
Abstract
Initially defined by Robinow et al. in 1969, Robinow syndrome is an exceptionally uncommon (1:500,000) hereditary disorder showing five distinct phenotypes. Although skeletal system symptoms are intense in all phenotypes, maxillofacial indications and genital organ hypoplasia are also present. Maxillofacial appearances can be listed as follows: hypertelorism, midface hypoplasia, wide and flat nose, low nasal bridge, downturned oral commissures, low-set ears, and micrognathia. In oral manifestations, gingival hyperplasia, tongue, and dental abnormalities are frequently encountered. The detection of intraoral and extraoral findings by the dentist plays a significant role in the diagnosis of this disease. Additionally, every new case documented will help dentists plan treatment approaches. Therefore, in this case report we aimed to describe the manifestations of a patient with Robinow syndrome who was referred to us by a pediatric cardiologist for her dental treatments and also the treatment approach under general anesthesia.
Introduction
In the literature, Robinow syndrome was first reported by Robinow et al. in 1969, and they reported the main characteristics of the syndrome as mesomelic limb shortening, hemivertebrae and genital hypoplasia. 1 Cardiovascular disorders, renal abnormalities, musculoskeletal dysplasia and craniofacial deformities might also accompany. 2 Although the incidence of Robinow syndrome was approximately 1:500,000, a lower prevalence and a 1:1 boy-to-girl ratio of incidence have been reported since 5–10% of patients were lost in infancy or early childhood. 3
Notwithstanding the fact that there are a number of studies conducted on different orofacial and dental features of Robinow syndrome in the literature, published reports, especially for the oral symptoms and dental treatment protocols of pediatric patients with Robinow syndrome, are limited. The aim of this case report was to present the management process of the dental problems of a pediatric patient with Robinow syndrome under general anesthesia (GA).
Case Report
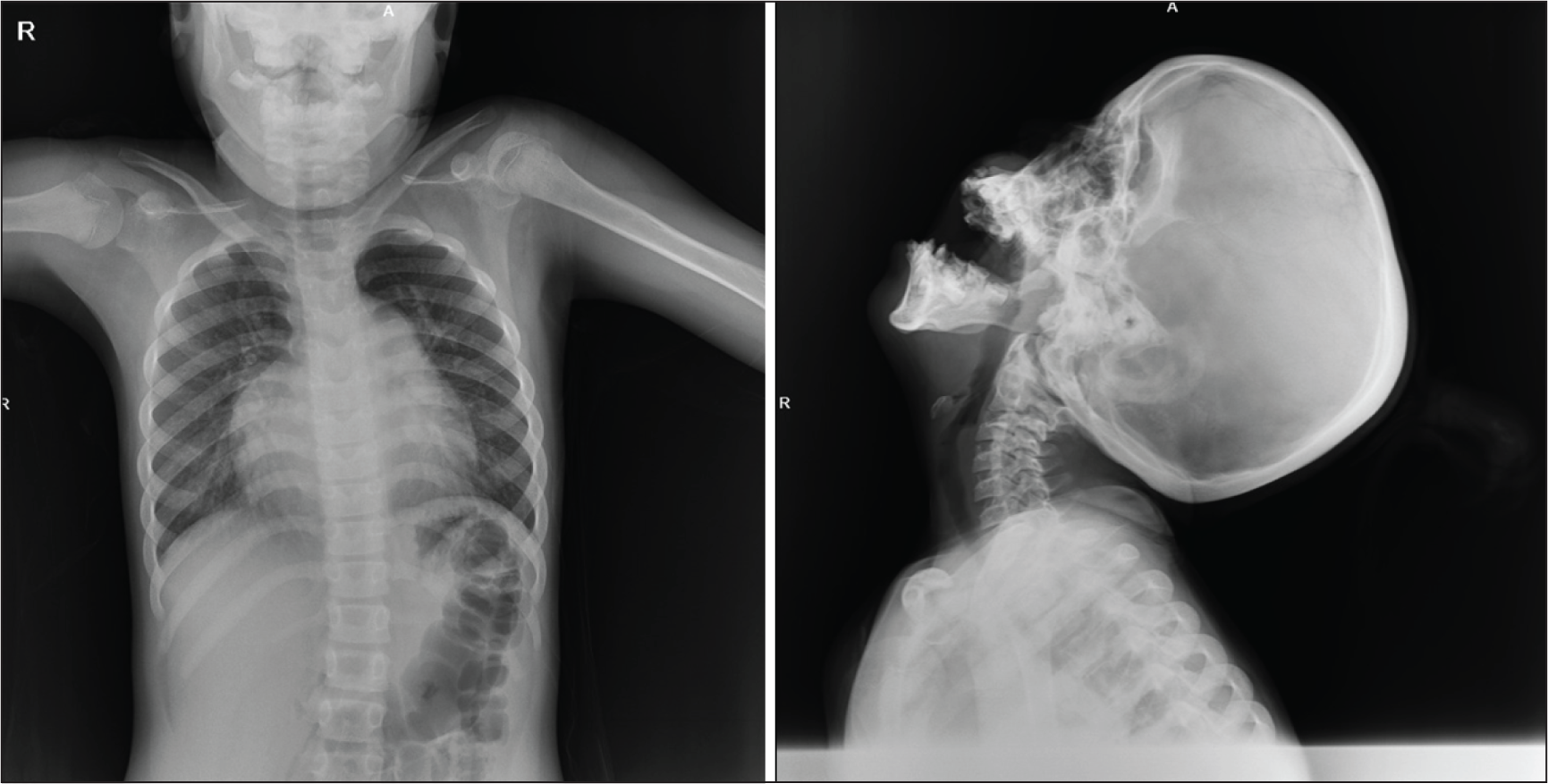
A 7-year-old girl with Robinow syndrome, who was in pediatric cardiac follow-up due to autism spectrum disorder, was referred to Ataturk University Faculty of Dentistry, Department of Pedodontics, for dental treatments. The patient had dental aesthetic concerns and toothache. In the anamnesis, we learned that the patient was diagnosed with autosomal dominant Robinow syndrome-2 (DRS2/osteosclerotic form) as a result of the genetic analysis performed at the age of 6 years. There was no consanguineous marriage in the parents, the gestational age of the mother was 33, the birth was post-term (42 weeks + 3 days), and the other two siblings were normal. In the physical examination performed, short stature, vertebral anomalies, scoliosis, mesomelic short extremity, short and wide fingers, macrocephaly, dysmorphic face, prominent forehead, hypertelorism and flat and wide nose were observed (Figure 1). In addition, anomalies were observed in the skull and spine extraoral radiographs of the patient (Figure 2).
Photo of the Patient’s Posture, Hand, Foot and Face.

Spine and Skull Radiographs of Patient.
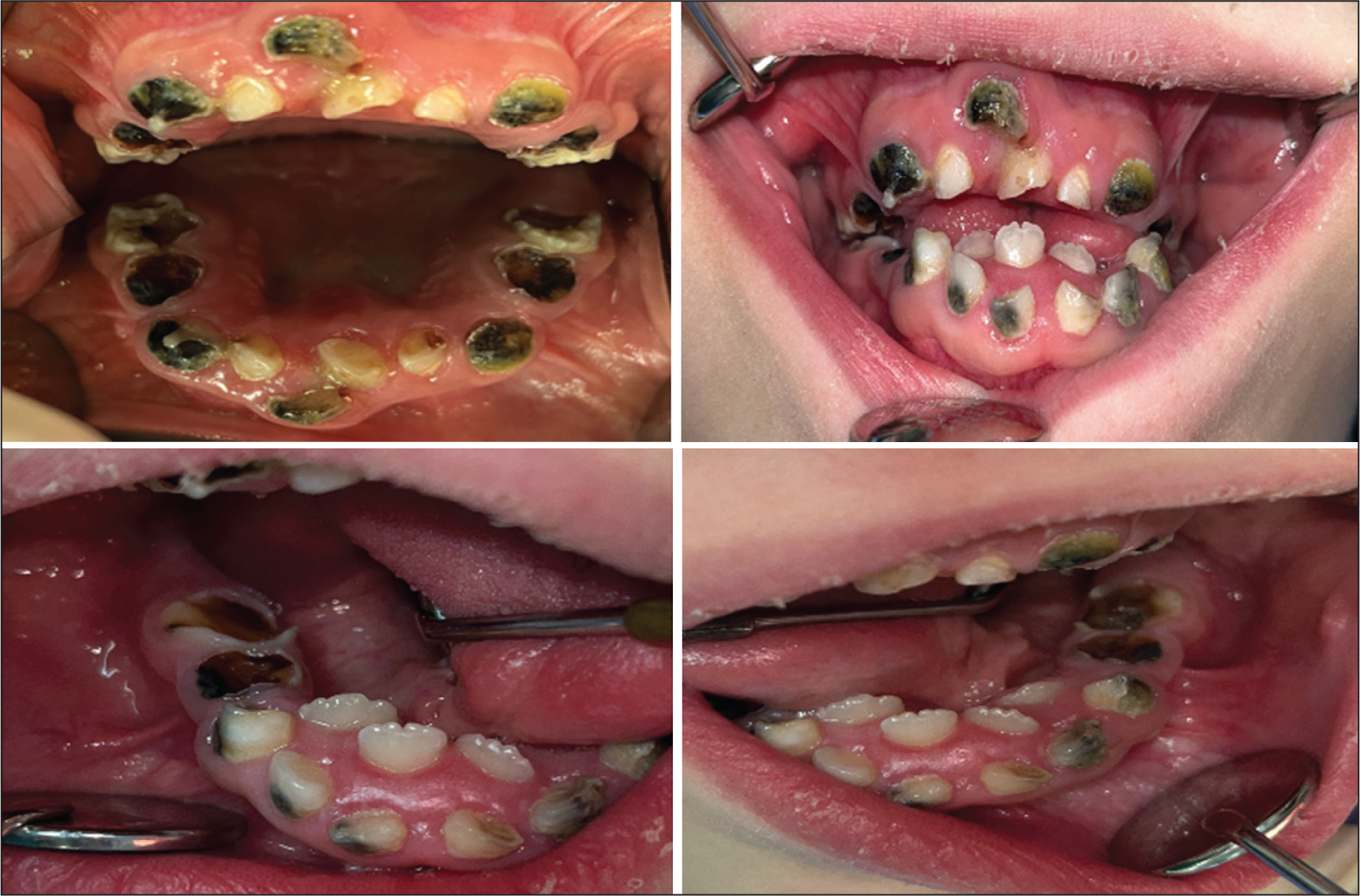
Intraoral examination manifested micrognathia, triangular mouth, thin upper lip, narrow and deep palate, gingival hyperplasia, macroglossia, bifid tongue, severe malocclusion (crowding, anterior open bite and lack of interocclusal tooth contact), agenesis-associated missing permanent teeth and delayed eruption. The patient retained all of her primary teeth with only mandibular permanent incisors. In accordance with the radiographic examination revealing carious lesions in all primary teeth, we concluded that there was a deficiency in permanent tooth germs (25, 35, and 45), and the roots of the primary molars were short (Figure 3).
Intraoral Photos of the Patient.
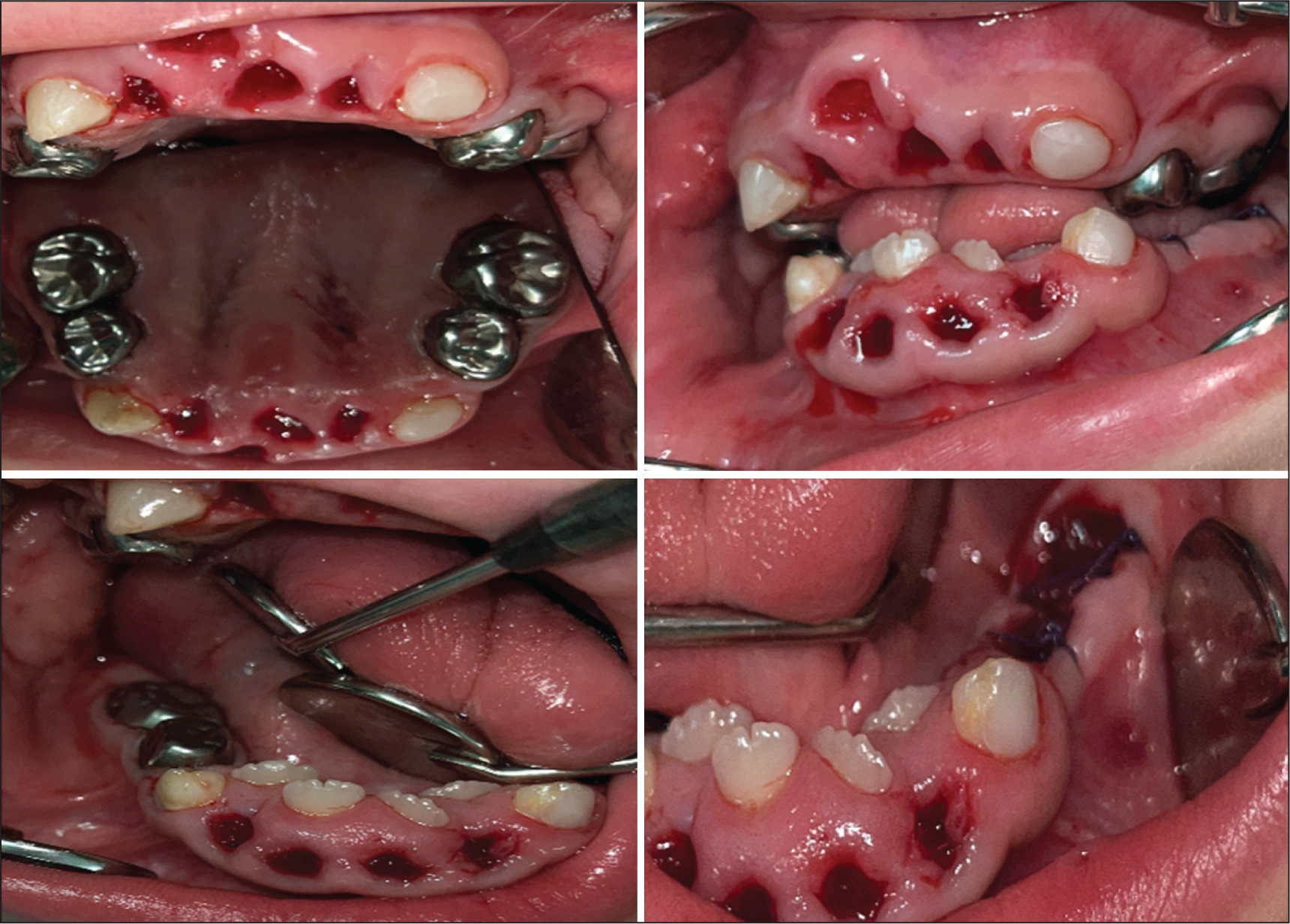
By consulting with pediatricians, pediatric cardiologists, and anesthesiologists, we planned dental treatment under GA for the uncooperative patient. Primary canines were restored with composite resin, stainless steel crowns were placed on teeth # 54, 55, 64, 65, 84, and 85 after MTA amputation, and teeth # 51, 52, 61, 62, 71, 72, and 81, 82 were extracted due to physiological mobility and # 74 and 75 due to infection (Figure 4). As no complication occurred following GA, the patient was discharged on postop day 1. In the patient’s follow-up after 1 week, we observed that extraction sockets started to heal, and patient’s pain complaints disappeared.
Intraoral Photos of the Patient After General Anesthesia.
Discussion
Robinow syndrome is one of the rare genetic disorders accompanied by limb and vertebral anomalies, dysmorphic facial appearance, and various systemic abnormalities. Surgical interventions for vertebral anomalies and scoliosis, facial reconstruction in selected cases for psychological support, treatment procedures for associated systemic anomalies, and sometimes hormonal treatments are used in the management of the syndrome. 4 Since the typical craniofacial appearance seen in the syndrome is also accompanied by orthodontic problems, severe dental caries, and agenesis, it is very important to eliminate these problems for an effective treatment.
All necessary dental treatments of our patient were performed under GA. Because of the narrowing attached gingiva in the mixed dentition, mucogingival surgeries are recommended to be postponed until gingival thickness increases. 5 Thus, mucogingival surgery was not performed on our patient, and her parents were informed. Additionally, she was also examined by the orthodontists, and due to insufficient number of teeth in the anchorage, poor oral hygiene, and as the child was in the mixed dentition, the narrow maxilla was not intervened, and the orthodontic treatment was postponed.
The incidence of Robinow syndrome is higher in Turkey, Oman, and some parts of the Czech Republic. This may be associated with the high rate of consanguineous marriages in these countries. Although consanguineous marriage appeared to play an important role, parental age was not found to be an important factor. 2 In our case report, no history of consanguineous marriage in the family of the patient with DRS, maternal age (33), and post-term delivery were the important points to notice.
Robinow Syndrome is a genetically heterogeneous disorder with autosomal dominant (DRS) and autosomal recessive (RRS) genotypes. While two genes, ROR2 and NXN, were reported to be responsible for RRS in recent studies, heterozygous pathogenic variants in WNT5A, FZD2, DVL1, and DVL3 were also remarked for DRS. 6 In RRS, musculoskeletal dysmorphology appears to be more severe than in DRS. 7 In our case, genetic analysis indicated that our patient had DRS due to DVL1 gene mutation.
Nevertheless, malocclusion and gingival hyperplasia were reported to be more severe in DRS. In addition, supernumerary teeth were observed only in DRS, whereas high arched palate was seen only in RRS.7,8 In Robinow syndrome, the presence of the relatively small face, ocular hypertelorism, and forward-pointing alae nasi resemble the fetal face. Thus, the term “fetal facies” was adopted by Robinow’s proposal. 2 Similar to the previously reported cases, bifid tongue, narrow and deep palate, severe malocclusion, gingival hyperplasia, agenesis and delayed eruption were the oral findings detected in our case. Additionally, downward sloping mouth corners, frontal prominence, triangular mouth, thin upper lip, midface hypoplasia, micrognathia, short and snub nose, wide nostrils, hypertelorism and depressed nasal bridge were observed in parallel with the previously reported typical craniofacial features.7,8
Conclusion
Management of Robinow syndrome requires a multidisciplinary approach, and these patients must have good oral health. Neglect of oral hygiene by parents due to various systemic problems in these patients may result in poor oral hygiene and gum diseases. Therefore, these patients should be monitored with regular follow-ups, and their oral hygiene should be maximized. Maintaining the optimum level of oral hygiene starting from a younger age will help improve the prognosis of orthodontic or surgical treatments, which will be applied for correcting severe malocclusion.
Footnotes
Acknowledgements
We thank the parents for permission to share patient records and photographs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval from Institutional Review Boards (IRBs) was obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.