
Abstract
IgG4-related disease is a recently established clinical entity. The disease might serve as the background for later development of systemic lymphoma. This study aims to confirm the diagnosis of IgG4-related disease by re-staining lacrimal gland lesions diagnosed previously with low-grade lymphoma in a patient who developed systemic diffuse large B-cell lymphoma (DLBCL) 18 years later. A 53-year-old man developed bilateral lacrimal gland swelling and right submandibular gland swelling and was diagnosed by excision as low-grade lymphoma. In follow-up, positron emission tomography showed high uptake in the median hyoid 11 years later but no malignancy was detected by laryngeal submucosal biopsy. He was well with no treatment until 18 years later when he had palatal swelling and was diagnosed with DLBCL by oral floor biopsy. He had systemic lymphadenopathy, infiltration in paranasal sinuses, hypopharynx, small intestine, kidney, and prostate. He underwent 8 courses of R-CHOP and 3 courses of high-dose methotrexate and achieved complete remission with no relapse for 1 year thereafter. Re-immunostaining of paraffin blocks of bilateral lacrimal gland lesions showed IgG and IgG4-positive lymphocytes and plasma cells among lymphoid follicles separated by fibrous bundles, with 10 or more IgG4-positive cells in high-power field. The IgG4/IgG-positive cell ratio was 100% and the number of κ chain-positive cells and λ chain-positive cells was the same. The bilateral lacrimal lesions were thus re-diagnosed as IgG4-related disease. In conclusion, systemic DLBCL occurred approximately 20 years after lacrimal gland IgG4-related disease. Literature review revealed 12 patients with IgG4-related disease, including the present patient, who later developed lymphoma in the other organs.
Keywords
Background
IgG4-related disease is a multisystem disease which is characterized by infiltration with IgG4-producing plasma cells in association with fibrotic changes in various organs. 1 The diagnosis of IgG4-related disease is confirmed by pathological diagnosis which is based mainly on IgG4 immunostaining of excised tissue or biopsy specimen. The comprehensive diagnostic criteria for IgG4-related disease was established as recently as in 2011, 2 and since then, the standard pathological procedure, 3 based on the common understanding of the disease, has been advanced in Japan as well as in the other parts of the world. 4
The lacrimal glands in the orbital space are common sites involved not only with IgG4-related disease5-8 but also with malignant lymphoma.9-12 Under the circumstances, lacrimal gland masses have to be differentially diagnosed in the list of lymphoma and inflammation including IgG4-related disease and other inflammatory diseases.13,14 As blood examinations, serum soluble interleukin-2 receptor (sIL-2R) would be elevated in lymphoma as well as inflammation including sarcoidosis and IgG4-related disease. 8 Serum IgG4 measurement would help make the diagnosis of IgG4-related disease, based on the clinical criteria, 135 mg/dL or higher.2,5
In this study, we present a patient with systemic diffuse large B-cell lymphoma who was diagnosed 18 years previously as IgG4-related disease in bilateral lacrimal glands by re-immunostaining of the preserved pathological specimens. We also review the literature15-21 to answer a clinical question whether IgG4-related disease might be the background, or more specifically, the predisposition for the later development of lymphoma.
Case Report
A 53-year-old man with no history noticed a submandibular mass on the right side, together with palpable bilateral lacrimal gland enlargement (Figure 1A) in 1999. Half a year later, he underwent extirpation of the right submandibular gland under general anesthesia by an otolaryngologist, but the pathology was suspicious of low-grade lymphoma. Two years later from the initial visit, he then underwent complete extirpation of bilateral lacrimal gland masses under general anesthesia and the pathological report stated low-grade lymphoma. The patient was followed with no additional treatment. Eight years later from the initial visit, whole-body 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) showed an abnormal uptake site on the lymph node around the left submandibular gland (maximum of standardized uptake value [SUVmax] = 4.08, Figure 1B). Eleven years later from the initial visit, he noticed palpable enlargement of the lacrimal gland on the left side. FDG-PET showed abnormal uptake in the left lacrimal gland (SUVmax = 3.21, Figure 1C) and in a median mass at the level of hyoid bone (SUVmax = 4.38, Figure 1D). Biopsy of the laryngeal submucosal lesion showed no evidence of malignancy and the patient chose observation for the left lacrimal gland mass.
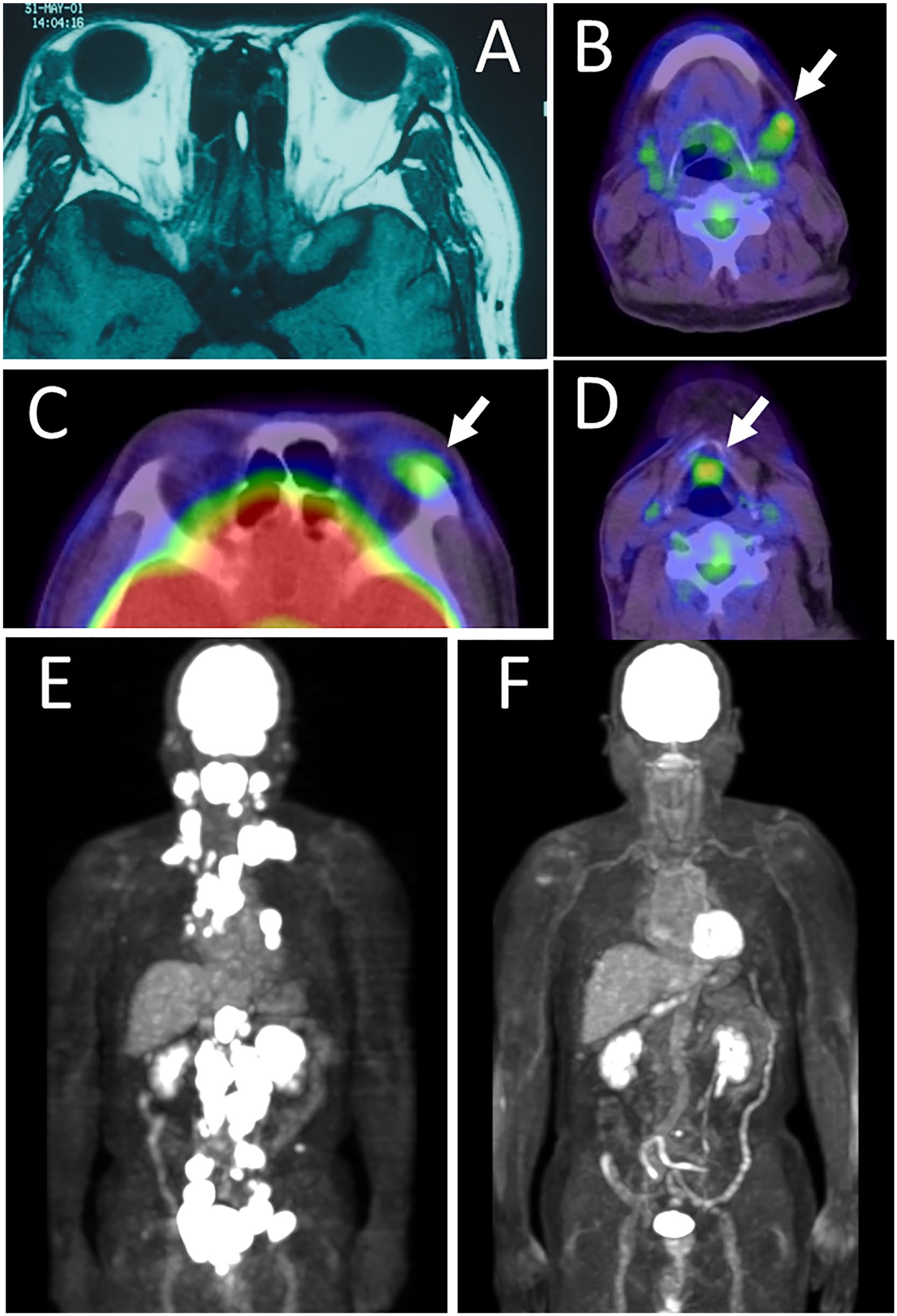
Bilateral lacrimal gland masses in magnetic resonance imaging 2 years later from the initial visit (A). High uptake (maximum of standardized uptake value [SUVmax] = 4.08) in a lymph node around left submandibular gland by whole-body 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) 8 years later from the initial visit (arrow, B). High uptake in left lacrimal gland (SUVmax = 3.21, arrow, C) and in a median mass at the level of hyoid bone (SUVmax = 4.38, arrow, D) by FDG-PET 11 years later from the initial visit. Abnormal high uptake sites in massive lymphadenopathy from the cervix to pelvis 20 years later from the initial visit (E) and no abnormal uptake in complete remission after chemotherapy 21 years later from the initial visit (F).
He was well for the following 9 years until 20 years later from the initial visit when he complained of laryngeal discomfort and was found to have palatal swelling. In a few months, biopsy of a mass in the floor of the oral cavity showed diffuse large B-cell lymphoma. The biopsy specimen showed diffuse infiltration with large anomalous cells with large irregularly shaped nuclei (Figure 2A) which were positive for CD20 (Figure 2B) and MUM-1 (Figure 2D). The smaller number of CD3-positive small lymphocytes were also present (Figure 2C). Ki-67 labeling index was high at 90% (Figure 2E). IgG4 was negative and Epstein-Barr virus (EBV)-encoded small RNAs (EBER) in situ hybridization was negative. FDG-PET showed multifocal abnormal uptake along systemic lymphadenopathy from the cervix (SUVmax = 32.1 in submental lymph node) to the pelvis and also in extranodal lesions of Waldeyer tonsillar ring, ethmoid sinus mucosa, soft palate, left hypopharynx, bilateral parotid glands, small intestine, left kidney (SUVmax = 34.1), and prostate (Figure 1E). The patient had no B symptoms and was on Stage 4A. The performance status was 1, the enhanced International Prognostic Index (NCCN-IPI) was high-intermediate, and the central nervous system (CNS)-IPI was at high risk. In half a year, he underwent 8 courses of R-CHOP (rituximab 375 mg/m2 Day 1, cyclophosphamide 750 mg/m2 Day 1, doxorubicin 50 mg/m2 Day 1, vincristine 1.4 mg/m2 Day 1, and prednisolone 100 mg Day 1-5) and then 3 courses of high-dose methotrexate (1500 mg/m2, reduced dose based on the age of 65 years or older) as prophylactic treatment for central nervous system infiltration. He was in complete remission (Figure 1F) and had no treatment for the following 1 year, 22 years from the initial visit.

Diffuse large B-cell lymphoma in biopsy specimen at floor of mouth 20 years later from the initial visit. Diffuse infiltration with large irregularly shaped cells with large nuclei (A), which are positive for CD20 (B), MUM-1 (D), and Ki-67 (E). Small lymphocytes in the lesion are positive for CD3 (C), indicative for T cells. Ki-67 labeling index is high at 90% (E). White scale bar = 100 µm in B-E, bar =50 µm in A.
Methods
Paraffin sections were cut from paraffin blocks of bilateral lacrimal gland masses and the laryngeal submucosal lesion in the present case. Immunohistochemical staining was done by the protocol for Bond Polymer Refine Detection Kit in the system of Bond-III Fully Automated IHC and ISH Stainer (Leica Biosystems, Welzlar, Germany). Primary antibodies were mouse monoclonal antibodies against CD3 (Leica NCL-L-CD3-565, Leica Biosystems Novocastra), CD20 (Leica NCL-L-CD20-L26), IgG4 (MBL BS-MCO11, Medical & Biological Laboratories, Nagoya), IgG ((Leica NCL-L-IgG), and Ki-67 (Leica NCL-L-Ki67-MM1). Both κ light chain and λ light chain were detected by in situ hybridization using probes, Bond Ready-to-Use ISH Kappa Probe (PBO0645, Leica Biosystems) and Lambda Probe (PBO0669). 8 Re-immunostaining of the preserved specimen of series of previous patients was approved as a retrospective observational study by the Ethics Committee of Okayama University Graduate School of Medicine, Dentistry, and Pharmaceutical Sciences and Okayama University Hospital (identifier, 2101-002).
Results
In the present case, bilateral lacrimal gland lesions 2 years later from the initial visit showed common features of lymphoid follicles separated by fibrous bundles (Figure 3A and 3B on the right side, Figure 4A and 4B on the left side). Small lymphocytes and plasma cells, especially in interfollicular areas, were positive for IgG and IgG4, fulfilling the criteria of more than 10 IgG4-positive cells in a high-power field. The ratio of IgG4-positive cells / IgG-positive cells was 100% on both sides (Figure 3C and 3D on the right side, Figure 4C and 4D on the left side). The number of κ light chain-positive cells and λ light chain-positive cells were almost the same, indicative of no clonal restriction to either κ chain or λ chain, on both sides (Figure 3E and 3F on the right side, Figure 4E and 4F on the left side). The pathological diagnosis was confirmed as IgG4-related disease of the bilateral lacrimal glands. The laryngeal submucosal lesion 11 years later from the initial visit showed that predominant B cells (Figure 5B) were mixed with the small number of T cells (Figure 5C) in lymphoid tissue (Figure 5A). There were no Ki-67-positive cells (Figure 5D) or IgG4-positive cells (Figure 5E). The re-immunostaining of the laryngeal submucosal lesion confirmed no evidence of malignancy.

IgG4-related disease in the right lacrimal gland mass 2 years later from the initial visit. Lymphoid follicles separated by fibrotic bundles (A) and infiltration with plasma cells and lymphocytes (B). IgG4 (D) / IgG (C) = 100%. Both κ chain (E) and λ chain (F) are equally positive. White scale bar = 100 µm in B-F, bar =500 µm in A.
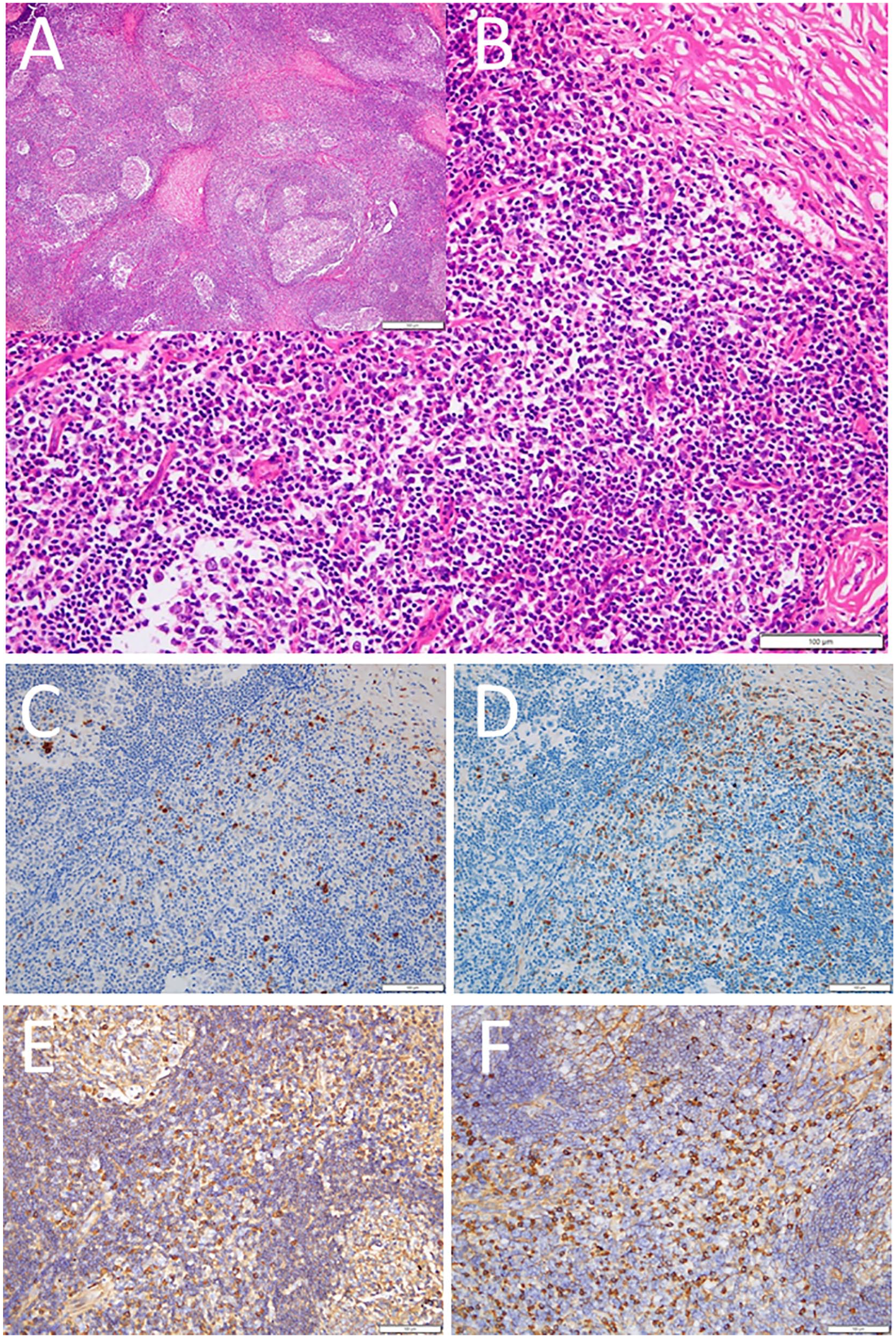
IgG4-related disease in the left lacrimal gland mass 2 years later from the initial visit. Lymphoid follicles separated by fibrotic bundles (A) and infiltration with plasma cells and lymphocytes (B). IgG4 (D)/IgG (C) = 100%. Both κ chain (E) and λ chain (F) are equally positive. White scale bar = 100 µm in B-F, bar =500 µm in A.

Restaining of the laryngeal submucosal lesion 11 years later from the initial visit. Small lymphocytes in lymphoid tissue (A) consisting of predominant CD20-positive B cells (B) and the small number of CD3-positive T cells (C). Note no Ki-67-positive cells (D) or IgG4-positive cells (E). White scale bar = 200 µm.
Discussion
The present patient developed submandibular gland enlargement on the right side and lacrimal gland enlargement on both sides at the same time of the initial phase of the disease around the year 2000 when the entity of IgG4-related disease had not yet been established. The pathological diagnosis of the excised submandibular gland at the first surgery remained obscure from the viewpoint of malignancy, and thus at the second surgery, the excision of bilateral lacrimal glands was performed, but with the indefinite pathological diagnosis. The patient was followed for 20 years with no treatment until the development of systemic malignant lymphoma because the right submandibular gland and the bilateral lacrimal glands had been extirpated completely.
Re-immunostaining of the bilateral lacrimal gland tissues confirmed the pathological diagnosis of IgG4-related disease in this study. The tissue for the right submandibular gland has been lost and could not be reexamined by immunostaining. Bilateral lacrimal gland enlargement and the right submandibular gland enlargement in this patient are indeed consistent with the diagnosis of Mikulicz disease which is now recognized as IgG4-related disease. In a previous case report, a middle-aged man with long-term history of Mikulicz disease with enlargement of the salivary and lacrimal glands developed later a renal pelvic mass which was diagnosed pathologically as IgG4-related disease, and finally at autopsy, he was diagnosed as systemic diffuse large B-cell lymphoma (Case 5 in Table 1). 17 The course of that patient is similar to the course of the present patient.
Review of 12 Patients, Including the Present Patient, With IgG4-Related Disease Who Later Develop Lymphoma in Other Organs.

Abbreviation: DLBCL, diffuse large B-cell lymphoma.
Case reports have been accumulated to support the fact that IgG4-related disease would serve as the background, or more specifically, the predisposition for the later development of lymphoma in the other parts of the body.15-21 As review of the literature, Table 1 summarizes 12 patients with IgG4-related disease, including the present patient, who later developed lymphoma in the other organs.15-21 Patients with concurrent development of IgG4-related disease and lymphoma,22,23 those with lymphoma who were later diagnosed as IgG-related disease,24-26 and those with IgG4-related disease and lymphoma occurring in the same organ 27 are not included in the review of literature in Table 1. We, in fact, experienced a woman at the initial presentation with extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) in the bilateral lacrimal glands. She was later diagnosed as IgG4-related disease in the unilateral lacrimal gland, and after a while, developed paracardiac MALT lymphoma in the long-term follow-up.7,8 The present patient further reinforces the sequence of events that the background of IgG4-related disease would lead later to the development of lymphoma in the different part of the body. However, it still remains controversial whether IgG4-related disease would be a precipitating event for the development of malignancies including lymphomas.28-31
The 12 patients, including the present patient, in Table 1 were 2 women and 10 men, with the age at the diagnosis of IgG4-related disease ranged from 53 to 74 years (median, 66 years). IgG4-related disease was diagnosed as autoimmune pancreatitis in 3 patients, sclerosing cholangitis in 2, sclerosing sialadenitis with or without sclerosing dacryoadenitis in 5, prostatitis in 1, and lymphadenopathy in 1. The interval between the initial diagnosis of IgG4-related disease and the later diagnosis of lymphoma ranged from 2 to 18 years (median, 4 years). The pathological diagnosis of lymphoma was diffuse large B-cell lymphoma (DLBCL) in 10 patients, B-cell lymphoma in 1 patient, and peripheral T-cell lymphoma in 1 patient (Case 4). The manifestation of lymphoma was lymphadenopathy in 10 patients, a liver mass in 1 patient, and bilateral renal masses in 1 patient. These series of 12 patients would support the clinical question that IgG4-related disease might be the precipitating event for the later development of lymphoma. Even with the clinical evidence, we could not exclude completely the possibility that lymphoma, mostly DLBCL, might occur by chance in those patients with the preceding diagnosis of IgG4-related disease.28-31
In conclusion, the establishment of diagnostic criteria for IgG4-related disease can lead to definite pathological diagnosis of IgG4-related disease in the preserved tissue of the lacrimal glands of the present patient. IgG4-related disease should be followed carefully since the condition may be the background or the predisposition for later development of systemic lymphoma.
Footnotes
Authors’ Note
Data are available upon reasonable request to the corresponding author.
Author Contributions
TM as an ophthalmologist and KO as an oncologist treated and followed the patient. TT and KN as pathologists made the diagnosis. TM wrote the manuscript, and TT, KN, and KO did critical review of the manuscript. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics committee review was not applicable to case reports, based on the Ethical Guidelines for Medical and Health Research Involving Human Subjects, issued by the Government of Japan.
Informed Consent
Verbal informed consent was obtained from the patient for his anonymized information to be published in this article.