of the kidney.13,14 Renal IPT is a benign disease caused by an inflammatory reaction, so treatment with antibiotics rather than nephrectomy is required. 14 For those cases of IgG4-related IPT of the kidney, glucocorticoid treatment is rather effective. 15
In our case, symptoms did not indicate inflammation; furthermore, CT findings revealed a mass in the right kidney. An exact preoperative diagnosis was not established, and the patient underwent a nonessential nephrectomy. A histopathological report confirmed IPT of the kidney. Further questioning revealed that the patient had experienced slight fever (38 °C) within the previous 2 months. On reevaluating the CT scanner images and associated with the histopathology results, we determined that this lesion was a ruptured abscess into the perirenal space associated with earlier chronic inflammation.
Conclusion
We reported an IPT of the kidney masquerading as a renal carcinoma. The clinical symptoms and imaging findings were nonspecific and led to an unnecessary nephrectomy. We recommend that clinicians consider IPT as the differential diagnosis of a primary renal mass. Preoperative renal biopsy is crucial to avoid overtreatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was obtained.