
Abstract
This study reported 2 new patients and 16 historical cases with pathologically proven intraocular infiltration with adult T-cell leukemia and lymphoma (ATLL) to know the timing of intraocular infiltration in the disease course. The first case was a 67-year-old woman who developed bilateral vitreous opacity about half a year after the onset of acute type of ATLL that had been unresponsive to chemotherapy. She underwent vitrectomy combined with cataract surgery in both eyes. She had bilateral optic disc atrophy and localized retinal white infiltrates in both eyes. Cytological examination of vitreous aspirates demonstrated medium-sized cells with aberrant flower-like convoluted nuclei, positive for CD3, and thus indicative of T-cells. The second case was a 38-year-old man who was diagnosed acute type of ATLL at the presentation of acute kidney injury. About half a year after initial chemotherapy and allogeneic hematopoietic stem cell transplantation, he developed aqueous hypopyon in the right eye, concurrent with cutaneous and central nervous system relapse. Aqueous tap disclosed class V abnormal cells. The aqueous “pseudohypopyon” resolved in response to another round of chemotherapy with mogamulizumab. In review of 18 patients, intraocular infiltration with ATLL was diagnosed by vitrectomy in 9, aqueous tap in 3, chorioretinal biopsy in 3, and autopsy in 3. The intraocular infiltration developed concurrently with systemic diagnosis of ATLL in 5 patients, but developed later after chemotherapy in 13. In conclusion, intraocular infiltration with ATLL appears rare, and pathological diagnosis by vitrectomy and aqueous tap would help determine therapeutic plan in relapse after chemotherapy.
Keywords
Background
Adult T-cell leukemia and lymphoma (ATLL) is a consequence of infection of T lymphocytes with human T-lymphotropic virus type 1 (HTLV-1). HTLV-1 infection or carrier state is endemic in specific areas in the world such as southwest Japan, Caribbean Islands, Central Africa, and South America. 1 In addition to ATLL, HTLV-1–associated uveitis and myelopathy are known as clinical entities of HTLV-1 infection.2,3 Intraocular infiltration with ATLL cells manifests as retinal vasculitis with sheathing, retinal white lesions, and vitreous opacity.1,4 ATLL may also present a space-occupying lesion in the conjunctiva 5 and orbit. 6
In this study, we present 2 patients with pathologically proven intraocular infiltration with ATLL: one patient with vitreous opacity in both eyes and the other patient with aqueous hypopyon (pseudohypopyon) in the right eye. In addition, we reviewed 16 patients of pathologically proven intraocular infiltration with ATLL in the literature7-22 to answer a clinical question when would be the timing of intraocular infiltration in the course of the disease.
Report of Cases
Case 1
A 67-year-old woman developed acute type of adult T-cell leukemia in the 20-year follow-up of diabetes mellitus that had been well controlled with insulin. She was born in Kochi Prefecture where HTLV-1 infection is endemic, and was known to have a positive serum titer to HTLV-1. She underwent CHOP-V-MMV (cyclophosphamide, doxorubicin, vincristine, prednisolone, VP-16, ranimustine, mitoxantrone, vindesine) as standard chemotherapy in the year 2003 for 5 months but without marked effect. She had received partial retinal laser photocoagulation for diabetic retinopathy only in the left eye. She noticed blurred vision in both eyes and was referred from a local hospital to Okayama University Hospital. The best-corrected visual acuity was 0.06 in the right eye and light perception in the left eye. She showed 2+ fine keratic precipitates, aqueous 1+ cells, and 1+ flare, and total posterior iris synechiae in both eyes. Vitreous opacity in both eyes prevented detailed fundus visualization, but the optic discs in both eyes appeared atrophic (Figure 1B). The intraocular pressure was 15 mm Hg in both eyes. Systemically, white blood cell count was 24 300/µL and red blood cell count 2.52 × 106/µL.
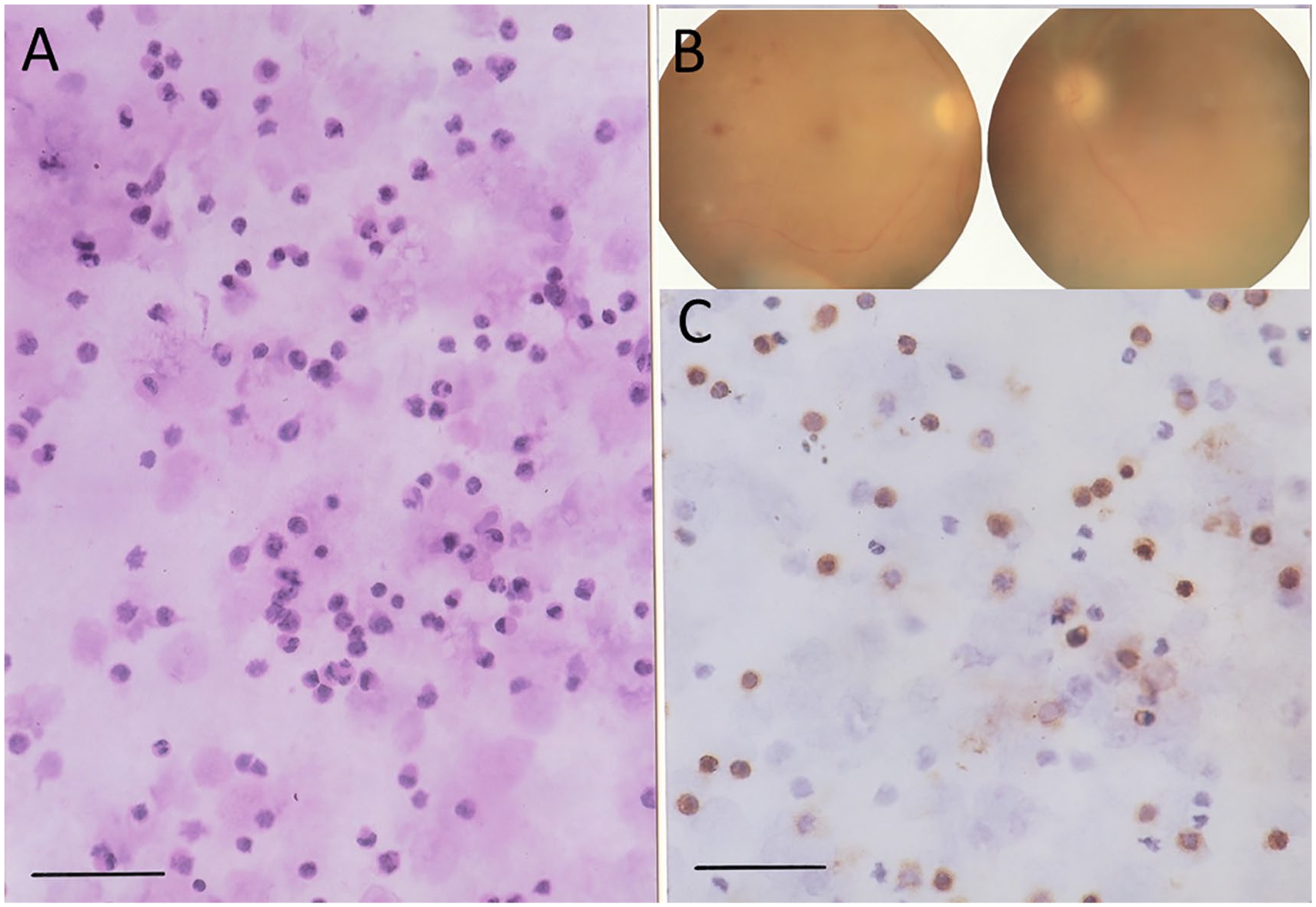
Case 1. A 67-year-old woman with vitreous opacity and atrophic optic disc in the right eye (B, left panel) and the left eye (B, right panel). Vitreous cytology of vitrectomy fluid in both eyes demonstrates medium-sized cells with aberrant nuclei in hematoxylin-eosin stain (A), which is positive for CD3 (C), indicative of T-cells. Bar = 50 µm.
She underwent vitrectomy combined with cataract surgery at first in the right eye and later in the left eye. On cytological examinations, the vitreous aspirates contained medium-sized cells with aberrant nuclei (Figure 1A). Immunostaining revealed that these cells were positive for CD3, indicative of T-cells (Figure 1C). During the surgery, white localized retinal infiltrates were observed in the superior fundus of the right eye and inferotemporal fundus of the left eye. The visual acuity after the vitrectomy was 0.2 in the right eye and hand movement in the left eye. Blot retinal hemorrhages were present in both eyes, and photocoagulation scars were noted in the left eye. She was referred back to the local hospital and lost to follow-up.
Case 2
A 38-year-old man developed abdominal fullness, headache, vomiting, and lower limb tremor, and was transferred in emergency to Okayama University Hospital as acute kidney injury. On the blood test, white blood cell count was 10 720/µL, calcium 17.1 mg/dL, and creatinine 6.65 mg/dL. He underwent emergency hemodialysis. He showed a positive serum titer to HTLV-1 and had abnormal cells with flower-like convoluted nuclei in the peripheral blood. Flow cytometry of the peripheral blood as well as the bone marrow tap showed a dominant population of CD4-positive, CD25-positive, CCR4-positive, and CD7-negative cells. He was diagnosed as acute/lymphoma type of adult T-cell leukemia/lymphoma with central nervous system involvement. He underwent one course of mLSG15 chemotherapy, 23 namely, standard combination of VCAP (vincristine, cyclophosphamide, doxorubicin, prednisolone), AMP (doxorubicin, ranimustine, prednisolone), and VECP (vindesine, etoposide, carboplatin, prednisolone), followed by 2 courses of CHOP. He was in complete remission. In the myeloablative preconditioning with cytarabine and total body irradiation, he had allogeneic hematopoietic stem cell transplantation (HSCT) from his brother as a HTLV-1–negative donor. He was stable in 3 months after HSCT, but he then developed tremor and nausea. Magnetic resonance imaging of the head disclosed multiple subcortical high signals in fluid-attenuated inversion recovery (FLAIR) sequence, and flow cytometry of the spinal tap showed CD7-negative and CCR4-positive cell population. Skin biopsy showed infiltration with CCR4-positive abnormal lymphocytes.
Four months after HSCT, he noticed blurred vision in the right eye and showed aqueous hypopyon in the right eye (Figure 2B). The fundus in the right eye was normal. The left eye had nothing particular. The best-corrected visual acuity was 1.2 in both eyes. Cytological examination of aqueous tap showed atypical cells with Class V (Figure 2A). With the diagnosis of systemic relapse, he underwent 3 courses of mogamulizumab and 2 courses of CHOP, followed finally by lenalidomide. Five months after HSCT, he developed graft-versus-host disease at stage IV, manifesting as generalized skin edema and erythema, and underwent steroid pulse therapy. He was stable for the following 7 months but developed abdominal fullness about 1 year after HSCT. Computed tomographic scan showed peritoneal thickening with ascites, and abdominal paracentesis disclosed abnormal lymphoid cells. He underwent 2 courses of CHOP. He showed no intraocular infiltration with the best-corrected visual acuity of 0.9 in the right eye and 0.2 in the left eye. The left eye had corneal surface damage after graft-versus-host disease.

Case 2. A 39-year-old man with aqueous pseudohypopyon in the right eye (arrowhead, B). Cytology of aqueous tap demonstrates class V abnormal cells with flower-like convoluted nuclei in Papanicolaou stain (A). Bar = 50 µm.
Methods
To analyze historical cases from the literature, the Japanese literature was searched for the key words “adult T-cell leukemia/lymphoma (in Japanese)” and “ocular (in Japanese)” or “eye (in Japanese)” in the bibliographic database of medical literature in Japanese (Igaku Chuo Zasshi, Japana Centra Revuo Medicina, Ichushi-Web), published by the Japan Medical Abstracts Society (JAMAS). Old literatures were further collected from references cited in the articles identified during the literature search. PubMed was also searched for the key words “adult T-cell leukemia/lymphoma” and “ocular” or “adult T-cell leukemia/lymphoma” and “eye.” The sufficient description was found in 16 Japanese patients who showed pathologically proven intraocular infiltration with ATLL (Table 1).7-22
Review of 18 Patients With Pathologically Proven Intraocular Infiltration With Adult T-Cell Leukemia/Lymphoma (ATLL) Including the Present 2 Patients.
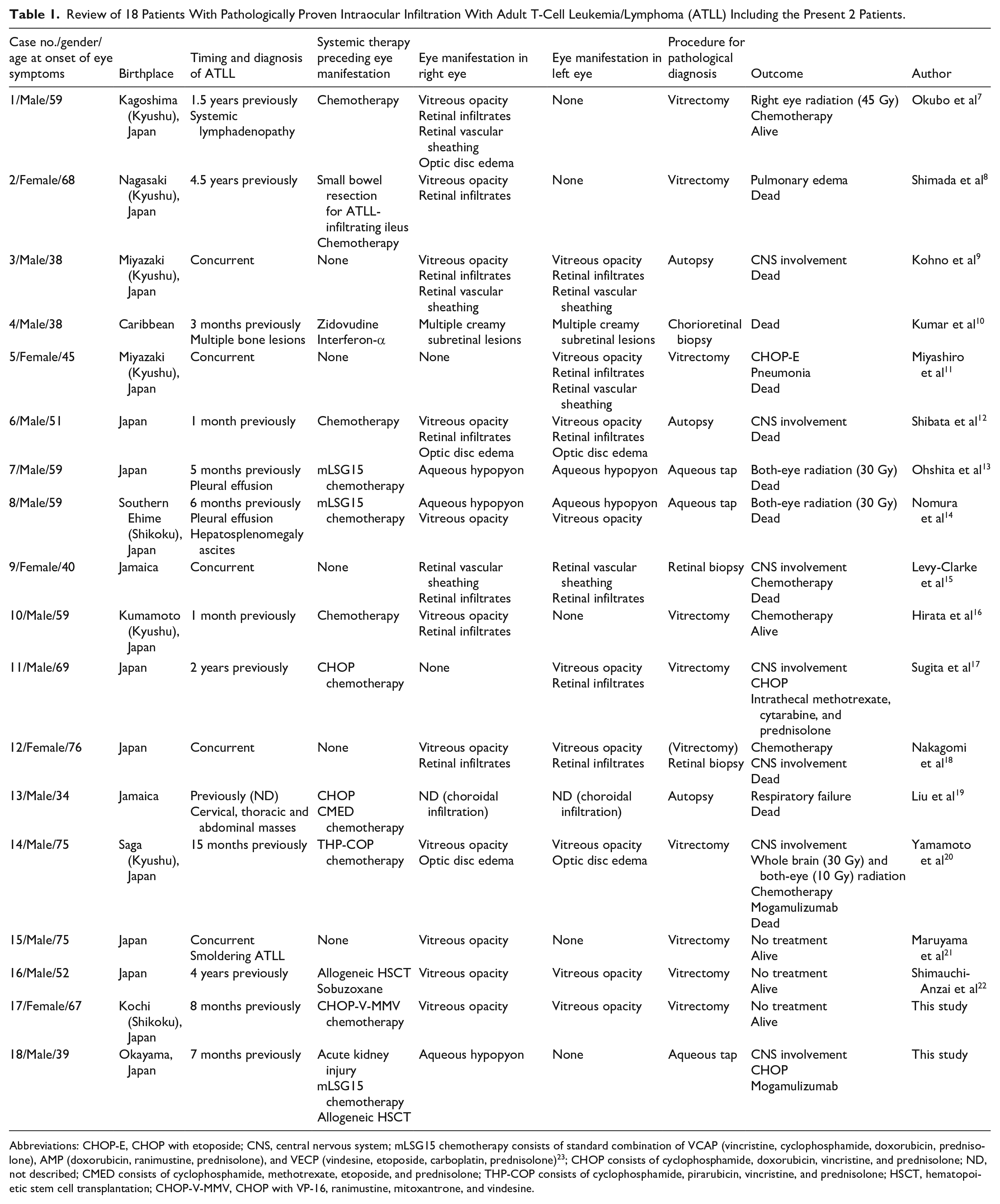
Abbreviations: CHOP-E, CHOP with etoposide; CNS, central nervous system; mLSG15 chemotherapy consists of standard combination of VCAP (vincristine, cyclophosphamide, doxorubicin, prednisolone), AMP (doxorubicin, ranimustine, prednisolone), and VECP (vindesine, etoposide, carboplatin, prednisolone) 23 ; CHOP consists of cyclophosphamide, doxorubicin, vincristine, and prednisolone; ND, not described; CMED consists of cyclophosphamide, methotrexate, etoposide, and prednisolone; THP-COP consists of cyclophosphamide, pirarubicin, vincristine, and prednisolone; HSCT, hematopoietic stem cell transplantation; CHOP-V-MMV, CHOP with VP-16, ranimustine, mitoxantrone, and vindesine.
Results
The 18 patients, including the present 2 patients, were 13 men and 5 women, with the age at the onset of eye symptoms ranging from 34 to 76 (median = 59) years (Table 1). All 18 patients were Japanese living in southwest part of Japan, except for 3 Caribbean patients. The eye manifestations were vitreous opacity only in 3 patients, aqueous pseudohypopyon only in 2, the combination of vitreous opacity and aqueous pseudohypopyon in 1, vitreous opacity with retinal infiltrates in 8, retinal (choroidal) infiltrates only in 3, and vitreous opacity with optic disc edema in 1. Both eyes were involved in 12 patients, while 6 patients showed unilateral eye involvement. The onset of eye manifestations was concurrent with systemic manifestations in 5 patients, while the eye manifestations developed later in the period ranging from 1 month to 4.5 years (median = 8 months) after chemotherapy or allogeneic HSCT for ATLL in 13 patients. After pathological diagnosis of intraocular involvement, 6 patients underwent additional chemotherapy, 2 had radiation to both eyes, 1 had right eye radiation combined with chemotherapy, and 1 had whole brain and both-eye radiation combined with chemotherapy. Mogamulizumab was given in combination with conventional chemotherapy in 2 patients. Death was described in 11 patients, and 6 of them had central nervous system involvement.
Pathological diagnosis of intraocular involvement was made by vitrectomy in 9 patients, aqueous tap in 3, retinal or choroidal biopsy in 3, and autopsy in 3. Cytological diagnosis of vitreous aspirates or vitrectomy fluid or aqueous tap was based on abnormal cells with flower-like convoluted nuclei, so-called flower cells. Retinal (chorioretinal) biopsy10,15,18 or autopsy9,12,19 showed perivascular infiltration with abnormal cells in the neuroretina or subretinal pigment epithelial infiltration. Autopsy in 1 patient showed infiltration with abnormal cells in the choroid. 19
Discussion
In the first patient of the present study, bilateral vitreous opacity in a patient with ATLL could be easily diagnosed as infiltration with leukemia/lymphoma cells. The patient and her family wished to have better vision in the late stage of uncontrolled leukemia. Vitrectomy in both eyes was thus done to improve the vision in this patient who even had bilateral optic disc atrophy probably due to the adverse effect of chemotherapy. Cytology of vitreous aspirates demonstrated unequivocally ATLL cells (Figure 1A). The white retinal lesions in both eyes would be subretinal or subretinal pigment epithelial infiltration with ATLL cells. Vitrectomy for clearing vitreous infiltrates would be useful for improving the quality of vision even in the late stage of uncontrolled ATLL. Perspective for the expected vision after vitrectomy should be discussed well with the patient and family members since other complications such as optic disc atrophy would be present.
In the second patient of the present study, hypopyon appeared after allogeneic HSCT, which is the current standard treatment in relapse after chemotherapy for ATLL. 24 Hypopyon was easily diagnosed clinically as relapse of ATLL. With pathological diagnosis of aqueous aspirate as class V, the patient underwent additional chemotherapy combined with mogamulizumab as the current standard therapy.25,26 Renal failure in the initial phase of the disease in this patient would be attributed to direct infiltration with ATLL in the kidney. 27
Vitreous opacity and pseudohypopyon are 2 clinical features of intraocular lymphoma, which may be either primary or secondary infiltration into the eyeball. Primary intraocular lymphoma presents as vitreous opacity or subretinal infiltrates or their combination, and occurs also in association with primary central nervous system lymphoma.28-30 Other types of systemic lymphoma may infiltrate secondarily into the eyeball and present vitreous opacity or subretinal infiltrates or their combination. 31 Pseudohypopyon is a rare presentation of intraocular relapse of lymphoma or leukemia.29,32 The signs of vitreous opacity or aqueous hypopyon have to be differentiated from inflammation, which is caused by different types of uveitis. 33 In the present 2 patients, either vitreous opacity or pseudohypopyon was observed as a sign of relapse after systemic chemotherapy or HSCT. ATLL would take a course of relapse to present signs of intraocular infiltration that are similar to primary intraocular lymphoma28-30 or secondary infiltration of other types of systemic lymphoma.31,32
In the review of literature, all 16 patients with pathological diagnosis of intraocular ATLL infiltration were from Japan or Caribbean Islands where HTLV-1 infection is prevalent. The frequent manifestations of intraocular infiltration with ATLL were retinal infiltrates with vitreous opacity. Thus, vitreous cytology by vitrectomy or vitreous aspirates was the predominant method to reach the pathological diagnosis. As for a clinical question in this review, the timing of pathologically proven intraocular infiltration was frequently at the time point of relapse of ATLL after chemotherapy and also after allogeneic HSCT. The prognosis after the pathologically proven intraocular infiltration with ATLL was basically poor often due to the central nervous system involvement.
In conclusion, the present study focused on the pathologically proven intraocular infiltration with ATLL. So far only 16 cases with the pathologically proven intraocular infiltration have been reported in the literature, in addition to the present 2 patients. The clinical features of intraocular infiltration such as vitreous opacity, aqueous pseudohypopyon, and retinal infiltrates in ATLL are basically the same as primary intraocular lymphoma and secondary infiltration with other types of systemic lymphoma.
Footnotes
Authors’ Note
Data are available on reasonable request to the corresponding author.
Author Contributions
TM, as an ophthalmologist, followed 2 patients (Case 1 and Case 2) and did vitrectomy in Case 1. TS, as an ophthalmologist, followed Case 2. TT, as a pathologist, made the diagnosis. AY and HT, as hematologists, followed and treated Case 2. TM wrote the manuscript, and TS, TT, AY, and HT did critical review of the manuscript. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics committee review was not applicable to case reports, based on the Ethical Guidelines for Medical and Health Research Involving Human Subjects, issued by the Government of Japan.
Informed Consent
Written informed consent for vitrectomy or aqueous tap was obtained from the patients. Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.