
Abstract
Dyskeratosis congenita (DC) is an uncommon disease characterized by nail dystrophy, cutaneous hyperpigmentation, leukoplakia, pancytopenia, and malignant transformation. There can be some oral and dental changes such as oral leukoplakia, increase in tooth decay, hypodontia, thinning of enamel layer, aggressive periodontitis, intraoral brown pigmentation, missing tooth, taurodontism, and blunted roots. Most of cases belong to dermatology or pediatrics department. There are few reports about dentistry. The aim of this report is to lay emphasis on this fatal syndrome among dentists about the multisystem findings and oro-dental changes. Thus, this information may aid dentists in early diagnosis. A case of 21-year-old male diagnosed with DC is reported.
Introduction
Dyskeratosis congenita (DC) is an uncommon hereditary syndrome. 1 In 1910, it was first determined by Zinsser. 2 Thereafter, other cases were reported by Engman and Cole et al and this syndrome is also mentioned as Cole–Engman syndrome or Zinsser–Cole–Engman syndrome. 3 DC is frequently seen in men and occurs between 5 and 12 years. Classic triad of this syndrome is skin pigmentation, nail dystrophy, and oral leukoplakia. DC is a fatal disease. Most of the patients undergo aplastic anemia and malignant transformation in the keratotic white patches. 1 , 3
The most serious complications in DC patients are bone marrow failure and pulmonary fibrosis. 4 It becomes more difficult to intubate, especially in the presence of mass. In addition, tooth decay, gingival hyperplasia, alveolar bone loss and malignant lesions are common in the oral cavity. Gingival hyperplasia can lead to bleeding during intubation. 5 , 6
This report will discuss the oral and dental features, and treatment options of DC with a review of recent literature.
Case Report
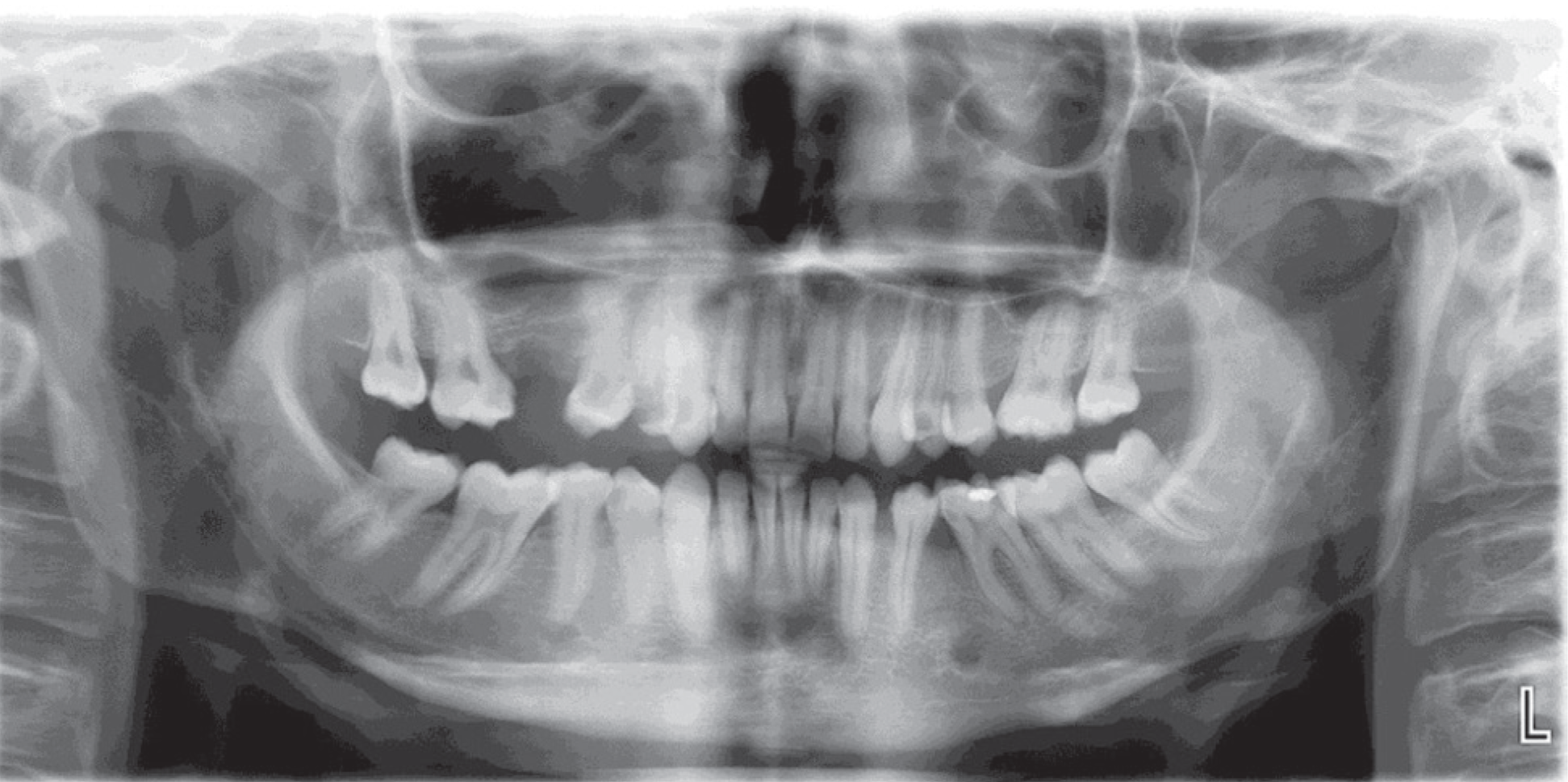
A 21-year-old male diagnosed with DC was admitted because of multiple caries and gingival problems to Department of Dentomaxillofacial Radiology. The patient also had acid reflux. The patient looked pale, but the vital signs were within normal limits. Hyperpigmentation was seen on the forehead. Nails of both fingers were cracked and there was also nail atrophy. The patient had pulled on glove because of esthetic reasons when he referred to the clinic. Inadequate oral hygiene and extensive caries were observed in clinical examination of the patient (Figure 1). On clinical and radiological examination, missing teeth and taurodontism was observed, the right upper first and second premolar and the lower first molar teeth (14,15,36) had deep carious lesion which should be treated with endodontic treatment. There were also carious teeth that were observed in both arches (12,13,17,21,24,26,27,37,44,46) (Figure 2). Plaque accumulation was also observed especially in gingival border of anterior upper and lower teeth. Alveolar bone loss most marked around posterior regions of both jaws was observed. The tongue was normal in size but geographic and rusty tongue was observed. A white patch of approximately 0.5 cm in diameter was observed on the buccal mucosa, bilaterally (Figure 3). Erythematous lower lip was observed. Lesion was not scrapable with gauze. Other oral mucosal surfaces were normal. A biopsy from this hyperkeratotic lesion was recommended. But, the biopsy was not performed as the patient refused to undergo the biopsy. So, no definite diagnosis of the hyperkeratotic lesion could be made, although it was suspected to be a leukoplakia. The treatment plan included a strict prevention protocol as follows:
Periodontal treatment. Endodontic treatment of the 14,15,36. Restorations of the all decayed teeth. Although the patient refused to undergo the biopsy, he was consulted to the Department of Oral and Maxillofacial Surgery for the intraoral hyperkeratotic lesions. After establishing optimal oral health such as restoration of carious teeth and periodontal treatment, oral hygiene instructions were given to the patient and he was referred for rehabilitation with crowns and bridge prosthetics.
The Intraoral Photographs Showing Upper (a) and Lower (b) Jaws with Carious Lesions, Teeth Pigmentations, and Inadequate Oral Hygiene

Panoramic View
Intraoral Photograph Showing a White Patch on the Buccal Mucosa

Soon after, the patient was referred to necessary departments, firstly periodontology department because of periodontal problems which was appeal reason of the patient.
Discussion
Between eighty and ninety percent of the patients die early because of the complications of DC. Pancytopenia-associated hemorrhage and opportunistic infections are frequently observed in patients with DC. 7 In addition to this, fatal neoplasms such as myelodysplastic syndrome, acute myeloid leukemia, and solid tumors can be observed in patients. 8 Alter et al 7 evaluated 552 reports of DC in English literature and found 52 patients (9.4%) with 61 cancers. Solid tumors were observed in 60 cases and one case had acute myeloid leukemia. The most frequently observed malignancy was squamous cell carcinomas of head and neck region (40%) and skin (13%) followed by anorectum (10%) and lungs (6.6%). 7
Bongiorno et al 9 reported a case with DC about malignant transformation of oral leukoplakia. Panda et al 10 also reported a case of DC with acute myeloid leukemia and oral leukoplakia. The most frequently observed pulmonary situations in patients with DC involve pulmonary fibrosis with damaged gas exchange and the pulmonary vasculature anomalies. 7 The mortality rate because of pulmonary complications is estimated between 10 and 15%. 8 After all, previous studies have reported that complications of DC occur due to the use of drugs that cause pulmonary toxicity, particularly in patients planned for bone marrow transplantation. 11 Other pulmonary complication is the common infection which develops because of immunodeficiency. 12 , 13
Early childhood caries is a frequent finding which affects 17% of DC patients with other dental changes such as short-blunted roots and periodontal problem. 2 , 13 , 14 These findings are thought to be because of anomalies within ectodermal origin structures, which conclude the enamel layer or its epithelial attachment defects. 15 In this case, extensive carious lesions, and plaque accumulation were observed and, according to patient’s anamnesis, he also had early childhood caries.
In oral cavity, the white patch can affect the buccal mucosa, tongue or palate, however, tongue is most affected area. 1 But in our patient, white patch was seen in buccal mucosa.
In the report of Atkinson et al, 13 17 individuals with DC were evaluated and the most frequently observed oral findings were reported as oral leukoplakia (65%), decreased root/crown ratio (75%), and mild taurodontism (57%). Ko et al 16 reported some dental changes that were suggestive of shortened, blunted roots and enlarged pulp chambers. In our case, mild taurodontism and enlarged pulp chambers were observed in the panoramic radiograph although root length was observed as normal.
Davidovich et al 6 reported a case with DC and described extensive alveolar bone loss in all quadrants. In this case, similarly we observed alveolar bone loss.
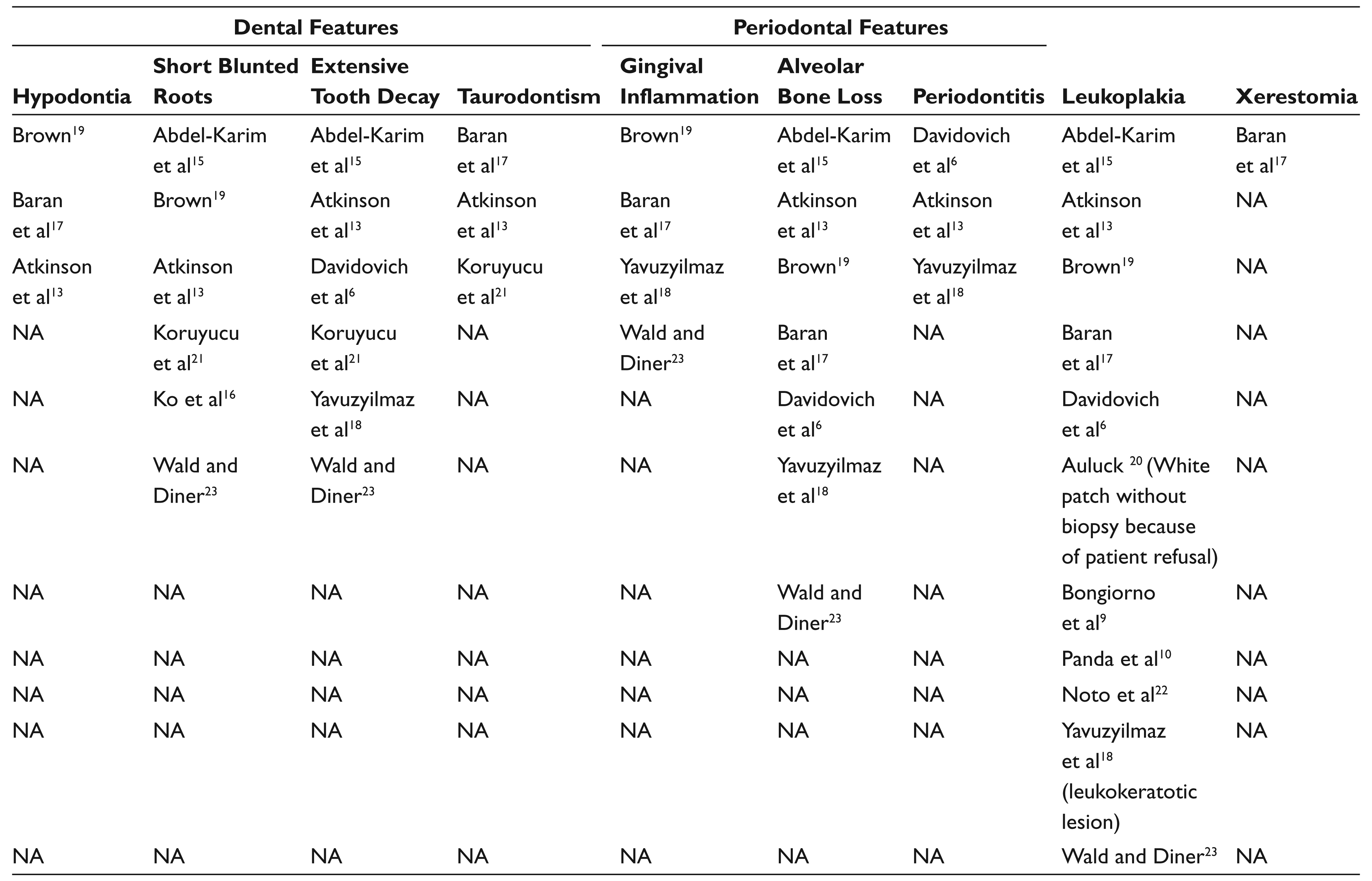
In the report of Baran et al, 17 some similar dental features such as hypodontia, delayed tooth eruption, short blunt roots, increase in tooth decay, gingival problem and hemorrhage, alveolar bone loss, leukoplakia of buccal mucosa, and irregular ulcers were observed. Yavuzyilmaz et al 18 also reported a case of DC with some dental findings such as tooth decays and mobility, gingival recession and hemorrhage, short-blunted roots, excessive alveolar bone loss and leukokeratotic lesion on the buccal region. Table 1 shows the case series of DC with intraoral findings.
Oral and Dental Features in DC with Literature Review
In conclusion, DC is a rare syndrome and there were a few studies in the field of dentistry in the English literature and also in my country. Dentists should recognize this important disease and direct the patient to the hematology department in case of doubt. Regular follow up of the patients with DC is mandatory for malignant transformation possibility. Of course, it is important to solve aesthetics, occlusion, and functional problems. But the psychological condition of the patient is also important. This would bring positive effect in the patient’s life.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.