
Abstract
Supine orthostatic hypertension with orthostatic hypotension is an autonomic dysfunction where the patients present with hypertension when supine and with decrease in blood pressure while bearing an upright posture. We report on a 74-year-old male who was admitted with dizziness and was found to have profound orthostatic hypotension with supine hypertension. The patient also developed orthostatic paroxysmal premature ventricular beats as well as nonsustained ventricular tachycardia. In this report, we attempt to present the possible mechanism of orthostatic ventricular tachycardia in our patient and the overview of the treatment strategies used in management of patients with supine hypertension and orthostatic hypotension.
Case Report
A 74-year-old Caucasian male with a history of hypertension, stroke 4 years ago, hypothyroidism, and profound deafness was admitted to the hospital with episodes of orthostatic dizziness and disorientation. Sometimes these episodes would result in loss of balance and fall. He denied any chest pain and complete loss of consciousness.
The patient was admitted to the telemetry and started having premature ventricular contractions (PVCs) and runs of nonsustained ventricular tachycardia (NSVT). Physical examination of the patient revealed a significant orthostatic blood pressures drop from supine 155/79, to sitting 110/69, and standing 88/58 with no fluctuation in heart rate.
The patient was also having PVCs and NSVT on standing up (Figure 1). He would then get disoriented and would be unaware of his surroundings. His echocardiogram revealed a normal ejection fraction without any significant structural heart disease. Given his episodes of NSVT, he underwent a stress test as well. His stress test revealed a medium size and a moderate intensity reversible defect in anteroseptal area. The patient subsequently underwent coronary angiography that revealed a triple vessel coronary artery disease (Figures 2-4) and the patient was sent for coronary artery bypass surgery.

Rhythm strip shows wide complex ventricular tachycardia with a rate of close to 200 beats per minute.
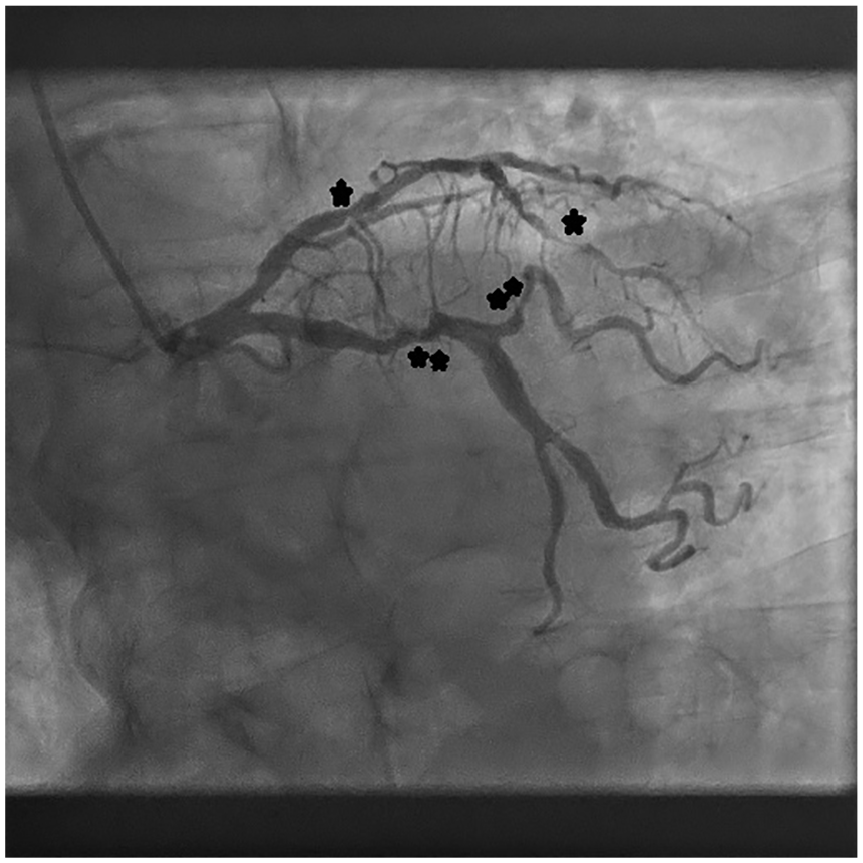
Coronary angiography showing significant narrowing in the left anterior descending artery (*) and left circumflex artery (**).
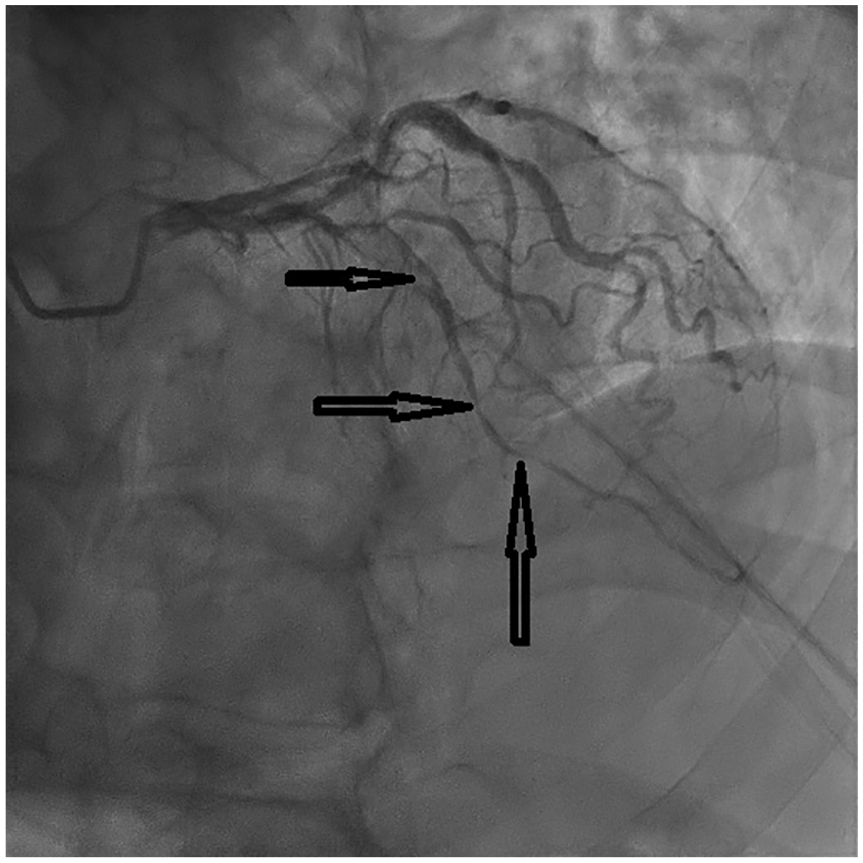
Coronary angiography with arrows pointing toward significant narrowing in the left anterior descending.

Coronary angiography with arrow pointing toward significant narrowing in the right coronary artery.
The patient was started on pyridostigmine and fludrocortisone and his orthostatic drop in blood pressure improved along with orthostatic ventricular tachycardia. After surgical revascularization, the patient continued to be on pyridostigmine and was not having any recurrent ventricular tachycardia. The patient was seen in the follow-up in the arrhythmia clinic and was not having any palpitations. The patient also had an event monitor that showed no episodes of ventricular tachycardia.
Discussion
Normal standing increases pooling of more than half a liter of blood to the dependent body compartments, which significantly lowers venous return and eventually affecting cardiac output, leading to decreased blood pressure. This initiates a compensatory reflex mechanism in the carotid sinus and aortic arch. 1 This compensatory mechanism leads to a boost in cardiac output, preventing the decrease in the blood pressure caused by changing to an upright, standing position. This is attained by upregulating the sympathetic outflow and at the same time downregulating the parasympathetic outflow. Once this reflex mechanism fails, orthostatic hypotension (OH) results in cerebral decreased perfusion, which eventually leads to orthostatic intolerance and can present with a spectrum of symptoms ranging from dizziness, presyncope, to syncope.
As eluded earlier, supine orthostatic hypertension (SH) with OH is a form of hypertension where the patient presents with hypertension when supine and a significant decrease in blood pressure when the patient bears a standing or upright position. 2
SH/OH can develop in a majority of patients with OH and autonomic dysfunctions and failure, which is characterized by inhibition of sympathetic outflow because the postganglionic neurons are limited and deficient in the release of norepinephrine, particularly when assuming an upright posture.3-5
This can lead to SH and, most likely due to deficient baroreflex function, inadequate natriuresis, and residual sympathetic output in the setting of hypersensitive postsynaptic adrenergic receptors and this can explain autonomic failure as a significant risk factor for SH/OH. 6 Long-term hypertension can cause desensitization and downregulation of the baroreceptor reflex mechanisms, which can be a contributing factor to the development of SH/OH. Additional contributing mechanism to SH/OH is residual sympathetic tone acting on postsynaptic adrenergic receptors that have become hypersensitive. This can lead to the conclusion that long-standing hypertension might be a risk factor for developing OH due altered sensitivity of adrenergic and baroreceptors, especially when assuming a standing and upright position.1,2
OH because of autonomic failure (primary or secondary) can develop SH in some occasions, and that could be due to the pharmacological treatment of OH. It can also be due to baroreflex dysfunction with coexistence of residual sympathetic outflow, especially in patients with central autonomic degeneration. 4
Our patient had a significant orthostatic drop in his blood pressure and he also had runs of PVC and runs of NSVT on assuming upright posture. There are 2 mechanisms that could explain orthostatic ventricular tachycardia in our patient.
Our patient had significant coronary artery disease and it is possible with OH he would have been experiencing further worsening of his coronary perfusion resulting in coronary ischemia and PVCs and NSVT secondary to worsening ischemia.
The other mechanism could have been orthostatic surge in sympathetic tone precipitating PVCs and NSVT. There have been reports of orthostatic surge in catecholamine levels in patients with OH, which could trigger ventricular ectopy and ectopic ventricular tachycardia. 7 This catecholamine surge could have led to triggering of PVC and NSVT from an ischemic focus in our patient. When the orthostatic drop in his blood pressure improved, we noticed improvement in orthostatic ventricular ectopy and NSVT.
Management of patient suffering from SH/OH can be challenging. Patient education is important and emphasis should be made for the management of autonomic dysfunction, more importantly when SH is also present. The goals of therapy should be to improve quality of life. On the other hand, good control of blood pressure is important to prevent end-organ damage. However, permissive hypertension may be acceptable in some cases where OH is profound.1,2
Autonomic stressors (eg, arduous workout, sudden change in position withstanding, and heavy meals) should be avoided if possible. Medications that affect vascular tone or heart rate should also be avoided or reduced as medically indicated. Increasing salt and water intake is helpful for some patients. Maneuvers like sitting for few minutes prior to standing and keeping the head on the bed elevated while sleeping can be helpful. Compression stockings are particularly important for patients with significant blood pooling in the lower extremities. Finally, engaging in exercise routines and is highly advised to increase volume and left ventricular mass, thereby improving cardiac output and blood pressure. If exercises that require upright posture are not well tolerated, exercises, not requiring such posture, such as recumbent biking, may be beneficial to start.1-4
Many patients improve with conservative measures only. However, some continue to be symptomatic and require other intervention. One of the things important to understand is, medications for the treatment of OH will exacerbate SH and vice versa. The optimal medical regimen is often reached after multiple rounds of trial and error, and it is important to recognize that combination therapy may be required in some patients.
Table 1 summarizes some of the studies on medications for treatment of autonomic dysregulation. Midodrine, which is α1-agonist, helps by boosting the vascular tone and decreases the risk of developing OH. 5 Midodrine has rapid pharmacokinetics and is therefore taken 3 to 4 times a day. It is typically recommended that patients take a pill in the morning before getting out of bed. In addition, it is recommended for patients to avoid bedtime doses to prevent SH.
Summary of Studies on Medications to Treat Autonomic Dysregulation.

Abbreviations: IOT, idiopathic orthostatic tachycardia; IV, intravenous; POTS, paroxysmal orthostatic tachycardia syndrome; HR, heart rate; DBP, diastolic blood pressure.
Droxidopa also boosts the vascular tone. Droxidopa is a synthetic amino acid that acts as a precursor of norepinephrine. Droxidopa can, however, cause accelerated hypertension. 6
Clonidine, which is centrally acting α2-agonist, can be used in certain cases. This is due to decreased sympathetic activity in the symptomatic individuals with autonomic dysfunction allows the peripheral effects of this centrally acting α2-agonist to predominate. Therefore, clonidine does not significantly affect blood pressure, in contrast to what is seen in normal individuals. Fludrocortisone is a mineralocorticoid that improves blood pressure through its action on the nephron for increased sodium and water reabsorption. Also, desmopressin acetate causes water retention by increasing water permeability in the renal tubular cells. This occurs independent of sodium, making this drug less likely to cause hypertension when compared with fludrocortisone. Serotonin and norepinephrine reuptake inhibitors may also be used, as they improve OH without causing hypertension. Similarly, the peripheral acetyl cholinesterase inhibitor pyridostigmine also improves OH without having any negative consequence on SH.8,9
Pyridostigmine acts at the ganglionic level by increasing transmission, which is minimal when lying down and peaks in the upright standing position. Thus, pyridostigmine is unlikely to cause SH in this subgroup of patients. 8 Finally, immunomodulation therapy, such as intravenous immunoglobulins, steroids, mycophenolate mofetil, and plasmapheresis, may be effective in appropriately selected patients. This strategy was tested and found to be highly effective where autoimmune state is believed as the main cause of autonomic dysfunction and failure.8-10
We initiated our patient on pyridostigmine and fludrocortisone. His orthostatic drop in blood pressure improved and he had no orthostatic paroxysmal episodes of ventricular tachycardia. The patient underwent coronary bypass surgery given his significant coronary artery disease. After surgical revascularization, the patient continued to be on pyridostigmine and was not having any recurrent ventricular tachycardia. The patient was seen in the follow-up in the arrhythmia clinic and was not having any palpitations.
Conclusion
Orthostatic paroxysmal ventricular tachycardia in patients with SH/OH may indicate an underlying structural heart disease and should be evaluated for such.
Footnotes
Authors’ Note
All authors have contributed equally to the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kanjwal is the consultant for St Jude Medical and Biosense Webster. No other author has any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information.