
Abstract
A 65-year-old African American man initially presented to the emergency department complaining of headaches, retro-orbital pressure, decreased vision, white flashes and floaters, and palinopsia of both eyes. After complete evaluation, he was diagnosed with migraine with aura and discharged to home with an ophthalmology follow-up. Upon follow-up with the ophthalmology team, he had developed severe periorbital inflammation, proptosis, chemosis, and vision loss that was greatest on the left side. The patient was immediately hospitalized for further evaluation and steroid treatment. His vision, ocular symptoms, and physical findings dramatically and rapidly improved with a 3-day course of high-dose intravenous steroids. Existing literature is sparse on rapid loss and recovery of vision following steroid treatment for orbital myositis. The exact mechanism of vision loss in orbital myositis is not understood and merits further investigation. Orbital myositis is a subset of nonspecific orbital inflammatory syndrome. It remains a poorly understood condition that mimics other, more common conditions such as thyroid eye disease and orbital cellulitis. If left untreated, orbital myositis could progress to the point of continued inflammation, enlargement of ocular tissues, ocular ischemia, and optic neuritis. To reverse these symptoms and prevent further progression, a quick diagnosis followed by steroid treatment is imperative.
Keywords
Background
Orbital myositis is a relatively common condition that accounts for about 5% to 10% of orbital disorders, yet the etiology and pathophysiology remain largely unknown. 1 This condition is thought to be a benign, noninfectious, inflammatory process of orbital tissues without an obvious local or systemic cause. Orbital myositis often presents with nonspecific symptoms that are frequently confused for migraine with aura, orbital cellulitis, giant cell arteritis, demyelinating disease, or thyroid eye disease. The disease itself is characterized by painful diplopia and proptosis; however, in most cases, vision loss does not occur. 2 To reverse these symptoms and prevent further progression, a quick and accurate diagnosis followed by steroid treatment is imperative. This case report describes the development of vision loss and subsequent vision recovery in orbital myositis. It illustrates an atypical disease course and demonstrates a rapid and excellent patient outcome following high-dose intravascular steroid.
Case Presentation
A 65-year-old African American man with a past medical history significant for hypertension, chronic obstructive pulmonary disease, mitral valve prolapse, chronic kidney disease, osteoarthritis, posttraumatic stress disorder, 2 cerebral vascular accidents (2005 and 2015), nephrolithiasis, and chronic low-back pain presented to the emergency department complaining of headaches, retro-orbital pressure sensation, decreased vision in the left eye, white flashes and floaters, and palinopsia of both eyes. These symptoms developed and worsened over the course of 24 hours prior to presentation in the emergency room. On initial workup in the emergency room, he lacked fever, leukocytosis, or other signs of infectious etiology. Ophthalmology was then consulted for further evaluation. His best-corrected visual acuity (BCVA) was 20/40 right eye (OD) and 20/60 left eye (OS) with full extraocular movements and high/normal intraocular pressures of 20 mm Hg OD and 21 mm Hg OS. There was a 1+ relative afferent pupillary defect OS. Computerized tomography (CT) scan of the head was unremarkable. Slit lamp examination and dilated fundus examination were unremarkable except for 2+ nuclear sclerotic cataract of both eyes. The initial diagnosis was migraine with aura, and he was subsequently discharged to home with a follow-up ophthalmology appointment.
Ten days later, the patient presented to the ophthalmology clinic with worsening vision loss bilaterally, worsening headaches and retro-orbital pressure sensation, and periorbital swelling (Figure 1). His BCVA was 20/150 OD and counting fingers at 1 meter OS. His intraocular pressure (IOP) was elevated at 26 mm Hg OD and 27 mm Hg OS. His extraocular movements were reduced in all directions of gaze. His Hertel’s exophthalmometer reading was 22 mm OD and 26 mm OS with a base of 118 mm.

Anterior and lateral views of left eye chemosis, proptosis, and erythema before steroid therapy at initial presentation at the ophthalmology clinic.
He was admitted that same day to the hospital for further evaluation. Magnetic resonance imaging (MRI) (Figure 2) of the orbits showed significant proptosis with straightening of the optic nerves and enlargement of all extraocular muscles to include the tendon sheath. Immunoglobulin (IgG), angiotensin-converting enzyme (ACE), thyroid stimulating immunoglobulin (TSI), thyroid stimulating hormone (TSH), and thyroxine (T4) levels were all within normal limits.
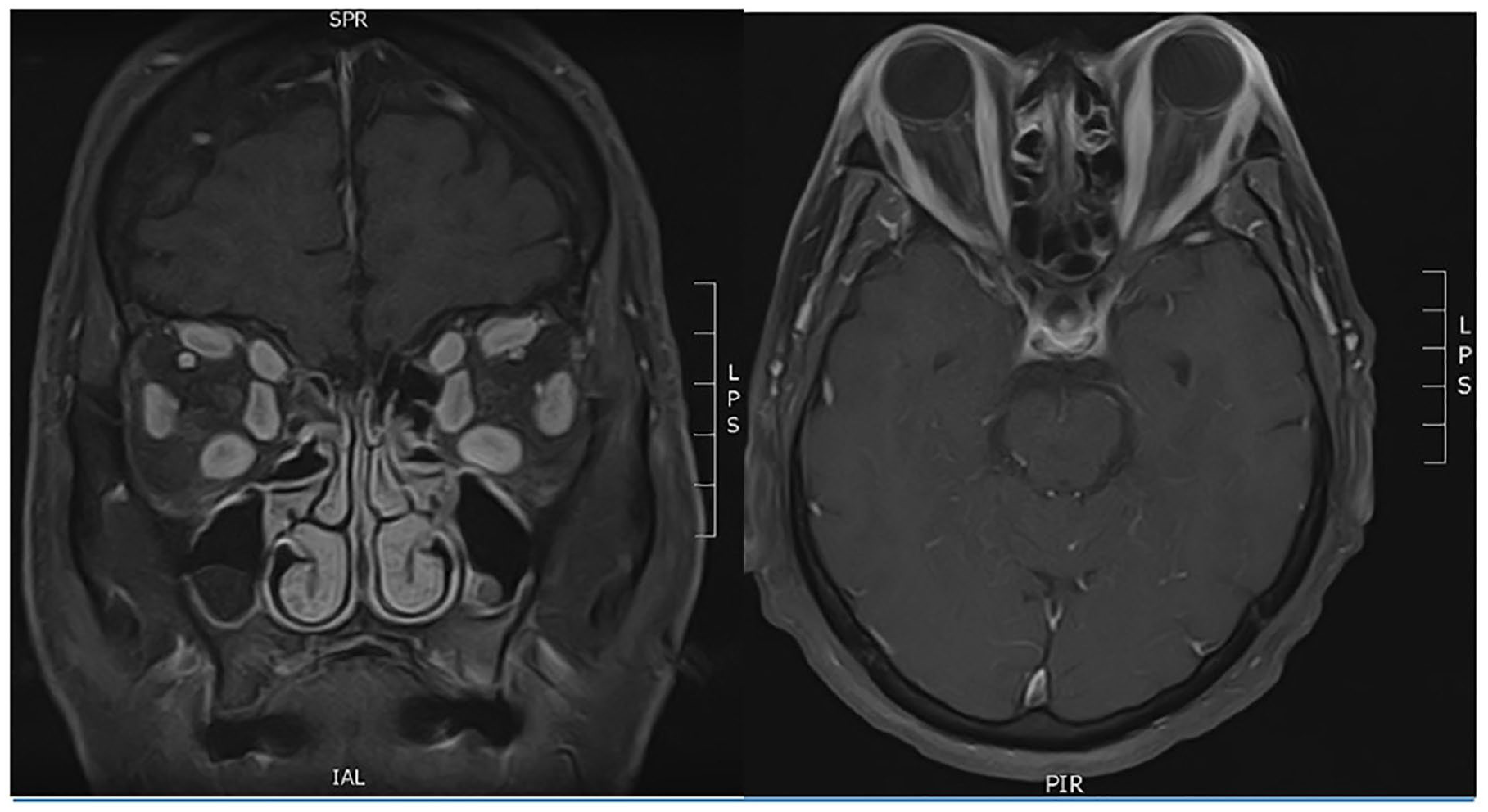
Magnetic resonance imaging head, coronal, and axial views. Enlargement of all extraocular muscles bilaterally. Scattered fluid-attenuated inversion recovery (FLAIR) hyperintensities were also noted within the white matter.
On hospital day 2, the patient began a 3-day course of 1000 mg of intravenous (IV) prednisone. The following day, BCVA improved to 20/40 OD and 20/50+ OS, with an IOP of 21 mm Hg in each eye. His extraocular movement was full, and orbital swelling greatly decreased (Figure 3). He was held at the hospital for 2 more days on 1000 mg of IV prednisone and finally discharged on 100 mg per os (PO) of prednisone with a weekly taper. A month after discharge, his BCVA improved to 20/25 OD and 20/20 OS with an Hertel’s exophthalmometer reading of 17 mm OD and 17 mm OS on 40 mg PO of prednisone every day.

Anterior view of dramatic improvement of proptosis, chemosis, and conjunctival injection after only 24 hours of intravenous corticosteroid.
Investigations
In the emergency department at the time of presentation, a CT scan of the patient’s head was ordered (Figure 4). The rational for this imaging was headache with decreased sensation on the left side of face. The radiologist report stated no evidence of acute hemorrhage, edema, or mass effect.

Computed tomography head, coronal, and axial views. Taken in the emergency room at the time of initial presentation. The radiologist report stated no evidence of acute hemorrhage, edema, or mass effect.
On follow-up, the patient was admitted to the hospital, and CT angiogram and MRI head scans were performed. The CT angiogram did not show abnormalities besides some calcification of bilateral carotid bulbs and R > L stenosis of the carotid arteries. No dissection or aneurysm was noted. On MRI (Figure 2), the radiologist noted enlargement of all extraocular muscles bilaterally. Scattered FLAIR hyperintensities were also noted within the white matter, likely reflecting sequelae of microvessel angiopathy, vasculitis, demyelinating process, migraine/headaches, posttraumatic residue, postinfection gliosis, and/or postinflammatory gliosis. Conjunctival biopsy (Figure 5) was normal and showed no sign of lymphoproliferative disease.

Conjunctival biopsy taken was normal and showed no sign of lymphoproliferative disease.
Differential Diagnosis
Many disease processes can mimic orbital myositis, and thus, a broad differential diagnosis should be considered to ensure other serious conditions are not overlooked. As one of the most common orbital diseases causing proptosis, thyroid eye disease must always be included in the differential. However, the normal thyroid function tests and thyroid antibodies made this diagnosis less likely. Orbital cellulitis, another common and serious cause of orbital swelling, was considered due to pain, proptosis, and reduced extraocular movement. However, this too was ruled out due to lack of fever, leukocytosis, or other signs of infectious etiology. Giant cell arteritis was considered because of unilateral eye pain associated with vision changes but ultimately ruled out due to a lack of jaw claudication and normal C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) laboratory test results and normal optic nerve appearance. Lymphoproliferative disease was considered as it is a common source of unilateral eye swelling, but negative conjunctival biopsy made this diagnosis less likely. Peculiar presentation of infectious etiologies such as tuberculosis, syphilis, Lyme disease, and acquired immunodeficiency syndrome was also ruled out given negative laboratory markers for these diseases. Finally, many rheumatologic conditions, such as lupus, dermatomyositis, sarcoidosis, rheumatoid arthritis, and Wegener’s granulomatosis, have been known to cause orbital swelling, but an unremarkable autoimmune panel (Antinuclear antibodies (ANA), Rheumatoid factor (RF), Cytoplasmic antineutrophil cytoplasmic antibody (c-ANCA)), made these diagnoses less likely.
Orbital myositis is largely a diagnosis of exclusion as there are no positive diagnostic criteria. Once thyroid eye disease, orbital cellulitis, and a lymphoproliferative etiology were ruled out, the next step in management was to proceed with steroid therapy. The rapid and dramatic response to this therapy ultimately made orbital myositis the most likely diagnosis in this patient.
Treatment
The patient was admitted to the hospital to receive 1000 mg of IV prednisone. After 3 days of 1000 mg of IV prednisone, the patient was discharged to begin a 9-week steroid taper from 100 mg PO daily prednisone for 1 week down to 2.5 mg PO daily prednisone for 1 week. After discharge from the hospital and finishing his 9-week steroid taper, the patient’s BCVA improved to 20/25 OD and 20/20 OS with normalization of the Hertel’s exophthalmometer reading. No harmful side effects from steroid therapy were observed or reported.
Discussion
Clinical guidelines surrounding orbital myositis depend on the severity of presentation according to a treatment algorithm by Iowa University. 3 Per this algorithm, for mild disease (ie, mild/moderate pain and diplopia, but no examination findings to suggest proptosis), guidelines suggest deferring laboratory testing and trialing nonsteroidal anti-inflammatory drug treatment. For a classic disease (ie, mild/sever pain, diplopia, and obvious proptosis/inflammation), basic laboratory testing is indicated to rule out infection or thyroid eye disease. Also, CT or MRI remains the imaging modality of choice, and oral corticosteroids are the recommended treatment. For an atypical disease (ie, severe/debilitating disease and diplopia with or without evidence of orbital inflammation), basic laboratory testing should be pursued to rule out infective/thyroid etiology, then orbital MRI/CT scan and orbital biopsy should be considered as well as hospitalization for pain management and IV steroid treatment. Radiation therapy may be used in extreme scenarios. 4
Because this patient had acute vision changes and lacked diplopia, he did not fit perfectly into this classification system. However, given the severity of his proptosis, evidence of active orbital inflammation, and severe pain, he was characterized as having the “classic disease.” Based on his symptoms and this classification, a trial of steroid treatment was warranted. Because of the severity of his symptoms and his inability to consistently take oral medications, he was admitted to the hospital for IV steroid treatment.
Existing literature shows that patients with orbital myositis generally respond well to steroid treatment. Steroid treatment dramatically reduces proptosis and inflammation in these patients and consequently reduces diplopia. Despite this patient’s vision loss and lack of diplopia, he still responded quickly and completely to steroid treatment. To the best of our knowledge, this case report describes for the first time the development of vision loss secondary to orbital myositis, followed by subsequent recovery. We illustrate such a disease course and demonstrate an excellent patient outcome when treated with high-dose steroid taper.
The exact mechanism of vision loss in orbital myositis is not understood. Some possible hypotheses that merit further investigation may include optic nerve compression, swelling-induced ischemia, or generalized neuronal or brain injury secondary to inflammation. Further investigation may elucidate the pathophysiology of this disease and provide a framework for improved classification and management of this condition in the future.
Learning Points
Orbital myositis is a common condition that accounts for about 5% to 10% of orbital disorders.
Orbital myositis mimics other conditions such as thyroid eye disease and orbital cellulitis.
Orbital myositis may be associated with vision loss.
A quick and accurate diagnosis followed by treatment with steroid is imperative to prevent progression and is associated with a rapid resolution.
Footnotes
Authors’ Note
The currently submitted work represents original research that has not been previously submitted and is not under consideration for publication elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient was lost to follow-up and unable to be contacted. All personal identifiers have been removed and information has been anonymized for patient protection.