
Abstract
Immunoglobulin A vasculitis (IgAV), formerly known as Henoch-Schönlein purpura, is an immune-mediated small vessel vasculitis characterized by palpable purpura, arthralgia, abdominal pain, and renal disease. It is primarily a childhood disease and usually resolves spontaneously with supportive therapy. Treatment of IgAV in adults is controversial with no clearly established guidelines. We report a rare case of IgAV in an adult male who developed gut necrosis and perforation while receiving glucocorticoid therapy for treatment of acute glomerulonephritis. A 44-year-old male was admitted with joint pain, leg swelling, mild abdominal pain, and a diffuse rash. Laboratory values revealed acute kidney injury with significant proteinuria and hematuria. The patient was started on glucocorticoid therapy for suspected IgAV nephritis, which was confirmed by kidney biopsy. Several days later, he complained of worsening abdominal pain. Imaging demonstrated bowel ischemia and perforation requiring multiple abdominal surgeries. The patient was critically ill in the intensive care unit with worsening renal failure requiring dialysis. He was discharged a month later after gradual recovery with stable but moderately impaired kidney function. IgAV is less common in adults; however, the disease is more severe with a higher risk of long-term complications. Adult patients with renal involvement may benefit from glucocorticoid therapy in preventing progression to end-stage renal disease. However, glucocorticoids may mask the symptoms of abdominal complications like gut necrosis and perforation causing delay in diagnosis and treatment. Therefore, vigilance to detect early signs of gut ischemia is imperative when treating an adult case of IgAV nephritis with glucocorticoids.
Keywords
Background
Immunoglobulin A vasculitis (IgAV), previously referred to as Henoch-Schönlein purpura, is the most common systemic vasculitis in children. It is a small vessel vasculitis that can affect the joints, kidneys, skin, and the gastrointestinal tract. IgAV is chiefly a childhood disease with an annual incidence of about 20 per 100 000.1,2 It is much less common in adults with a reported annual incidence of 2 to 5 per 100 000.3,4
IgAV is characterized by a tetrad of clinical manifestations that includes palpable purpura, arthralgia, renal disease, and abdominal pain. 5 Diagnosis is confirmed by performing a biopsy demonstrating deposition of IgA in affected organs.
IgAV is generally self-limited and the majority of patients recover spontaneously. An exception is adults with renal disease, who have a much higher incidence of severe renal failure and progression to end-stage renal disease (ESRD).6-8 For the majority of patients, treatment is generally supportive including bed rest, hydration, and pain control with nonsteroidal anti-inflammatory drugs. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are indicated for proteinuria >0.3 g/day.
The role of glucocorticoids in IgAV treatment is controversial. Studies have shown glucocorticoid therapy shortens the duration of abdominal pain and reduces the risk of developing persistent renal disease. 9 There is a paucity of high-quality data from randomized clinical trials on the management of IgAV in adults. Adults with IgAV and renal disease are frequently treated with systemic immunosuppression.3,10 There is evidence suggesting benefit of aggressive glucocorticoid therapy for adult-onset IgAV in preventing severe renal disease and ESRD. 11 Predictors for persistent renal disease are elevated creatinine, proteinuria >1 g/day, and nephrotic syndrome. The caveat in using glucocorticoids is that these medications may mask the symptoms and signs of gut ischemia associated with IgAV. 12
Case Presentation
The patient is a 44-year-old African American male, with a history of diabetes and hypertension, who presented to the emergency department on December 30, 2018, with complaints of joint pain, leg swelling, mild abdominal pain, and a rash. His symptoms began 5 days before admission with lower extremity arthralgia and swelling. The pain progressed and a diffuse rash appeared over his back, legs, and abdomen. Physical examination was notable for palpable purpuric lesions distributed extensively across the lower extremities, abdomen, and back (Figure 1A-D). Laboratory studies were significant for acute kidney injury (AKI) with a serum creatinine of 1.4 mg/dL, hematuria and proteinuria >1 g/day. His baseline creatinine was 1 mg/dL 3 months ago.

Palpable purpura with convalescence and necrosis on (A) bilateral palmar hands, (B) bilateral dorsal hands, (C) bilateral lower extremities, and (D) chest and abdomen. There is edema and inflammation as well as extravasation of blood from damaged blood vessels in association with immunoglobulin A vasculitis (Henoch-Schönlein purpura).
Nephrology was consulted, and a clinical diagnosis of IgAV was made based on his symptoms, palpable purpura, and renal failure. The patient was admitted and started on intravenous hydration and an nonsteroidal anti-inflammatory drug (NSAID) for pain. On hospital day 2, his creatinine sharply increased to 2.4 mg/dL. Urinalysis revealed active sediment with hematuria and proteinuria. Acute glomerulonephritis from IgAV was suspected. The NSAID was stopped and changed to acetaminophen-hydrocodone. Glucocorticoid therapy was started with pulse dose intravenous methylprednisolone daily for 3 days followed by oral prednisone. Kidney biopsy was performed. Light microscopy demonstrated diffuse proliferative changes with endocapillary hypercellularity, infiltration of polymorphonuclear neutrophils within capillary loops, and segmental fibrinoid necrosis (Figure 2A, C). There were no cellular crescents, interstitial inflammation, fibrosis, or tubular atrophy. On immunofluorescence, there was granular staining of the glomeruli with IgA, C3, and Lambda light chains consistent with diffuse proliferative and exudative glomerulonephritis with IgA dominant immune complex deposits (Figure 2B).
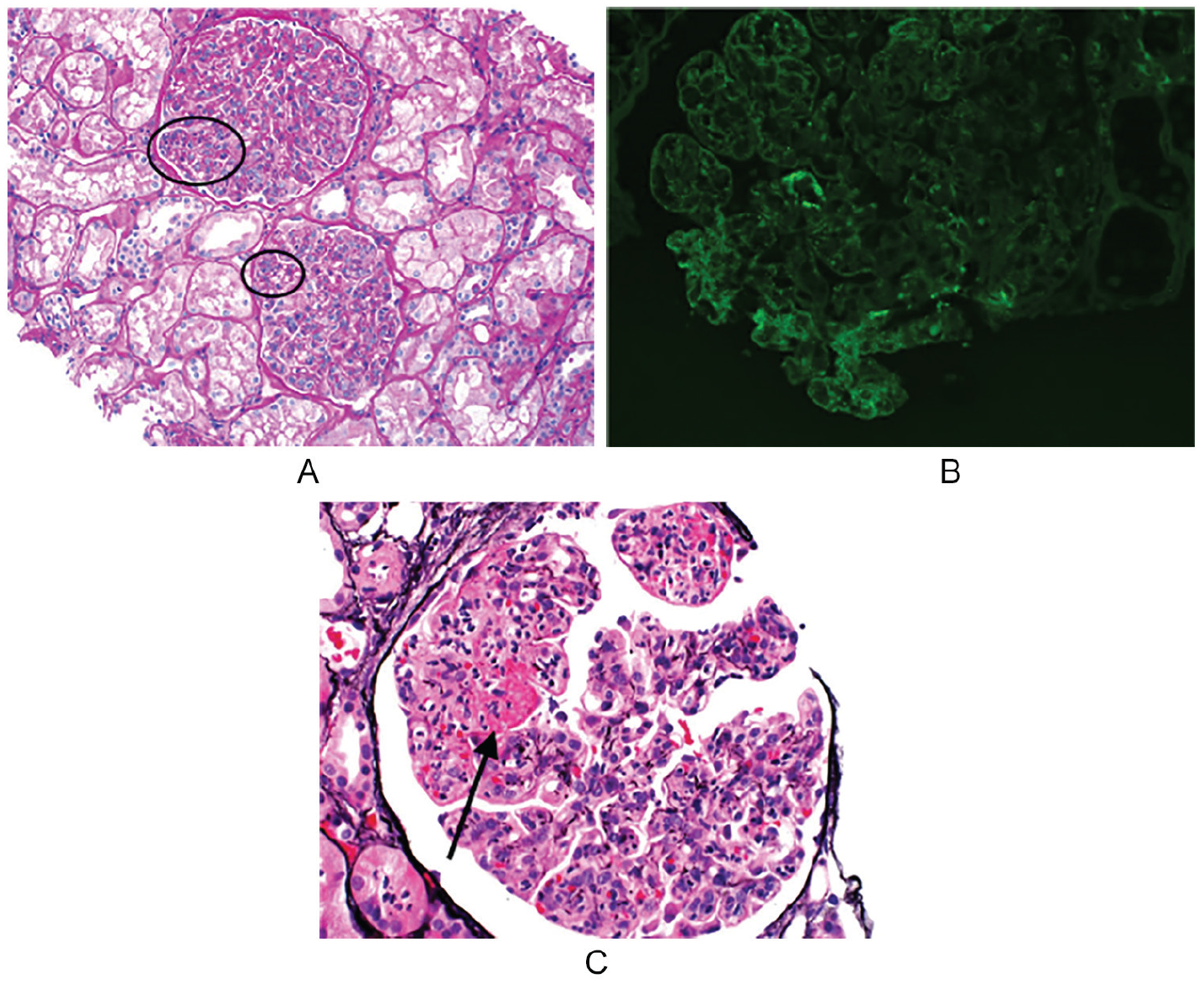
(A) Light microscopy with hematoxylin and eosin (H&E) stain highlights diffuse proliferative glomerulonephritis with inflammatory changes in glomeruli, including mesangial hypercellularity (ovals). (B) Direct immunofluorescence microscopy with staining shows granular IgA deposition in peripheral and mesangial capillary walls. (C) Light microscopy with H&E stain displays vessel wall fibrinoid necrosis (arrow) surrounded by focal capillary loop rupture.
Treatment with high-dose prednisone was continued. His serum creatinine decreased to 1.3 mg/dL. However, the purpuric rash became more widespread involving his mouth and throat, and the lesions on his legs grew larger. He continued to complain of abdominal pain. On hospital day 8, 6 days after starting glucocorticoid therapy, the abdominal pain worsened and was even more intense on hospital day 9. A computed tomography (CT) scan of the abdomen was performed and showed extensive pneumatosis of the gut wall consistent with bowel ischemia (Figure 3).

Axial view of CT scan of the abdomen pelvis displays extensive bowel pneumatosis (arrows).
He underwent urgent surgery that night. On laparotomy, he was found to have a perforation in the duodenum along with ischemic necrosis of 6 feet of the jejunum and the entire ascending colon. The necrosed jejunum and ascending colon were resected and a vacuum-assisted closure of the wound was placed. After the surgery, the patient was critically ill in the intensive care unit with hypotension requiring high-dose vasopressors including vasopressin and norepinephrine. His urine output dropped significantly, creatinine increased to 4.5 mg/dL, and his serum potassium increased to 6.0 mg/dL. He was losing fluid from his abdominal wound. Continuous renal replacement therapy (CRRT) was started in the intensive care unit with a permcath. He underwent a repeat exploratory laparotomy that revealed contamination but no evidence of ischemia or leak. The colon looked viable. On hospital day 12, the patient had another exploratory laparotomy and a small bowel anastomosis with ileostomy. The surgical wound had delayed closure despite wound care and vacuum-assisted closure of the wound. The wound was large and widely open involving the entire thickness of the muscles of the anterior abdominal wall (Figure 4).

On postoperative day 6, the open abdominal wound measures 20 cm × 15 cm × 10 cm in the left lower quadrant. The opening of the wound is oval, dusky, and oozing. There are ulcerations in the surrounding skin.
His condition was further complicated by gastrointestinal bleeding requiring embolization of the bleeding vessel by interventional radiology. He developed bilateral deep vein thromboses and underwent placement of an inferior vena cava filter. He had a prolonged course on mechanical ventilation and was switched from CRRT to every other day hemodialysis. Over the next few weeks, his condition slowly improved and his urine output gradually increased.
He was extubated on hospital day 22 and was eventually discharged after a 6-week hospital stay complicated by multiple surgeries, infections, delayed wound healing, and cytopenia. During the admission, he received multiple units of blood products including 19 packed red blood cell transfusions, 2 platelet transfusions, 3 fresh frozen plasma transfusions, and 1 cryoprecipitate. His kidney function slowly improved, and he was taken off dialysis. On discharge, his serum creatinine was 1.42 mg/dL, and his blood urea nitrogen was 28 mg/dL. An appointment was made for him to follow-up with nephrology.
Conclusion
IgAV in adults tends to be a more severe disease than it is in children and carries an increased risk of progressive renal disease and ESRD. 13 Renal involvement, otherwise known as IgAV nephritis (IgAVN), is the most serious manifestation of IgAV since it is the only organ linked to long-term morbidity and mortality in both childhood-onset and adult-onset disease. 14 Adults with IgAV and IgAVN tend to have a worse prognosis and usually need more aggressive treatment with glucocorticoids and other cytotoxic drugs.13,15 Although there is no evidence that treatment of IgAV with glucocorticoids prevents renal disease or ESRD, glucocorticoids may be beneficial in preventing progression of renal disease and ESRD in patients with established IgAVN.
Pozzi et al showed the effectiveness of glucocorticoids in preventing ESRD in adults with IgA nephropathy. 16 Also, the efficacy of glucocorticoid therapy in the treatment of various other forms of immune complex-mediated glomerulonephritis is well established. 16 Data from a systematic review of 3 randomized trials and 12 retrospective studies showed glucocorticoids decreased risk of intussusception, renal involvement, and recurrence of disease. 9 Based on data obtained in adults with IgA nephropathy, Kidney Disease: Improving Global Outcomes 2012 guidelines recommend treatment of IgAVN with glucocorticoids. 17 Furthermore, the 2019 International Consensus Guidelines proposed treatment with glucocorticoids for renal disease in IgAV using the best available evidence. 18
Our patient had AKI on presentation and biopsy-proven IgAVN. This put him at an increased risk of worsening renal function and ESRD, which warranted aggressive treatment with glucocorticoids. Unfortunately, he developed bowel perforation from IgAV. The gastrointestinal signs may have been masked by prednisone, leading to delay in diagnosis. However, the significant recovery of renal function after sustaining severe IgAVN-related AKI, which ultimately required dialysis, may have been due to early initiation of glucocorticoid therapy. Our patient was successfully taken off dialysis and remains dialysis free to this day.
An important pitfall of treating IgAVN with glucocorticoids is that it can mask pain and other signs of bowel ischemia, a potentially life-threatening complication of IgAV. This case illustrates the importance of early recognition and screening for abdominal complications of IgAV in patients treated with high-dose glucocorticoids, while at the same time making judicial use of glucocorticoids to prevent long-term renal sequelae in adult onset IgAV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.