
Abstract
A 68-year-old man with end-stage renal disease was hospitalized because of radicular pain and weakness in the left arm and hand. Sonography and computed tomography had recently shown a large right renal mass. On admission, magnetic resonance imaging demonstrated vertebral metastases with epidural extension, and radiotherapy was directed to the spine and kidney. Hypocalcemia was first noted on the fourth hospital day. A second computed tomography scan showed bleeding into and around the kidney, and arterial embolization was required to halt the bleeding. Hypocalcemia persisted for at least 27 days at values between 6.0 and 7.7 mg/dL and was consistently associated with ionized calcium concentrations less than or equal to 4.44 mg/dL. After an unrevealing search for a recognized cause, we attributed hypocalcemia to persistent sequestration of calcium in the right retroperitoneum. Exogenous supplementation eventually restored the concentration to normal. In the absence of renal and intestinal loss, hypocalcemia reflects abnormal flux of calcium from the extracellular compartment into tissue. Our patient’s repository appears to have been a necrotic and hemorrhagic cancer. Tumor-induced sequestration of calcium should be included in the differential diagnosis of hypocalcemia.
Introduction
In hemodialysis patients, hypocalcemia has been reported as a complication of extreme hyperphosphatemia, low dialysate calcium, abrupt reduction in the parathyroid hormone concentration ([PTH]), antiresporptive therapy with denosumab, and iron chelation with deferasirox.1-6 This report describes a patient with transient hypocalcemia that could not be attributed to recognized causes. We ultimately concluded that a necrotic renal cancer had provided a temporary repository for extracellular calcium.
Case Report
A 68-year-old man was hospitalized because of radicular left arm pain of 2 weeks duration. Over the previous 14 weeks, the hemoglobin concentration ([hgb]) had fallen from 9.6 g/dL to values as low as 6.6 g/dL; 2 units of red blood cells (RBCs) had been transfused 4 weeks prior to admission. The patient, who was anuric, had experienced a single episode of gross hematuria almost 2 months before admission, but investigation of this complaint had been delayed. Nine days before admission, a renal sonogram had shown an atrophic left kidney and a large complex mass replacing the right kidney.
The patient had hypertensive renal disease and had undergone thrice-weekly hemodialysis for 2¾ years. Paget’s disease had been diagnosed approximately 17 years prior to admission; 8 years before admission a bone scan had shown increased activity in the pelvis, thoracic spine, and right humerus. The serum alkaline phosphatase concentration ([AP]s) had subsequently varied between 400 and 1000 units/L. [PTH] had been consistently elevated during the patient’s tenure on dialysis. Excellent control of phosphatemia ([P]s) had been achieved with 2 intestinal phosphate binders.
Medicines on admission included calcium acetate 1334 mg and lanthanum carbonate 1000 mg 3 times daily with meals; a multivitamin once daily; folic acid 1 mg daily; metoprolol tartrate 50 mg 3 times daily on nondialysis days; a nutritional supplement 3 times daily; simvastatin 40 mg at bedtime; sodium bicarbonate 650 mg 3 times daily; and ergocalciferol 50 000 units weekly. Cinacalcet had never been prescribed. During each dialysis treatment the patient received heparin, 3000 units at the outset and 1000 units/hour; paricalcitol 5 µg; and sodium ferric gluconate 62.5 mg. He also received darbepoietin 200 µg weekly.
Vital signs on admission were temperature 98.7°F, pulse 86/minute, blood pressure 187/89 mm Hg, and respiratory rate 16/minute. Skin, lymph nodes, lungs, and heart were normal. No masses or organomegaly were detected in the abdomen. Grip strength, wrist dorsiflexion, and elbow extension were weak in the left upper extremity, and pinprick sensation was reduced in the left fifth finger. Leg strength was normal; lower extremity reflexes were not hyperactive, and Babinski reflexes and clonus were absent. The patient was not incontinent.
Results of a technetium medronate bone scan performed 6 days before admission were compared to findings reported 8 years earlier. Previously described areas of increased activity were present in the right humerus, the sacrum, and the thoracic spine. An area of high uptake in the vertex of the skull had not been evident in the earlier study (Figure 1).

Technetium99 medronate bone scan.
On the day prior to admission, computed tomography (CT) of the abdomen confirmed the presence of a large, mixed-density mass in the right kidney (Figure 2a). Cortical thickening and increased trabeculation in multiple ribs, thoracic and lumbar vertebrae, the pelvis, and the left femur were suggestive of Paget’s disease (Figure 2c). Bone lysis and cortical breakthrough in T11 and T12 were attributed to malignancy (Figure 2d). Adenopathy was not seen.

Computed tomography of the abdomen.
On the day of admission, magnetic resonance imaging of the spine showed an expansile mass involving C7 and T1 with cortical breakthrough, epidural extension, and effacement of the left C7-T1 neural foramen. Cord compression was not evident. At T12, another expansile lesion involved the posterior vertebral body and the right pedicle and extended into the right anterior spinal canal. Widespread marrow signal changes and numerous focal lesions were suggestive of extensive vertebral metastases (Figure 3).

Magnetic resonance imaging of the cervical and thoracic spine.
After administration of 10 mg intravenously, dexamethasone was prescribed at an oral dose of 4 mg every 6 hours in anticipation of radiotherapy, which was begun on the second hospital day. In total, 32 Gy was delivered over 10 treatments to the metastasis at C7-T1, and 30 Gy to the metastasis at T12 and the renal mass.
On admission, [hgb] was 6.2 g/dL. Three units of packed RBCs were administered on the third and fourth hospital days, but [hgb] fell to a nadir of 5.6 g/dL. A second computed tomography scan confirmed the presence of blood within, anterior to, and posterior to the mass (Figure 2b), and the patient was referred for right renal arterial embolization. Three additional units of RBCs were infused over the ensuing 2 days, and administration of heparin during dialysis was discontinued. Transfusions were then withheld for 25 consecutive days.
Table 1 shows temporal relationships between laboratory data and therapeutic efforts during a 30-day period commencing on day 1. Figure 4 depicts serum concentrations of total calcium ([Ca]s), ionized calcium ([Ca]i), phosphorus ([P]s), and albumin ([alb]s), and the blood concentration of hemoglobin ([hgb]) over a 60-day period commencing on the same day. Reference ranges are provided in the legend. On day 2, the first day of radiotherapy, [Ca]s, [alb]s, and [P]s, were 8.3 mg/dL, 2.4 g/dL, and 3.2 mg/dL, respectively. On day 4, [Ca]s was 7.1 mg/dL, and over the next 5 days it fell to 6.3 mg/dL, with a commensurate reduction in [Ca]i. Manifestations of hypocalcemia did not appear.
Overview of Hospitalization a .

Abbreviations: Ca, calcium; alb, albumin; Cai, ionized calcium; P, phosphorus; PTH, parathyroid hormone; 25D, 25-hydroxyvitamin D; 1,25D, 1,25-dihydroxyvitamin D3 (calcitriol); AP, alkaline phosphatase; hgb, hemoglobin; RBC, red blood cells; HD, hemodialysis treatment; RT, radiotherapy treatment. Doses and sites of RT are provided in the text.
Concentrations are in serum. Normal ranges are given in parentheses.
Enumerated from day of admission to hospital. Discharge was on day 17.
Given as calcium carbonate.
Daily administration continued after discharge.
Given as calcium gluconate.
Date of right renal arterial embolization.
Dialysis these days against [Ca] 6.0 mg/dL, and against 5.0 mg/dL on all other days. Dialysis continued on a thrice-weekly schedule after discharge.
Dose still in effect on day 60.
Dose expired on day 46.
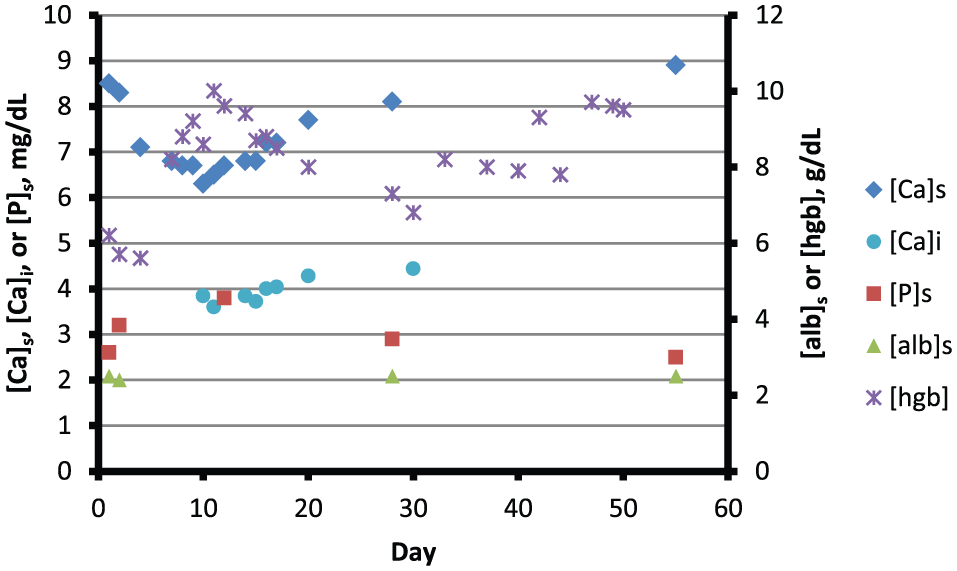
Blood hemoglobin and parameters of mineral metabolism over a 60-day period.
Calcium and ergocalciferol were not administered during the first 10 days of hospitalization, and cinacalcet was not provided at any time. Paricalcitol was not given during the periods summarized in Table 1 and Figure 4. Hemodialysis treatments were performed thrice weekly for 4 hours with Asahi Rexeed-18 high-flux polysulfone dialyzers. The dialysate calcium concentration was 5.0 mg/dL on all but 3 occasions; on days 15, 17, and 20 it was 6.0 mg/dL.
On day 11, 279 mg of calcium was infused as calcium gluconate; on day 12, an additional 186 mg was infused, and oral calcium carbonate was added with meals in a dose of 650 mg 3 times daily. Calcitriol, 0.25 µg/day, was prescribed on day 11 and increased to 0.25 µg twice daily on day 14. Introduction of these supplements was followed by a gradual rise in [Ca]i; the concentration was 4.04 mg/dL on day 17 (the date of discharge), 4.28 mg/d L on day 20, and 4.44 mg/dL on day 30. Thereafter, for a period of several months, [Ca]s exceeded 8.0 mg/dL while [alb]s remained at or slightly below 3.0 g/dL (Figure 5).

Parameters of mineral metabolism over a 600-day period.
Tests to investigate the cause of hypocalcemia were performed between the 3rd and 17th hospital days (Table 2). Serum concentrations of magnesium ([Mg]s), phosphorus ([P]s), urate ([ur]s), and 25-hydroxyvitamin D ([25OHD]) were normal, and concentrations of parathyroid hormone ([PTH]) and N-telopeptide ([NTx]) were markedly elevated. [AP]s was minimally increased. Reference ranges and conditions sought are summarized in Table 2.
Laboratory Investigations to Determine the Cause of Hypocalcemia a .

Abbreviations: P, phosphorus; ur, urate; Mg, magnesium; 25OHD, 25-hydroxyvitamin D; PTH, parathyroid hormone; AP, alkaline phosphatase; NTx, N-telopeptide; BCE, bone collagen equivalents.
All determinations in serum.
Figure 5 provides a 600-day temporal perspective. Over approximately 400 days prior to admission, [PTH] was consistently elevated despite normal [P]s and administration of parenteral paricalcitol during dialysis treatments. [25OHD] was robustly normal in response to supplemental ergocalciferol. [Alb]s remained between 3.0 and 3.5 g/dL, but it fell to a nadir of 2.4 g/dL during the period of hypocalcemia. [AP]s was consistently increased until 5 months before admission, but all subsequent values approximated or slightly exceeded the upper limit of normal.
The clinical suspicion of metastatic cancer was not confirmed histologically. An earlier iliac crest biopsy had shown no malignant cells, and risks associated with a renal or vertebral biopsy seemed prohibitive. Sunitinib was administered after completion of radiotherapy, but pulmonary and other metastases continued to appear and expand. The patient died in December 2012. An autopsy was not performed.
Discussion
This report describes a transient episode of hypocalcemia in a hemodialysis patient presumed to have renal cell cancer and metastases to bone. Measurements of [Ca]i repeatedly confirmed the hypocalcemia. The abnormality appeared after initiation of radiotherapy to the spine and right kidney and persisted for at least 27 days. It responded minimally to intravenous calcium during days 11 and 12, and gradually but incompletely to dialysis and oral calcium and calcitriol during days 12 to 30. The time required to restore normocalcemia was less than 60 days but is not precisely known.
During the first 10 days of hospitalization, we presume that omission of calcium acetate and paricalcitol from the medical regimen reduced intestinal calcium absorption. Simultaneously, however, we suspect that acquisition of calcium during dialysis equaled or exceeded this reduction. Values of [Ca]i on days 10 and 11 imply that dialysate-to-plasma [Ca] gradients had exceeded 1.0 mg/dL during the preceding week. On average, during a 4-hour dialysis treatment, such gradients should have promoted diffusion of at least 400 mg of calcium into plasma as 140 mg was removed by convection, with a net gain to the patient of 260 mg per treatment. 7 Because the patient had no diarrhea and produced no urine, it is unlikely that calcium was lost externally at a comparable rate if it was lost at all. During the period when [Ca]s was stable at its nadir, we infer that calcium accumulated in tissue at the rate of net influx.
On days 11 and 12, intravenous infusion of 465 mg of calcium had a negligible effect on [Ca]i. Between days 12 and 30, dialysis against physiologic or higher [Ca] and supplementation with calcium and calcitriol raised [Ca]i gradually but failed to correct it (Table 1). During days 1 to 30, we estimate that at least 2000 mg of exogenous calcium accumulated in a tissue reservoir.
We sought other causes of hypocalcemia. The patient presented no clinical evidence of pancreatitis or myonecrosis.8,9 Chelation by citrate could have reduced [Ca]i during RBC transfusions; 10 whereas [Ca]s typically remains normal during this process, 11 [Ca]s and [Ca]i fell in tandem in our patient (Figure 4), and hypocalcemia persisted for many days in the absence of transfusions.
We considered the possibility that dexamethasone had caused hypocalcemia. Steroids have lowered [Ca]s by causing pancreatitis or tumor lysis,12,13 or by interfering with intestinal calcium absorption in patients with hypoparathyroidism or vitamin D deficiency.14,15 However, under ordinary circumstances, exogenous steroids inhibit bone formation while resorption continues unabated, and the skeleton incurs a net loss of calcium. 16 We conclude that dexamethasone did not reduce [Ca]s in our patient.
Although chemotherapy had not been administered when hypocalcemia appeared, we wondered whether tumor lysis due to radiotherapy had lowered [Ca]s. We measured [P]s and [ur]s to investigate this possibility, 17 but neither was elevated. Hypomagnesemia may limit secretion of and end-organ responsiveness to PTH,18,19 but [Mg]s was also normal.
We considered the possibility that the skeleton had become an acutely receptive repository for calcium. In both Paget’s disease and secondary hyperparathyroidism (SHPT), rapid turnover of bone may produce an excess of unmineralized osteoid.20,21 We therefore contemplated a scenario, similar to the post-parathyroidectomy hungry-bone syndrome, 22 in which calcium flux from the skeleton had fallen while mineralization of osteoid continued unabated. We speculated that radiation-induced damage to bone or to the parathyroid glands had created the hypothetical disequilibrium.
Test results did not support this speculation. Although the concentration of alkaline phosphatase, a marker of bone formation, had been 714 units/L 5 months prior to admission, it was only 195 units/L on hospital day 2, and it fell further during the ensuing month (Table 1; Figure 2). In contrast, the concentration of N-telopeptide, a marker of bone resporption, was found to be markedly increased (Table 2), and [PTH] remained elevated despite radiotherapy to C7 and T1. The limited fields of radiation and the implied discrepancy between resorption and formation suggest that the skeleton was an unlikely repository for calcium. Although pharmacotherapy of SHPT or Paget’s disease may lower [Ca]s,3,23 we can find no evidence that radiation of affected bone has produced this result. We presume that lytic metastases caused net calcium flux into plasma.
Clinical and laboratory findings suggest that hypocalcemia did not result from drug toxicity, myonecrosis, pancreatitis, hypoparathyroidism, vitamin D deficiency, hypomagnesemia, tumor lysis syndrome, or hungry-bone syndrome. Because dialysate calcium levels were physiologic or higher, the only potential avenues of calcium loss from extracellular fluid were intestinal secretion and tissue deposition. We do not believe that muscle, pancreas, or bone served as a repository.
Our patient’s [Ca]s had remained consistently normal before admission. Hypocalcemia was detected 2 days after the initiation of radiotherapy, which appeared to exacerbate necrosis of and hemorrhage into a renal cancer. Arterial embolization probably amplified the necrosis. [Ca]i rose minimally with an intravenous infusion of calcium during days 11 and 12; through day 30, [Ca]i responded gradually but incompletely to influx of hundreds of milligrams of calcium from oral supplements and dialysate. We propose that a large collection of tissue and blood provided a reservoir for extracellular calcium; [Ca]s fell to a level at which influx from all sources could compensate for efflux into the right retroperitoneum, and returned to normal when the reservoir could accept no more calcium. In extraordinary circumstances, it appears that extensive tumor necrosis and associated hemorrhage can cause hypocalcemia.
Footnotes
Acknowledgements
This work was supported with resources of and made possible by facilities at the Stratton Veterans Affairs Medical Center, Albany, New York. We thank Drs Yat H. Lau and Brian McCandless for comments concerning the patient’s radiation therapy and radionuclide bone scan. We also thank Dr Pooja Ghatalia, who contributed to the patient’s care as a medical student.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.