
Abstract
Cinacalcet use is associated with risk of hypocalcemia; however, this risk has been mostly demonstrated in patients with chronic kidney disease. In this article, we describe a case of a 59-year-old male with primary hyperparathyroidism (PHPT), hypercalciuria, osteopenia, and normal kidney function who was started on cinacalcet for the management of recurrent hypercalcemia following prior unsuccessful parathyroidectomy. Within 6 months following cinacalcet commencement, he developed symptomatic and biochemical hypocalcemia requiring discontinuation of the medication and initiation of calcium supplementation. Over more than 3 years of follow-up, his calcium supplementation was gradually tapered off and then discontinued. He is presently eucalcemic and euparathyroid off calcium supplements while also demonstrating normalization of hypercalciuria and bone mineral density. These data indicate that our patient has experienced resolution of PHPT after brief exposure to cinacalcet. We recommend that low starting cinacalcet doses should be considered for treatment of hypercalcemia in patients with PHPT who underwent unsuccessful parathyroidectomy along with close clinical and biochemical follow-up.
Introduction
Primary hyperparathyroidism (PHPT) is characterized by a disproportionate release of parathyroid hormone (PTH) from the parathyroid gland resulting in hypercalcemia. 1 PHPT is the most common cause of hypercalcemia in the outpatient setting. 1 The incidence is 1% to 2% in the adult population and increases with age. Diagnosis of PHPT is made by the presence of hypercalcemia in the setting of an elevated or normal PTH level. 2 Since the 1970s, with an increase in frequency of multichannel biochemical screenings, the PHPT clinical presentation has changed from symptomatic (eg, nephrolithiasis, fractures, and abdominal pain) to more asymptomatic.2,3
Parathyroidectomy (PTx) is an effective PHPT treatment option with >95% success rate. 2 Also it is the only definitive therapeutic option. 4 However, not all patients are considered surgical candidates, and thus, medical management of PHPT is sometimes required to alleviate clinical manifestations of hypercalcemia. In 2004, Cinacalcet hydrochloride (Sensipar) was approved by the Food and Drug Administration for patients with parathyroid carcinoma or secondary hyperparathyroidism with chronic kidney disease on dialysis. 5 In 2011, a third indication was added for the management of hypercalcemia in adult patients with PHPT for whom PTx would be indicated, but who are unable to undergo PTx.2,5
Cinacalcet is a calcimimetic that works as an allosteric modulator of the calcium sensing receptor (CaSR) in chief cells of the parathyroid gland; it increases the sensitivity of the CaSR to calcium leading to a decrease in PTH and calcium levels. 6 Cinacalcet has a short half-life and is administered twice daily in the patients with normal renal function to maintain its calcemic effects, while in the patients with chronic kidney disease on hemodialysis, the medication is administered daily.5,7
Based on its mechanism of action, hypocalcemia may not be unexpected when cinacalcet is initiated. A few case reports described symptomatic hypocalcemia following initiation of cinacalcet for treatment of secondary hyperparathyroidism in dialysis patients.6,8 Lazar and Stankus 6 described a hemodialysis patient who after 2 weeks of cinacalcet initiation has developed irreversible hypocalcemia subsequently requiring calcium supplementation after discontinuation of cinacalcet. In another report, Novick et al 8 have described a case of severe hypocalcemia resulting in cardiac arrhythmia in a hemodialysis patient induced by cinacalcet. We report here for the first time a case of a PHPT patient with normal renal function who developed transient hypocalcemia followed by sustained eucalcemia following a brief therapy with cinacalcet.
Case Description
This is a 59-year-old Caucasian man with history of hypertension, type 2 diabetes, and obesity who initially presented to endocrinology clinic in April 2013 for management of newly diagnosed PHPT. His initial laboratory values were as follows: PTH 205.6 pg/mL (14-72), serum albumin corrected calcium 10.9 mg/dL (8.5-10.2), ionized calcium 1.48 mmol/L (1.15-1.32), serum phosphate 2.5 mg/dL (2.5-4.5), urinary calcium 427.5 mg/24 h (30-400), and serum creatinine 0.9 mg/dL (0.7-1.4, estimated glomerular filtration rate [eGFR] 89 mL/min/1.73 m2; Figure 1). In addition, his dual-energy X-ray absorptiometry (DXA) scan (Lunar, GE Healthcare) results showed presence of osteopenia (Table 1), and he denied prior fractures. Patient was asymptomatic at presentation. As the patient had hypercalciuria, he was referred for PTx. Preoperative imaging studies were ordered. The thyroid ultrasound showed several benign-appearing sub-centimeter thyroid nodules—2 in the left thyroid lobe and 1 in the right thyroid lobe; none of the nodules met criteria for biopsy. The single proton emission computed tomography-computed tomography (SPECT-CT) with 99mTc-sestamibi scan showed moderate prominence of the signal in the lower pole right thyroid without presence of corresponding nodule.

Time course of patient’s serum parathyroid hormone and ionized calcium levels throughout the course of primary hyperparathyroidism management. PTx, parathyroidectomy.
Select Patient’s Biochemical and Radiological Parameters Over the Course of Primary Hyperparathyroidism Care in Endocrinology and Nephrology Clinics.
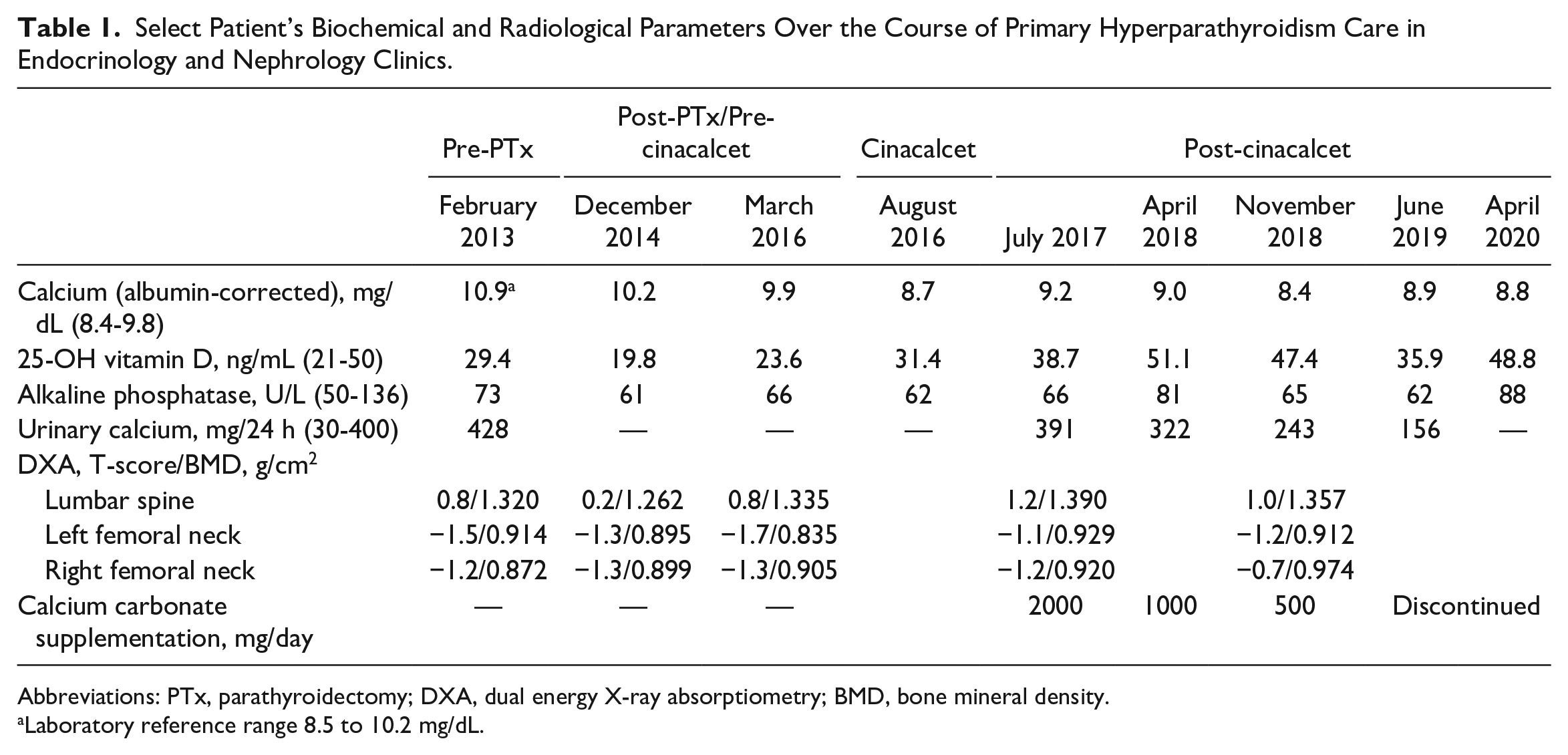
Abbreviations: PTx, parathyroidectomy; DXA, dual energy X-ray absorptiometry; BMD, bone mineral density.
Laboratory reference range 8.5 to 10.2 mg/dL.
He subsequently underwent a PTx in October 2013. During bilateral neck exploration, enlarged right inferior and left superior parathyroid glands weighing 0.7 g and 0.34 g both consistent with parathyroid adenoma on postoperative pathological examination, respectively, were excised, which, however, resulted in intraoperative PTH nadir of 133.1 pg/mL. The dissection was continued, and right thyroid nodule was removed and left inferior parathyroid gland was excised that appeared, on microscopic examination, to be benign thyroid adenoma and normal parathyroid tissue weighing 0.02 g, respectively. These surgical interventions also did not alter intraoperative elevated PTH levels. With prolonged course of the neck dissection, the right superior parathyroid gland was not located, and with the consideration of mediastinal parathyroid adenoma possibility, the surgical procedure was concluded. Less than a week after surgery, PHPT had persisted based on the laboratory findings of calcium 10.6 mg/dL (9.4-9.8) and PTH of 168.3 pg/mL. Postoperative thyroid ultrasound of the neck showed disappearance of the right thyroid nodule and stability of both left thyroid nodules. Patient underwent another SPECT-CT with 99mTc-sestamibi scan that showed again stable increased radioisotope uptake in the right mid-thyroid lobe without structural abnormalities to suggest presence of parathyroid adenoma. Surgery service has recommended against the reexploration of the neck.
Since the PTx in 2013, patient’s mild hypercalcemia was managed conservatively and his internist followed him in the clinic. His additional medical history also included hypogonadism on testosterone replacement therapy, gastric esophageal reflux disease, pancreatitis, alcoholism, and treated obstructive sleep apnea. During the follow-up evaluation in our office in March 2016, he complained of low back pain, irritability, depression, and anxiety of recent onset. On physical examination, his blood pressure was 138/83 mm Hg, and his heart rate was 60 beats/min. Body weight was 100 kg with a body mass index of 33.7 kg/m2. He was a well-appearing obese male in no acute distress. Scars were noted on neck examination from his previous PTx. The rest of his examination was otherwise unremarkable. His medications included amlodipine 5 mg daily, valsartan 160 mg daily, metformin extended-release 500 mg twice daily, cholecalciferol 1200 IU daily, omeprazole 20 mg twice daily, multivitamin daily, thiamine 100 mg daily, testosterone gel 1.62% applied 3 pumps daily, and folic acid 1 mg daily.
During the 2016 office visit, his laboratory values had not changed since 2013 showing persistent PHPT along with the stable renal function: PTH 201.4 pg/mL, ionized calcium 1.40 mmol/L, phosphate 2.2 mg/dL, and serum creatinine 0.8 mg/dL (0.7-1.4, eGFR 100 mL/min/1.73 m2). His diabetes was well controlled with hemoglobin A1c of 5.8%. Repeat DXA scan showed decline in the bone mineral density (BMD) in the left femoral neck and stable BMD in the right femoral neck BMD compared with the 2013 and 2014 studies (Table 1). Renal ultrasound was performed and did not show presence of kidney stone. Given his new neurocognitive symptoms in the setting of mild persistent hypercalcemia, we started trial of cinacalcet 30 mg daily.
Within 6 to 8 weeks of the cinacalcet therapy, his serum calcium normalized to 8.7 mg/dL (Table 1) and PTH level has reduced to 139 pg/mL; however, he has noted worsening of fatigue and “bone pain,” so we decreased the drug to 30 mg every other day as we attributed these symptoms to the relative change in his serum calcium level. During further follow-up in October 2016, his serum calcium and ionized calcium returned to levels similar to before cinacalcet was initiated and most recent complaints, so his dose was increased back to 30 mg daily (Figure 1).
In about 6 months since cinacalcet initiation, he presented to the emergency department with complaints of facial numbness and muscle spasms. Laboratory values showed hypoparathyroid hypocalcemia: PTH 6.9 pg/mL, serum albumin corrected calcium 7.2 mg/dL, and ionized calcium 0.96 mmol/L (Figure 1); serum magnesium was normal at 2.0 mg/dL. His electrocardiography showed no abnormalities. The patient was treated with 2 g of calcium gluconate intravenously resulting in resolution of his symptoms. It was thought that the hypocalcemia was a side effect from the cinacalcet, so the medication was discontinued. However, 1 week later, he returned to the emergency department with similar complaints. At that time, his PTH was within normal limits at 32.8 pg/mL, while serum albumin-corrected calcium and ionized calcium remained low (Figure 1). At that point, 1000 mg of calcium carbonate twice daily was initiated, and vitamin D3 was increased to 2000 units daily while he remained off cinacalcet.
Within 6 months from starting the calcium supplements, his calcium levels improved and PTH level was within normal limits (Figure 1). At that time, he had abdominal computed tomography for evaluation of new-onset right flank pain, which demonstrated presence of a 3-mm kidney stone in the right ureterovesical junction. As his urinary calcium was inappropriately elevated (Table 1), we reduced calcium dose to 1000 mg daily. He was subsequently referred to nephrology clinic for further evaluation of his nephrolithiasis. There he was found to still have high-normal urinary calcium; hence, his supplemental calcium was further reduced and then discontinued resulting in normalization of urinary calcium excretion (Table 1) without altering eucalcemic state (Figure 1). Based on the renal stone risk urine panel evaluation, he was also advised to reduce dietary intake of oxalate, sodium, and purines. Since these changes were implemented, he had no further evidence demonstrating kidney stone formation including negative findings on the computed tomography of the abdomen in June 2019. A follow-up evaluation of BMD trends performed on the same densitometer in 2017 and 2018 showed stability or improvement in cortical bone BMD over time since cinacalcet was discontinued (Table 1). As of April 2020, more than 3 years since cinacalcet was discontinued and 10 months since calcium supplementation was stopped, he remains clinically and biochemically eucalcemic.
Discussion
Cinacalcet-induced hypocalcemia is rare in clinical practice. 9 The Evaluation of Cinacalcet Hydrochloride Therapy to Lower Cardiovascular Events (EVOLVE) trial evaluated the use of cinacalcet in patients being treated for secondary hyperparathyroidism on hemodialysis. This study found severe hypocalcemia (less than 7.5 mg/dL) to be most associated with having higher baseline PTH, lower serum calcium, higher serum alkaline phosphatase, and higher body mass index. Indeed, prior case reports clearly demonstrated that hypocalcemia can be indeed a significant concern when hyperparathyroidism in dialysis patients is treated with cincalcet.6,8 Yet, there is paucity of published data including registration trials that would identify a risk of severe hypocalcemia following initiation of the medication in patients with PHPT.
Our case presents several unique findings. First, cinacalcet-induced hypocalcemia occurred in a patient with normal kidney function. Second, the hypocalcemia our patient developed on cinacalcet was PTH-mediated as PTH level at the time of calcium nadir was very low, suggesting direct effect of the medication on parathyroid glands. We suggest that patient’s normalization of PTH may have been due to an apoptosis of remaining parathyroid adenoma cells from cinacalcet. In our case, having 3 parathyroid glands surgically removed could have compromised patient’s response to cinacalcet-associated hypocalcemia as we hypothesize that the activity of the dominant parathyroid gland responsible for PHPT in the patient was abolished by cinacalcet due to its apoplexy or necrosis. On the other hand, the fact that we were able to wean the patient off the calcium supplementation without use of active vitamin D analogs after 2.5 years from the episode of hypocalcemia suggests that the patient may have initially had dormant fifth parathyroid gland that became functionally active once the activity of 4 parathyroid glands has ceased due to surgical excision and cinacalcet exposure. In a previous case report, Di Dalmazi et al 10 described an 80-year-old patient with PHPT treated with cinacalcet for 17 months at a maximum dose of 180 mg daily who developed severe and symptomatic hypocalcemia that was associated with the resolution large parathyroid adenoma. In contrast, our patient has been receiving only a very small dose of cinacalcet for a short period of time and did not have clear radiographic evidence of parathyroid adenoma(s). Finally, our patient has experienced resolution of PHPT after short-term exposure to cinacalcet. This conclusion is supported by normal calcium and PTH levels without calcium supplementation for the last 9 months. There was also progressive improvement of DXA findings since cinacalcet was started and then discontinued in spite of unchanged background testosterone replacement therapy and vitamin D level suggesting resolution of hyperparathyroidism. Last, the degree of hypercalciuria has markedly improved, and as of the most recent measurement, his calcium content in urine was within normal limits.
Conclusion
We report a PHPT patient with normal kidney function who has experienced resolution of the disease following 6-month exposure to low dose of cinacalcet. We recommend that in PHPT patients who remain hypercalcemic after unsuccessful PTx to consider initiating lower doses of cinacalcet with close clinical and biochemical follow-up to monitor for the development of hypocalcemia.
Footnotes
Acknowledgements
This material is the result of work supported with resources and the use of facilities at the Stratton VAMC, Albany, New York.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EOG and ARG are employees of the US Department of Veterans Affairs and their opinions expressed in this article are those of the authors’ and do not represent the views of the Department of Veterans Affairs or the US government.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.