
Abstract
Platypnea orthodeoxia syndrome (POS) occurs when an upright position results in acute-onset hypoxemia and is relieved with recumbency. POS can be due to intracardiac shunting, intrapulmonary shunting, ventilation-perfusion mismatch, or a combination of these. We report a case of POS that developed 3 days post liver transplantation as a result of new-onset right to left shunting across a patent foramen ovale. Right heart catheterization revealed a posteriorly directed inferior vena cava likely due to altered inferior vena cava—right atrial junction anatomy as a result of liver transplantation. The patient underwent successful transcatheter patent foramen ovale closure with a 25-mm Gore Cardioform septal occluder device with immediate and sustained improvement in hypoxia.
Introduction
We describe an unusual case of acute-onset positional hypoxia due to intracardiac shunting immediately following liver transplantation.
Case Presentation
A 69-year-old man with hepatitis C cirrhosis and hepatocellular carcinoma underwent uncomplicated orthotopic liver transplantation. Additional history includes a moderately dilated ascending aorta measuring 4.8 cm. Three days posttransplant, shortly following extubation, he developed profound positional hypoxia. Vital signs remained normal with recumbency with a blood pressure of 120/60 mm Hg, heart rate of 60 beats/min, and oxygen saturation of 94%. In an upright position, however, he became tachycardic to 120 beats/min, tachypneic with respiratory rate of 24 breaths/min, hypertensive with blood pressure of 175/100 mm Hg, and hypoxic with desaturations to 80% while receiving 100% supplemental oxygen via a non-rebeathing facemask. Physical examination revealed no new murmurs, pulmonary rales, jugular venous distension, nor peripheral edema.
Initial testing demonstrated a normal chest X-ray and ventilation perfusion scan. Transthoracic echocardiography demonstrated normal biventricular size and function, normal cardiac valve anatomy and function, and normal pulmonary artery, right ventricular, and right atrial (RA) pressures. An agitated saline study revealed evidence of a mild right to left shunting in the supine position with profound right to left shunting in the upright position (Figure 1a and b; Videos 1 and 2 [available online]).
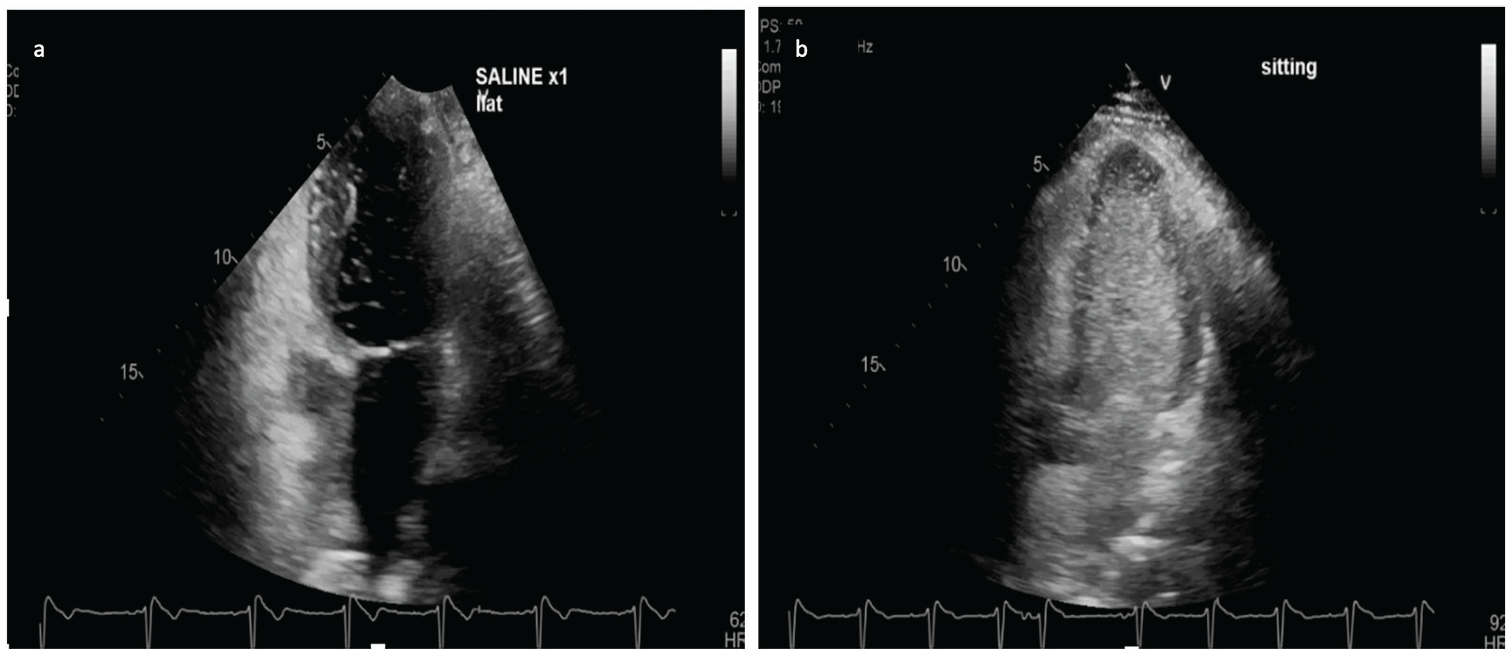
Transthoracic echocardiography following agitate saline infusion with patient supine (a) and upright (b) demonstrating the drastic increase in bubbles seen on the left-sided chambers when upright.
While echocardiography suggested shunting at the atrial level, the patient’s history of cirrhosis raised the possibility of intrapulmonary shunting. The patient was brought forward for a right heart catheterization performed through the right femoral vein demonstrating normal intracardiac pressures. The catheter course confirmed the presence of an interatrial communication although oximetry did not demonstrate a shunt while the patient was breathing spontaneously in the supine position (Table 1). Intracardiac echocardiography confirmed the presence of a patent foramen ovale (PFO) without evidence of a septal aneurysm, unusually long tunnel, or a prominent Eustacian valve. However, both the pressure catheter and intracardiac echocardiography catheter course were biased posteriorly and medially due to an acute angulation at the inferior vena cava (IVC)-RA junction.
Right Heart Catheterization Hemodynamics.

An agitated saline study performed within the high IVC demonstrated brisk shunting across the PFO. Additional agitated saline studies performed within the bilateral branch pulmonary arteries showed no evidence of intrapulmonary shunting. As such, a decision was made to proceed with transcatheter PFO closure, which was successfully performed using a 25-mm Gore Cardioform septal occluder device (Figure 2; Video 3 [available online]).

Intracardiac echo after atrial septal occluder device implantation.
Postintervention, the patient experienced immediate improvement in oxygen saturations and maintained oxygen saturations of 95%, in absence of supplement oxygen, in both the supine and upright positions. The patient was discharged on postoperative day 12 in excellent condition. One month follow-up transthoracic echocardiography confirmed complete occlusion of the interatrial shunt.
Discussion
Platypnea orthodeoxia syndrome is defined by acute-onset hypoxemia in an upright position, which is relieved with recumbency. It requires 2 factors be present, an anatomic component providing a passage for shunting and a functional component influencing the path of bloodflow. 1 Causes of POS include interatrial shunting, intrapulmonary shunting, and ventilation perfusion mismatch. 2 Interatrial right to left shunting may be due to increased RA pressures in the presence of an atrial septal defect or PFO. However, in select cases interatrial right to left shunting is observed in the absence of a right to left interatrial pressure gradient. It is generally accepted that shunting in the absence of a pressure gradient occurs as a result of flow dynamics such that venous return through the cavae are directed toward the interatrial septum resulting in right to left shunting through a preexisting communication. The sudden development of right to left shunting in the presence of a long-standing interatrial communication is less well understood, but in many cases, it is believed to be the result of atrial septal deviation as a result of aortic enlargement, kyphoscoliosis, or hemidiaphragmatic paralysis and augmented by positional changes.3,4
POS is a common sequela of advanced cirrhosis but largely as a result of intrapulmonary shunting due to hepatopulmonary syndrome, in which diffuse pulmonary arteriovenous malformations (AVMs) develop as a result of synthetic dysfunction. Hepatopulmonary syndrome leads to the POS due to preferential blood flow to the lower lung fields, where AVMs predominate, in an upright position. 4 POS immediately post liver transplantation is a well-described phenomenon due to persistence of diffuse pulmonary AVMs for many months posttransplantation and treatment centers on supportive care of this self-limiting pathology. 5
To the best of our knowledge, POS post liver transplantation as a result of acute right to left shunting across a PFO in the absence of cardiac pathology has never been reported. It stands to reason that our patient had a previously unknown PFO, which was of no clinical significance prior to liver transplantation. It is our belief that during liver transplantation the IVC was manipulated in such a way as to alter the path of blood flow across the IVC-RA junction toward the PFO resulting in POS. The marked posteromedial deviation of the catheter across the IVC-RA junction during the right heart catheterization supports this theory.
Conclusion
This case highlights the importance of a multidisciplinary approach to acute-onset hypoxia in patients undergoing surgical procedures that may result in altered orientation of either the IVC or intracardiac septum. The presence of POS as a result of an interatrial communication should prompt strong consideration for transcatheter occlusion, a safe and effective treatment strategy. 6
Footnotes
Authors’ Note
This case was presented as an abstract at the American College of Cardiology virtual meeting, March 2020.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Steinberg is a consultant for Medtronic. Dr Larson and Dr Vutien have no disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.