
Abstract
Aim:
This study aimed to evaluate the penetration depth and persistence of sealer residues in obturated canals with three different bioceramic sealers using confocal microscopy.
Materials and Methods:
In total, 60 single-rooted human premolars were selected and decoronated to maintain the working length of 14 mm. The samples were biomechanically prepared and obturated with Protaper Universal GP coated with three different bioceramic sealers, that is, CeraSeal RC, Bio-C and MTA Fillapex. The specimens were divided into three groups (n = 20) depending on the sealer used. Rhodamine B fluorescent dye was added to the sealers before using them for obturation. The obturated samples were sealed and placed in 100% humidity at 37oC for 7 days. Gutta-percha was removed from all the samples using retreatment files. Each sample was horizontally sectioned into 2 mm thick slices at 3 mm and 5 mm from the apex, which were analysed under a confocal scanning microscope to detect the depth of penetration of sealer into the dentinal tubules. Data were analysed using one-way ANOVA and Tukey’s post hoc tests.
Results:
Intergroup comparison of penetration depth at 3 mm showed that the mean depth of penetration among CeraSeal samples was found to be significantly more as compared to the other two materials, while, no statistically significant difference was found among Bio-C and MTA Fillapex with the significance level established at 5% (P < .05). Similarly, an intergroup comparison of penetration depth at 5 mm showed that the mean depth of penetration among CeraSeal samples was found to be significantly more as compared to the other two materials, while, no statistically significant difference was found among Bio-C and MTA Fillapex. CeraSeal RC sealer showed significantly higher depth of penetration than Bio-C and MTA Fillapex.
Conclusion:
All bioceramic sealers show a significant penetration into the dentinal tubules. However, none of the sealers was completely removed from the tubules following retreatment.
Introduction
A three-dimensional seal is the ultimate goal of any root canal obturation. 1 It prevents reinfection and promotes positive conditions for a sterile environment. 2 Various factors like proper instrumentation, biomechanical preparation and obturation are crucial for an ideal root canal treatment. 3 Keeping in mind the complex anatomy of the radicular pulp space, a good cleaning protocol is required to reduce the bacterial load. 4 The contemporary techniques used for cleaning and shaping along with three-dimensional obturation lead to outstanding treatment. 4 A fluid-tight seal of the pulp canal is established by the use of endodontic sealers along with an orally accepted core material. Numerous sealers are commercially available in dental practice. Based on their composition, sealers are categorized as zinc oxide eugenol sealers, calcium hydroxide sealers, silicon-based, glass-ionomer and bioceramic sealers. 5 The major role of any sealer is to block the apical foramen and accessory canals and also to bind the core material and the wall of the radicular dentin. 6 One of the main factors determining the selection of the canal sealer is its potential to infiltrate the tubule lumen, thus providing an adequate seal. The principal reason for endodontic failure is poor contact between gutta-percha and the endodontic sealer, and also between the sealer and the radicular dentin walls.7,8 In case a root canal failure occurs the principal treatment of choice would be a Nonsurgical retreatment. Retreatment includes a total removal of existing obturation to make the canal sterile and promote periapical healing by placing a suitable filling material. 9 Nonsurgical retreatment is considered successful only when all of the filling material is removed effortlessly and effectively. 10 Several methods have been advocated to eliminate the core material and sealer, such as heat pluggers, hand files, GP solvents, lasers and retreatment rotary files. 11
Bioceramic sealers came into practice due to their desirable properties of bioinert, bioactive or biodegradable in the oral environment. 12 These sealers have alkaline pH and chemical stability, which makes these materials more biocompatible than the rest of the materials available these days. 13 These sealers have suggested a mechanism of action of tubular dispersion of their particles into the lumen of the tubules that leads to mechanical engaging. 14 The tubular penetration of sealer depth can be evaluated in vitro as a method of assessing sealing ability. Various microscopic techniques are being used to evaluate the penetration depth, namely stereomicroscopy, transmission microscopy, scanning electron microscopy and confocal laser scanning microscopy. 15 Confocal laser scanning microscope (CLSM) gives more précised images about the existence of filling material in the dentin lumen at very low magnification by incorporating florescent Rhodamine-dye. 16
To the greatest extent of the authors’ knowledge, nonetheless, relatively few studies have assessed the bioceramic sealers’ tubular penetration in the retreated root canals. Three-dimensional cleaning of radicular space, to reduce bacterial population, can be quite challenging in the case of bioceramic sealers. The penetration and sealing of new material after retreatment can be hampered as residual particles of previous endodontic sealers or filling material are present at microscopic levels. This is due to the persistence of the bacterial population and infection. 17
The three bioceramic sealers have not been compared before in terms of remaining penetration depth after retreatment. Hence, the present ex vivo study evaluated the penetrability and prevalence of sealer residues in previously filled canals with three different bioceramic sealers using rhodamine B dye under confocal microscopy. This is the first attempt to undertake a confocal microscopy study for the assessment of residues of CeraSeal, Bio-C and MTA Fillapex in the radicular canal even after retreatment was performed. The null hypothesis considered that the bioceramic sealers used would not be entirely removed from the dentinal tubules after retreatment was performed.
Materials and Methods
Preparation of Specimen
The study plan for this in vitro experimental research was accepted by the Institutional Ethical Committee (REF:IES/2023/04). A non-probabilistic protocol of sample preparation was followed based on a correlated study published in the literature. 18 Freshly extracted 60 single-rooted premolars were selected. The teeth with curved roots, resorbed roots, fracture lines, caries and obliterated canals were not considered for the study. The samples were stored at room temperature in 0.9% sterile saline. The coronal part of the samples was decoronated with a diamond disc placed in a straight handpiece under water spray, to keep a specific root length of 14 mm. A 10 K file (Mani Inc., Tochigi, Japan) was used to maintain the apical patency.
A working length of 0.5 mm short of the apical foramen was established with a 10 K file. Canals were prepared with crown down techniques at a speed of 300 rpm and a torque-control level of 2, up to the working length (14 mm), using a 16:1 reduction handpiece and ProTaper Universal rotary file system (Dentsply Maillefer, Ballaigues, Switzerland) till the F3 instrument. Through irrigation was done in between each filling with 2 mL of 5.25% sodium hypochlorite using a passively placed 22 gauge needle into the canal without binding to the walls, keeping it 3 mm short of apex. A final rinse was culminated with 3mL of 17% EDTA for 3 min and 2 mL of 3% sodium hypochlorite over 3 minutes later treated with 3 mL of distilled water. The samples were then dehumidified with corresponding paper points and randomly categorized into three groups (n = 20) according to the Bioceramic sealer advocated for obturation.
Group I: CeraSeal (MetaBiomed, Korea)
Group II: Bio-C (Angelus, Londrina, Brazil)
Group III: MTA Fillapex (Angelus, Londrina, Brazil)
Obturation
Single cone technique using F3 gutta-percha (Dentsply Maillefer, Ballaigues, Switzerland) and three bioceramic sealers was used to perform root canal filling. The sealers were manoeuvred by the instructions provided by the manufacturer. 0.1% of rhodamine B fluorescent dye was incorporated into sealers before obturation. The endodontic sealer was placed in the pulp canal with Lentulo spiral. Obturation was done by F3 cones, which were covered by respective sealers mixed with rhodamine B dye. The coronal end was blocked by intermediate filling material (Cavit G, 3M ESPE, St. Paul, Minnesota, USA) and subjected to 100% moisture at 37oC for 1 week to ensure total hardening of sealers before testing.
Retreatment
The samples were subjected to root canal retreatment using retreatment rotary files (Waldent Innovations Pvt Ltd, New Delhi) at a speed of 350 rpm and a torque of 1.5NCm using X-Smart Endomotor (Dentsply Maillefer, Ballaigues, Switzerland). The files WR1 (30/09), WR2 (25/08) and WR3 (20/07) were employed to eliminate gutta-percha from coronal, middle and apical thirds respectively, according to manufacturers’ instructions. Irrigation was done in between each filling with 3% sodium hypochlorite.
Sectioning and Image Analysis
At the level of 3 mm and 5 mm from the root aperture, the specimens were sectioned horizontally using a diamond disc at a low speed using continuous water coolant. Thus, two specimens of 2 mm thickness each were procured from a single tooth. The sections were polished with abrasive sandpaper and later observed under laser scanning microscopy.
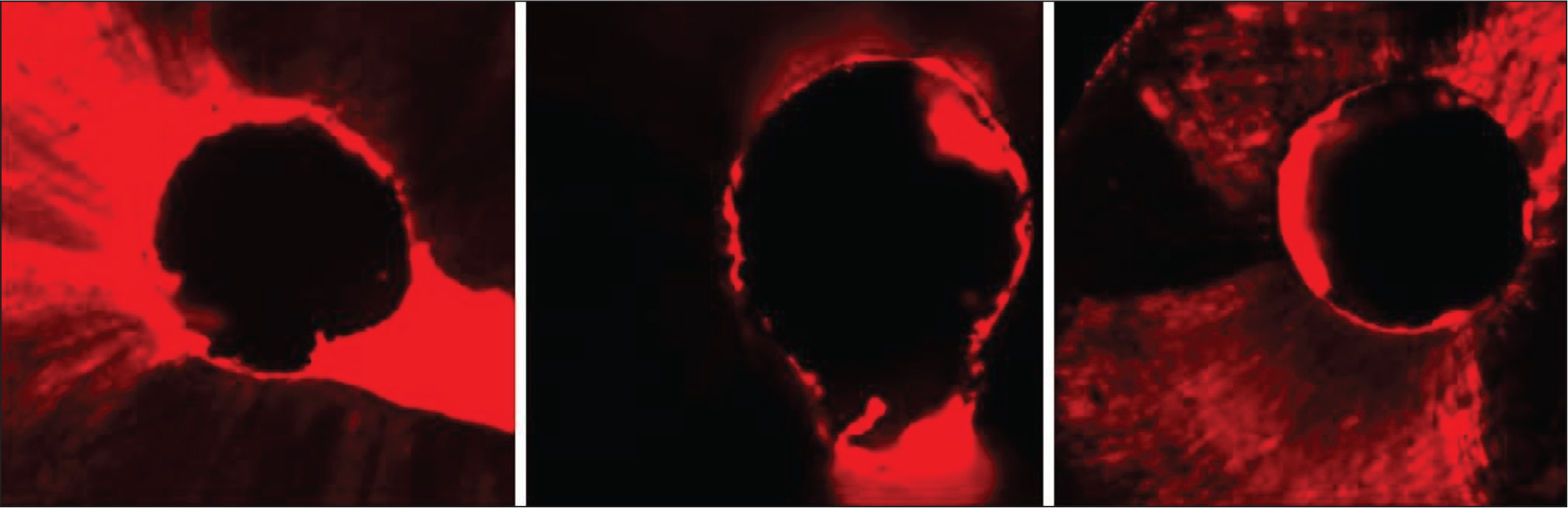
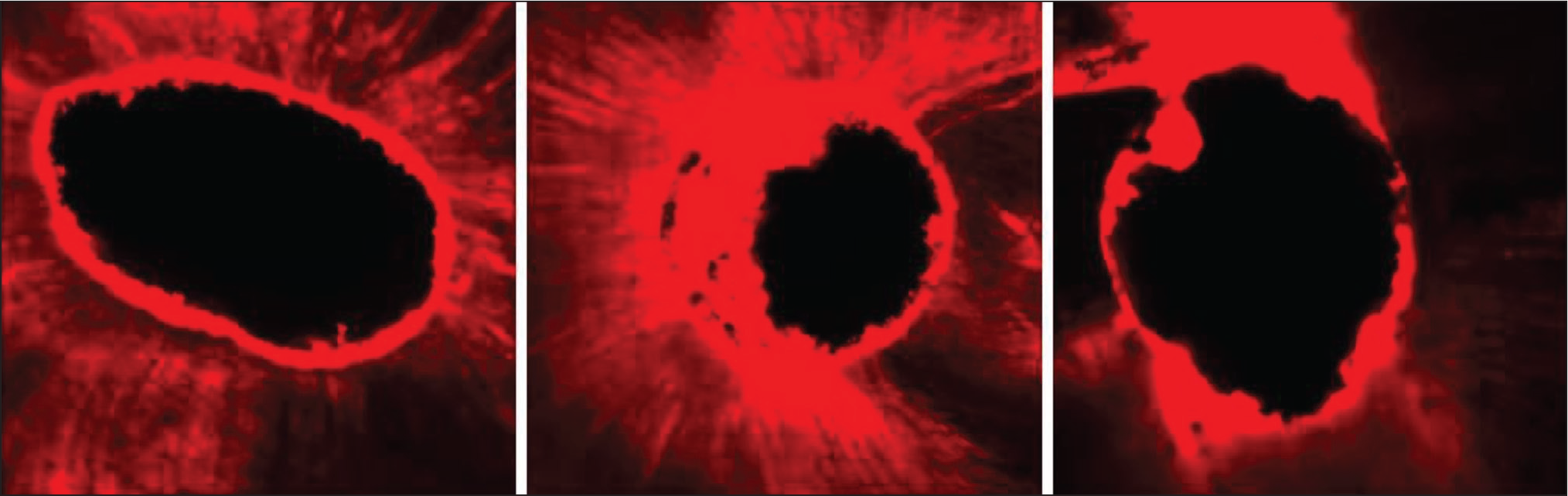
The sectioned specimens were arranged over glass slides and placed on the confocal microscope (Olympus Fluoview FV 1000) for examination. The maximum imbibing of the rhodamine B dye is 540 nm. The samples were examined using the 10 × lens. In total, 120 images were recorded correlating with the 60 samples at 3 mm and 5 mm, respectively. The digital images recorded were imported to ImageJ (National Institute of Health, Bethesda, MD, USA) program to measure the amount of sealer penetration into the dentinal tubules using an integrated ruler. The penetrability was recorded such that the starting point was determined from the canal wall and penetration of sealer into the lumen of the tubules was measured, up to a limit of 1,000 micrometres depth. An average was calculated for each sample to obtain a single reading (Figures 1 and 2).
Sealer Penetration (3 mm Level) of Ceraseal, Bio-C and MTA Fillapex Under 4 Confocal Scanning Electron Microscope.
Sealer Penetration (5 mm Level) of Ceraseal, Bio-C and MTA Fillapex Under 33 Confocal Scanning Electron Microscope.
Statistical Analysis
Three groups were examined by applying two-way ANOVA and post hoc multiple comparison tests at 3 and 5 millimetres from the apical end of the root canal using IBM SPSS Statistics Software (version 22.0, IBM SPSS Inc., Chicago, Illinois USA). A significant limit of P < .05 remains in effect.
Results
ANOVA was performed to analyse the sealer penetrability (μm) of each of the groups, and the outcomes were statistically significant.
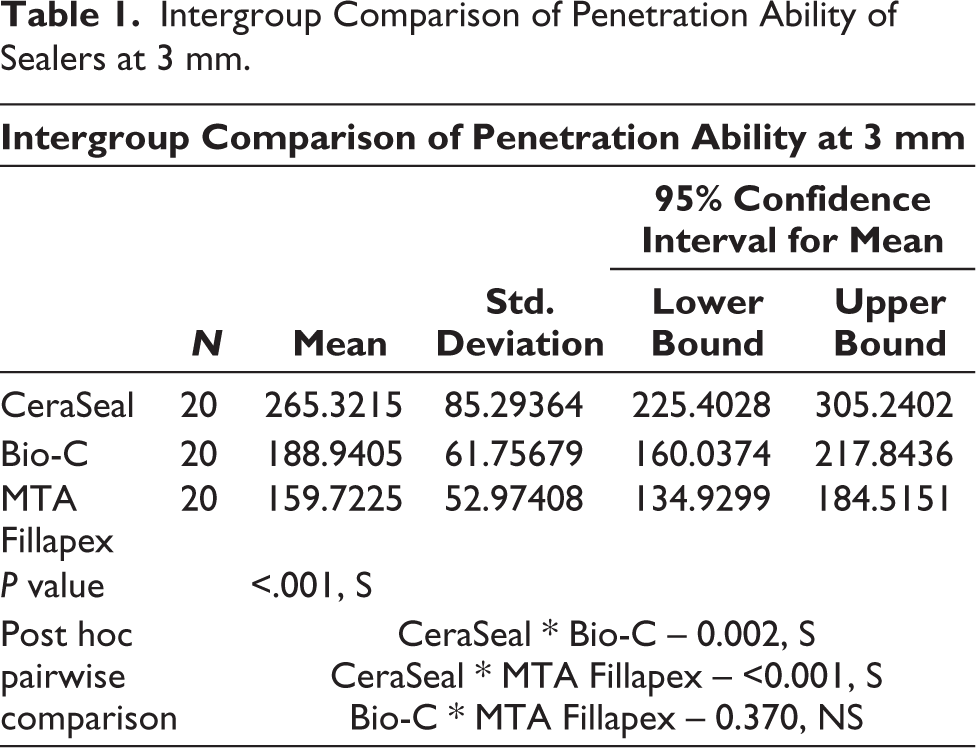
Intergroup comparison of penetration depth at 3 mm showed that the mean depth of penetration among CeraSeal samples was found to be significantly more, but there was no statistically significant difference between the other two materials, that is, Bio-C and MTA Fillapex (Table 1).
Intergroup Comparison of Penetration Ability of Sealers at 3 mm.
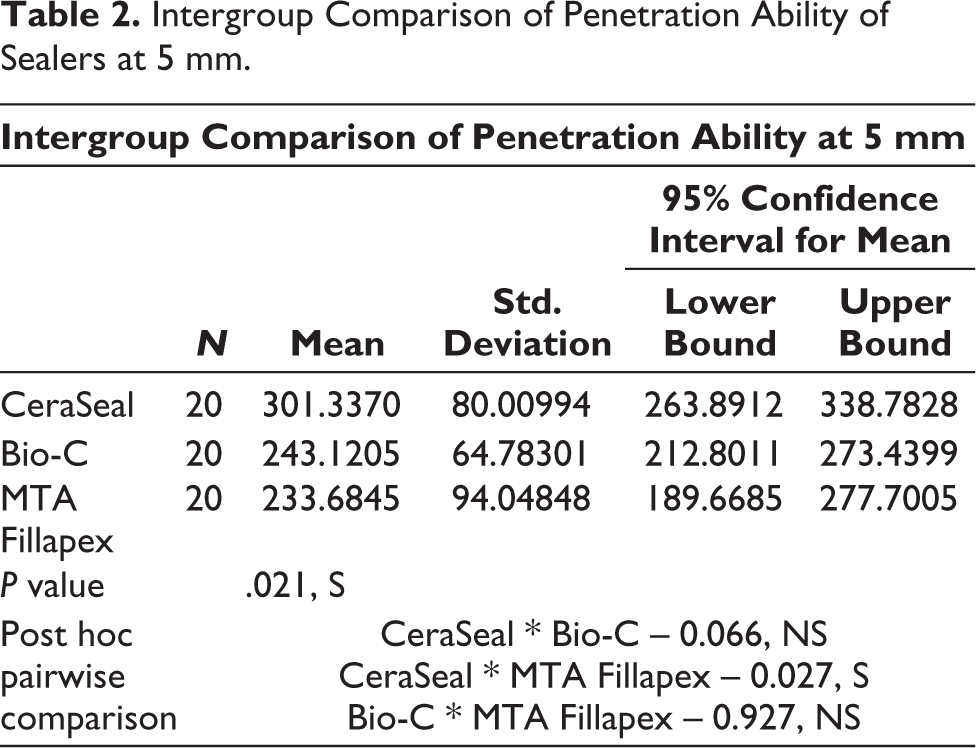
Similarly, an intergroup comparison of the penetration ability of sealer depth at 5 mm showed that the mean CeraSeal samples exhibited a substantially greater sealer penetrability when compared to the other two materials. Yet, no statistically significant difference was noticed comparing Bio-C and MTA Fillapex (Table 2).
Intergroup Comparison of Penetration Ability of Sealers at 5 mm.
An intragroup comparison of depth of penetration among CeraSeal samples showed that the mean depth of penetration did differ significantly at 3 mm and at 5 mm levels.
Bio-C samples on intragroup comparison showed that the mean depth of penetration at the 5 mm level was significantly more than that at the 3 mm level.
Intragroup comparison of depth of penetration among MTA Fillapex samples showed that the mean depth of penetration at the 5 mm level was significantly more.
Thus, the overall penetration of sealers was deeper at the level of 5 mm as compared to the level of 3 mm from the apical third of the root.
Discussion
The protocol of this research was devised to assess the remaining amount of sealer after the retreatment of specimens, which were previously filled with various new bioceramic endodontic sealers available. The retreatment procedure validated for the study aimed to completely eliminate the bioceramic sealer from the tubules. The use of rotary nickel-titanium files was considered the most efficient way to achieve it. These files are time-saving, cause less fatigue and also maintain the apical patency, 19 thus ProTaper Universal retreatment files were used. On the contrary, studies have shown that no retreatment systems cleaned the canal thoroughly. 19 Even with the use of solvent during retreatment procedure some amount of sealer residues are left on the dentin canal walls, which might be difficult to remove. 20
Any root canal treatment is said to be successful only if thorough cleaning, shaping and complete sealing of the radicular pulp space is achieved. Studies have shown that of all failures in root canal treatment, 58% are linked to defective obturation, thus total disinfection and three-dimensional obturation are needed. 21
To achieve a fluid-tight seal of the filling material and the root dentin, endodontic canal sealers are placed. These sealers penetrate deep into the tubular dentin, thus increasing the confluence between the core filling material and the radicular dentin. 22 This can be one of the major factors for the selection of the sealer for the root canal obturation. In addition, some researchers have revealed that the penetrability of sealers into the tubules of radicular dentin can prevent bacterial growth due to their antibacterial effect. 23
Recently many new types of sealers are being marketed. The Bioceramic sealers have superior biological as well as physio-chemical properties as compared to the traditional endodontic sealers. 24 The major advantages include that its biological properties are similar to hydroxyapatite, innate bone-healing capability, acts as a scaffold for regenerative activity and formation of chemical bonds with the tooth structure during obturation. 25 Studies have claimed that these sealers have small particle sizes, and thus show superior penetration depth than other sealers available. 13 Bioceramic sealers are categorized according to their composition, namely, calcium silicate-based, MTA-based and calcium phosphate-based. 26 The sealers used for investigation are CeraSeal, Bio-C and MTA-Fillapex bioceramic sealers.
CeraSeal is marketed in a syringe as a pre-mixed, ready-to-use sealer. It is a calcium silicate-based bioceramic sealer that sets in the presence of moisture-forming calcium hydrate gel and calcium silicate gel. CeraSeal has a 12.73 alkaline pH and 3.5 hours of setting time. 27 These sealers are said to form an excellent hermetic seal, thus preventing bacterial growth. Manufacturers also claim that odontoclastic activity is completely prevented due to their property being dimensionally stable. 28
Bio-C is a non-resin sealer that promotes tissue regeneration. It comes in a ready-to-use syringe formulation. The Bio-C sealers show excellent adhesion to dentin by the formation of a Mineral Infiltration Zone, which prevents bacterial infiltration. 29
Another sealer utilized in the investigation is a resin MTA-based sealer, which is made of nanosilicate particles, MTA Fillapex. 30 This sealer easily penetrates the lateral canal due to the property of elevated flow rate and decreased film thickness. The only drawback this type of sealer shows is the high cytotoxicity due to the resin component. 31
Removal of endodontic filling material is required in case of endodontic failure. Sometimes microbes can extend far into the tubule lumen of the radicular dentin up to 100–1000 μm, thus making it strenuous for the sealer to completely infiltrate the tubules. 32 This can lead to bacterial regrowth which prevents periapical healing and retreatment is required. 33 Various methods like scanning electron microscopy, digital radiography, micro-CT and confocal scanning microscopy, can be advocated to assess the amount of residual sealers in the canal after removal of the obturating material. Other methods like bacterial culture, glucose penetration or fluid filtration techniques can also be employed to evaluate the sealing ability of endodontic root sealers. 34 The drawback of these laboratory leakage methods is that the selection of extracted teeth with anatomical variations leads to unreliable results. 35 In this study, confocal microscopy was employed to validate the amount of remaining sealer residue after removal since it delivers the fluorescence detection of sealer penetration along the dentinal tubules. Confocal microscopy is a better choice in studies like this as it provides better contrast and well-defined images and can give better results even with thicker specimens. 34
The current study observed that the penetrability of all the sealers was increased at 5 mm than at 3 mm from the apex. Comparable findings were evaluated by studies done by Khullar et al. 36 and Camilleri, 37 and Mc Micheal et al. 38 stated that the dentinal tubules are comparatively fewer in number and also the size of tubules in the dentin reduces drastically as we go apically. Also, it is seen that the apical part of the radicular canal shows marked variations in the structures, such as, there might be irregularity in the direction and thickness of the dentinal tubules or there might be no tubule at all. Sometimes the tubules might be blocked, because of the existence of cementum-like tissue at the apical one-third of the root canal system. The flow of sealer into the dentinal tubules is reduced due to the inefficacy of the irrigant to reach the apical region of the radicular pulp and eradicate the smear layer. 39
The outcome of this study is in agreement with those of another laboratory study, which analysed that the sealers were not eliminated from the dentinal walls of the roots. However, CeraSeal sealer residues were significantly higher, compared to other sealers in the canal tubules. 40 The study by Tucer et al. reported that calcium phosphate silicate sealers form a good bond with tooth structure due to less shrinkage during the setting process as compared with the tricalcium silicate sealer that has low bond strength due to the inability to form tag-like structure. 41 The conjecture was not declined as none of the bioceramic sealer was removed from the canal specimens completely.
The major limitation of this study is that there is no standardization on the amount of sealer being used in each sample. The study has another limitation the single cone technique is being used for obturation as claimed by the manufacturer, but studies have shown that the continuous wave technique is a successful way of obliterating the lateral and accessory canals. 42 Calcium silicate sealers have revealed better results with a new approach of hot-modified obturation technique. 43 Also, the study is an ex-vivo analysis so the outcome of this study may not conclude the same results in clinical oral conditions. Further studies must be performed to know the extended effect of various bioceramic sealers on clinical success and their retreatment protocol in case of failure.
Conclusion
In conclusion, the penetrability of three bioceramic sealers into canal tubules was significant at different depths. However, in the case of retreatment, no sealer was entirely removed from the dentinal tubules of the endodontic canal. The remnants of sealer material with CeraSeal were significantly more, compared with other bioceramic sealers. Further research is indicated as current techniques for retreatment are inadequate for the total eradication of endodontic materials.
Footnotes
Acknowledgements
The authors would like to acknowledge the Council of Scientific and Industrial Research—Indian Institute of Integrative Medicine (CSIR-IIIM) for supporting this work.
Author Contributions
Conceptualization, D.C.; methodology, D.C.; software, A.G.; validation, N.B.; resource, data curation, writing and supervision, D.C. All investigators have acknowledged the published version of the document.
Clinical Significance
A change of era from the application of resin sealers to bioceramic sealers has revolutionized the successful outcome of endodontic treatment. In cases of endodontic retreatment, these sealers need to be completely removed from the canal to provide a successful endodontic therapy. Thus, more clinical trials need to be performed to achieve a completely clean canal that is free of sealer remnants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was conducted by the ethical standards Declaration of Helsinki (1964), and the research study plan was supported by the Ethics Committee of the Institute (Ref No.:IES/2023/04).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable