
Abstract
Aim:
Certain systemic risk factors associated with tooth loss are much more common. However, population-based studies that have investigated the impact of these diseases on tooth loss and age groups are not found. The study aimed to evaluate the relationship and change in effect by age in systemic diseases with the loss of 13 or more teeth in adults and elderly people in Brazil, comparing two periods, 2013 and 2019.
Materials and Methods:
A total of 49,553 participants aged 18 years or older from the National Health Survey in 2013 and 77,862 in 2019 were used. Data was sorted out into five different age groups. Using a Poisson Regression model, the magnitudes of associations were analysed with sequential adjustment (95% CI).
Results:
All diseases (Arterial hypertension, Rheumatoid Arthritis, Diabetes, Depression and Hypercholesterolemia) were associated with tooth loss (statistically significant magnitudes of associations) in the total population in 2013 and 2019. The magnitudes of associations were decreasing in older age groups and it was only statistically significant with cardiovascular diseases and tooth loss in ≥ 65-year age group (1.10 (95% CI:1.05–1.15)).
Conclusion:
More than 13 teeth loss were associated with Arthritis/rheumatism, Depression, Diabetes Mellitus, Hypercholesterolemia, Systemic Arterial Hypertension and cardiovascular diseases, especially among younger age groups, which suggests a focus on the prevention and control of such systemic diseases and primary dental care.
Introduction
According to the Global burden of oral conditions of 1990–2010 1 , tooth loss is a prime indicator for better health and quality of life. Periodontal disease is the main factor associated with tooth loss, although its cause is considered multifactorial, among 80%–90% of the total population.2,3 Tooth loss is often associated with the ageing process, but it also affects younger people.4,5 According to WHO, an adult persons’ functional dentition merely consist of a minimum of twenty permanent teeth. 6 The presence of comorbidities, especially chronic diseases, influences the occurrence of tooth loss in several studies.4,7–9 An increased prevalence rate in relation to tooth loss has been shown in past decades with Arthritis/rheumatism, Depression, Diabetes Mellitus, Hypercholesterolemia, Systemic Arterial Hypertension and cardiovascular diseases. 10 In such a scenario, untreated chronic periodontal disease may cause tooth.4,8,7,9
The impact of such systemic conditions was studied in the elderly population, 11 although studies have found significant evidence of this relationship in middle-aged adults.8,12 However, it is still not clear in what age group the presence of health conditions can lead to higher tooth loss.10,13 Other studies have investigated these relationships by restricting the study population to those exposed to potential confounding factors, such as smoking, 13 rural residents, 13 gender, 13 and income, 11 without using adjusted multivariate models as a control mechanism and presenting a smaller sample size.
The oral health scenario in Brazil and access to dental services reveal a country with many inequalities in these aspects. 14 The prevalence of tooth loss is still high in recent decades.15,16 Historically, the number of oral health teams has increased steadily since 2004, although there has been a slowdown since 2013.16,17 This was due to political changes characterized by budgetary restrictions and expressed in successive changes in the national coordination of oral health and the Brazilian Ministry of Health. 18 These declines in health investments culminated with the approval of Constitutional Amendment No. 95 in 2016, which established a spending limit for basic expenses. 17
In Brazil, no population-based epidemiological study has been carried out with the aim of investigating the impact of different health conditions on tooth loss, in addition to removing the effect of several confounding factors, including young and elderly adults in the analysis, and even comparing the relationships in two relevant time cuts for the Brazilian Health System, due to reduced investments. The study aimed to evaluate the relationship and change in effect by age in systemic diseases with the loss of 13 or more teeth in adults and elderly people in Brazil, comparing two periods, 2013 and 2019.
Materials and Methods
Study Population
Using data from the National Health Survey (PNS) in 2013 and 2019, a cross-section study was conducted by the Ministry of Health of Brazil in partnership with the Brazilian Institute of Geography and Statistics (IBGE) and the Oswaldo Cruz Foundation 16 . The purpose of the PNS is to present data on the health situation and lifestyles of the Brazilian population (IBGE, 2020). The survey is conducted every 5 years and maintains essential aspects of the investigation which makes it possible to compare the results between the years in which the survey was carried out. The study population included adults aged 18 or over in 2013 and 15 or over in 2019, living in urban and rural areas.16,19
Of the total of 60,202 participants in the 2013 PNS, those who had missing information for health conditions (DM = 5,875, SAH = 1,778 and hypercholesterolemia = 2,331) and covariates (race/skin colour = 3) were excluded. And of the 90,846 participants in 2019, those under 18 years of age (n = 2314) were excluded, as well as missing information for health conditions (DM = 4936, SAH = 1,550, and hypercholesterolemia = 1,900) and covariates (race/colour of skin = 10, age = 4,588). For this analysis, participants aged 18 years were eligible, with 49,553 participants in 2013 and 77,862 in 2019.
Response Variable
Our study had as an outcome the tooth loss of 13 or more teeth. First, the participants answered the following questions: “Remembering your upper teeth, did you lose any teeth?” and “Remembering your bottom teeth, did you lose any teeth?”. Those who said they had lost both top and bottom teeth were asked to say exactly how many they would be. The response variable utilized is binary (categorical) having two possible values: <13 and ≥13 missing teeth.
Explanatory Variables of Interest
The binomial explanatory variables, equivalent to health conditions, were the presence (No and Yes) of SAH, DM, CVD, depression, hypercholesterolemia, and Arthritis/rheumatism identified through the following questions: “Has a doctor ever given you the diagnosis of high blood pressure (high blood pressure)?” and “Did this arterial hypertension (high blood pressure) occur only during some period of pregnancy?”; “Has a doctor ever given you a diagnosis of diabetes?” and “Did this diabetes occur only during some period of pregnancy?”; “Has a doctor ever given you the diagnosis of a heart disease such as a heart attack, angina, heart failure or otherwise?”; “Has a doctor or mental health professional (such as a psychiatrist or psychologist) ever given you a diagnosis of depression?”; “Has a doctor ever given you the diagnosis of hypercholesterolemia?”; “Has a doctor ever given you a diagnosis of arthritis or rheumatism?”. Those who responded that they had received a medical diagnosis of hypertension or diabetes only during pregnancy were considered not to have such health conditions.
Covariates
The following adjustment variables were considered because they are related to both exposures and outcome as confounders2,5–9,11,16,20–23: Gender (male/female); Current level of education (complete higher education, complete secondary education, complete primary education and incomplete primary education or less); Age (categorical in the descriptive analysis, being 18–34, 35–44, 45–54, 55–64 and >65 years old, and continuous in years in the multivariate analysis); Macro region of Brazil (since Brazil has continental dimensions: Southeast, South, Midwest, Northeast or North); Region (urban/rural); Smoking (no/yes); and Abusive alcohol consumption (no/yes). It was considered abusive to consume five or more doses for men and four or more doses for women, on a single occasion, in the last 30 days. 24
Statistical Analysis
Statistical analysis was performed using the Stata 13.0 software (Stata Corporation, College Station), and to consider the complexity of the sample design, the weights were considered using the SVY command set of the statistical software. The magnitudes of the associations were measured using the prevalence ratio (PR) and their respective 95% CI, using Poisson Regression. We perform five models measuring the associations between each exposure related to health conditions and tooth loss. Model 1 was without adjustment. Model 2 included adjustments for the macro-region and urban/rural region of Brazil. Model 3 included model 2 plus age, sex, race/skin colour, and model 4 included model 3 plus current education. The preferred statistical model was model 5 which included model 4 plus adjustment for smoking and alcohol abuse. After complete adjustment (Model 5), the interaction term between each exposure and age was included to confirm the modification presence and the effect of age on this relationship. For the multivariate analyses stratified by age group, the same adjustments were used, except for age.
Results
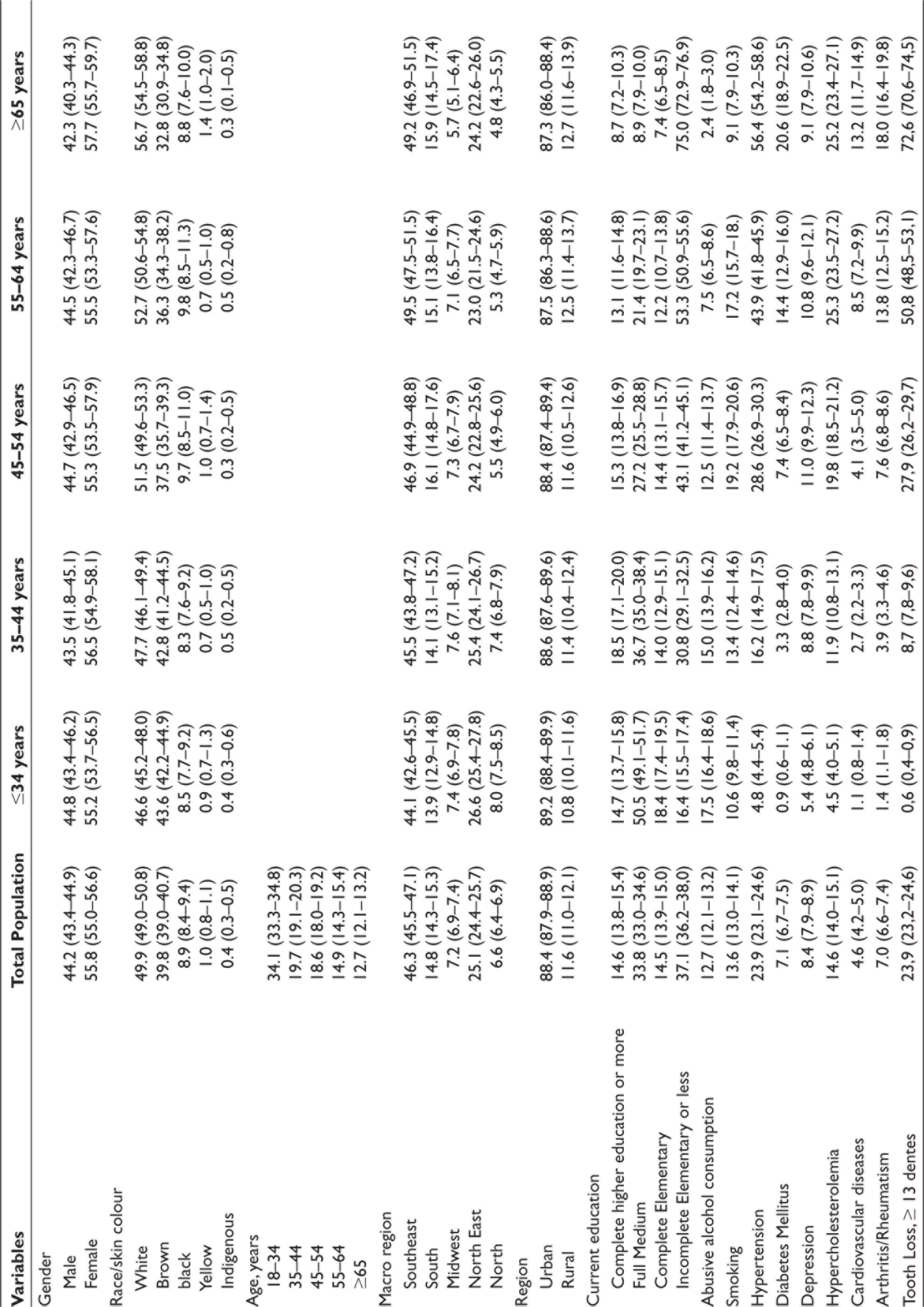
Tables 1a and 1b show the sociodemographic and health characteristics of the Brazilian population by total population and age groups in 2013 and 2019, respectively. It is observed that in all age groups, there are significantly higher frequencies of women, people who self-reported white and brown race/skin colour, living in the Southeast macro-region of the country and urban region. Lower frequencies are observed for those with a completely higher education level who abused alcohol and were smokers. The prevalence of tooth loss in 2013 was 23.9% (95% CI: 23.2–24.6) in the total population and showed an increase with advancing age, reaching 72.6% (95% CI: 70.6–74.5) in the age group 65 years or older. In 2019, we observed a slightly lower prevalence of tooth loss higher than 13 teeth for the total population (21.8%, 95% CI: 21.3–22.3), although a similar behaviour was observed with advancing age, reaching 69.2% in the age group 65 years or older (95% CI: 67.7–70.5).
Sociodemographic Characteristics (Brazil, 2013) with % (95% CI).
Sociodemographic Characteristics and Health Conditions (Brazil, 2019) with % (95% CI).
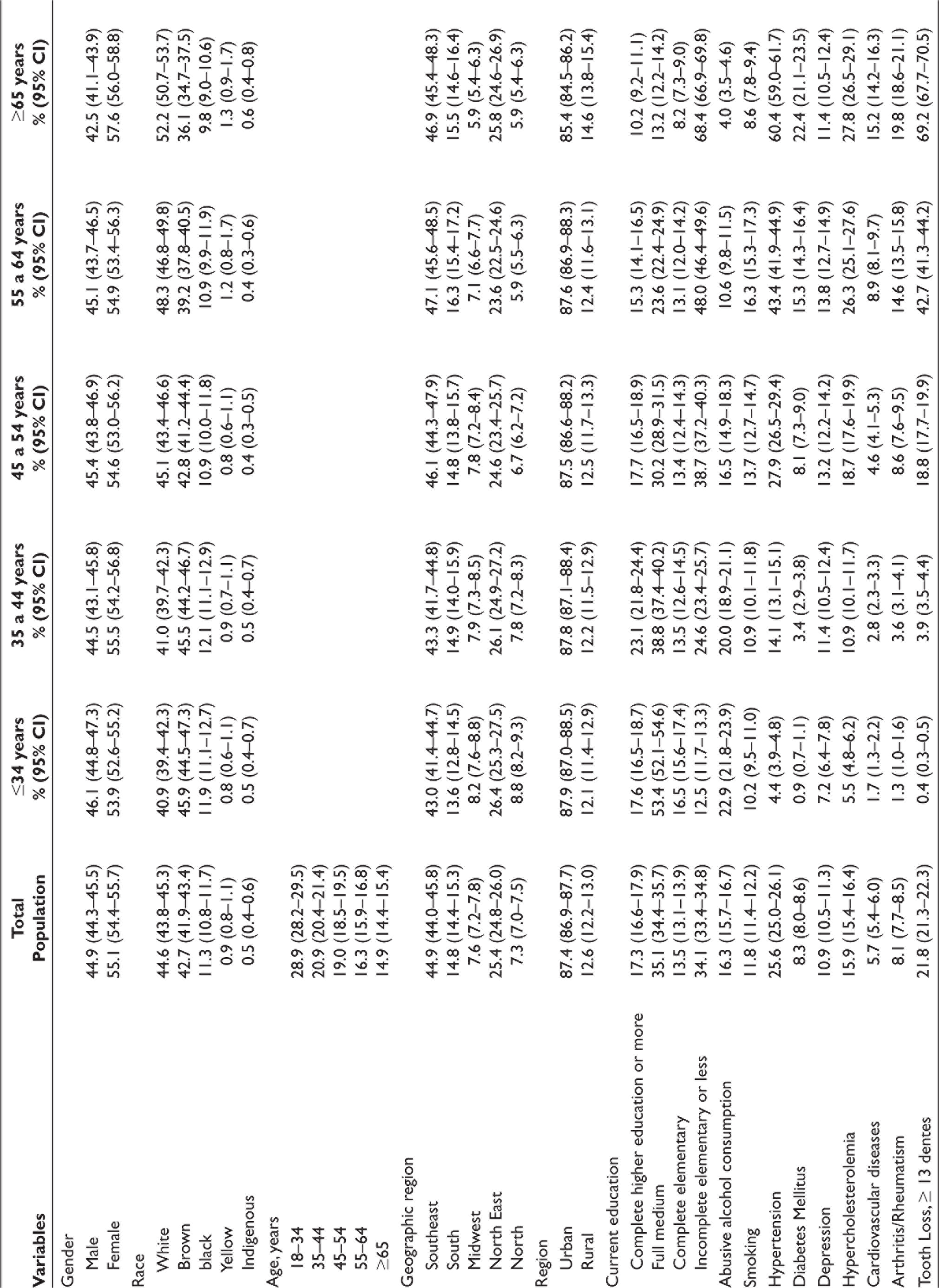
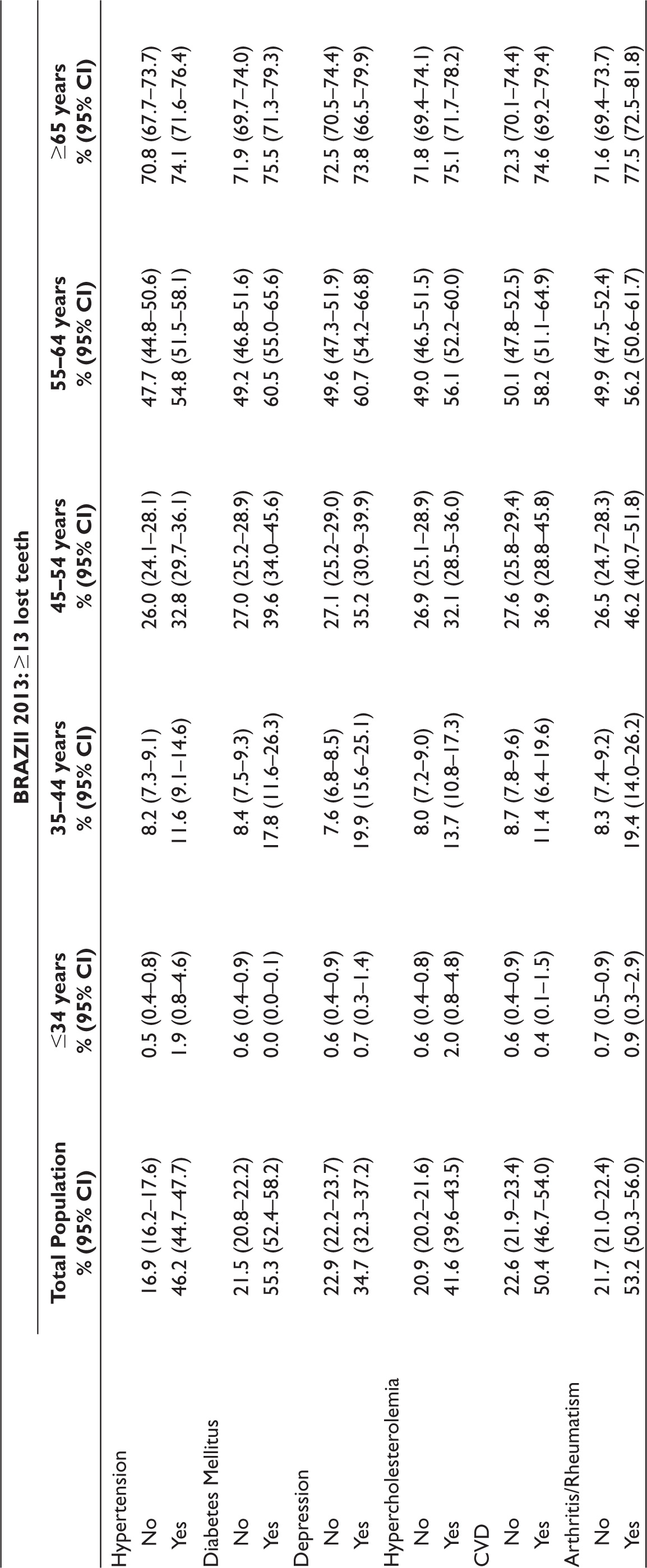
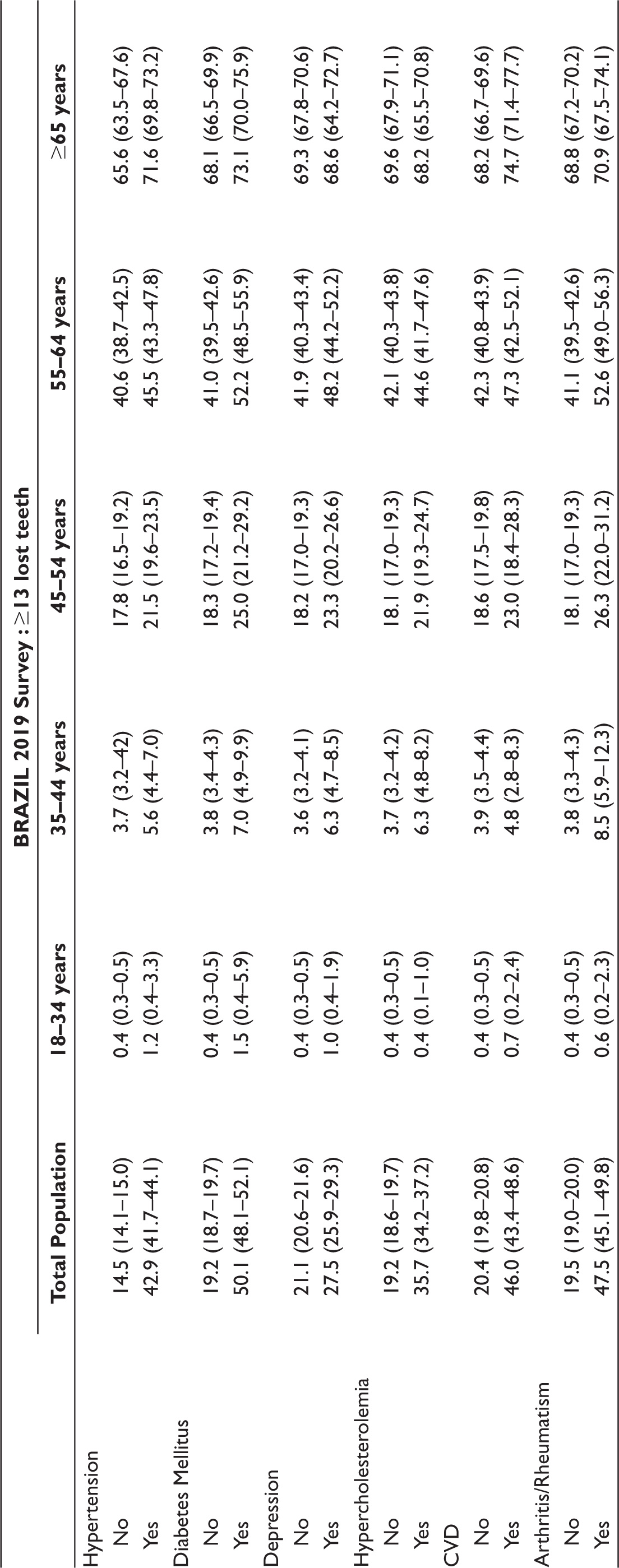
Table 2 shows the prevalence of 13 or more missing teeth according to health conditions. The prevalence was higher in individuals with a self-reported diagnosis than in individuals without in the total population. In the age group 18–34 years, in 2013, individuals without DM (0.6%: 95% CI: 0.4–0.9) and CVD (0.6%: 95% CI: 0.4–0.8) had a higher prevalence of 13 or more missing teeth than those with DM (0.0%: 95% CI: 0.0–0.1) and CVD (0.4%: 95% CI: 0.1–1.5).
Data Showing Prevalence of More than 13 Missing Teeth.
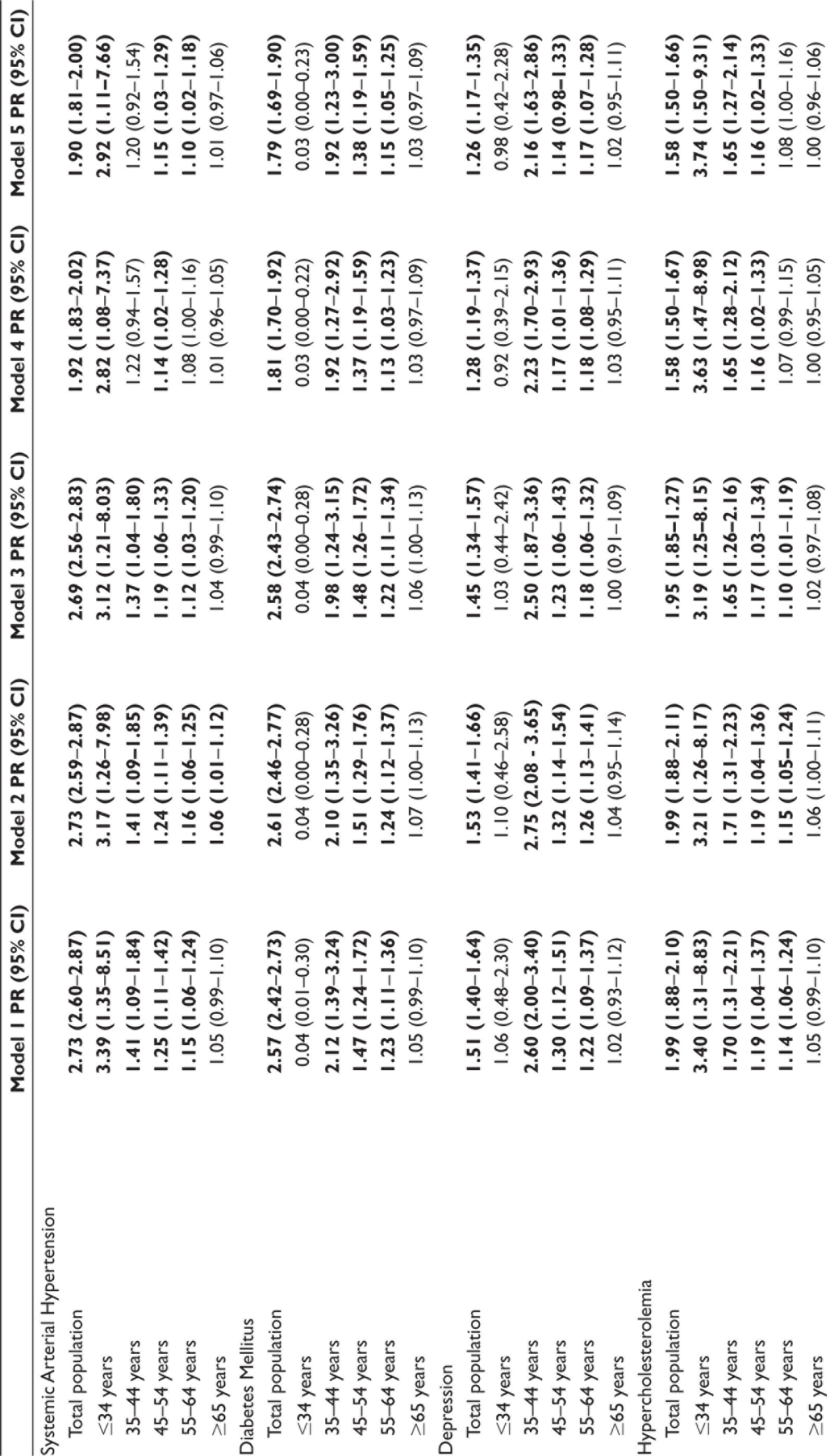
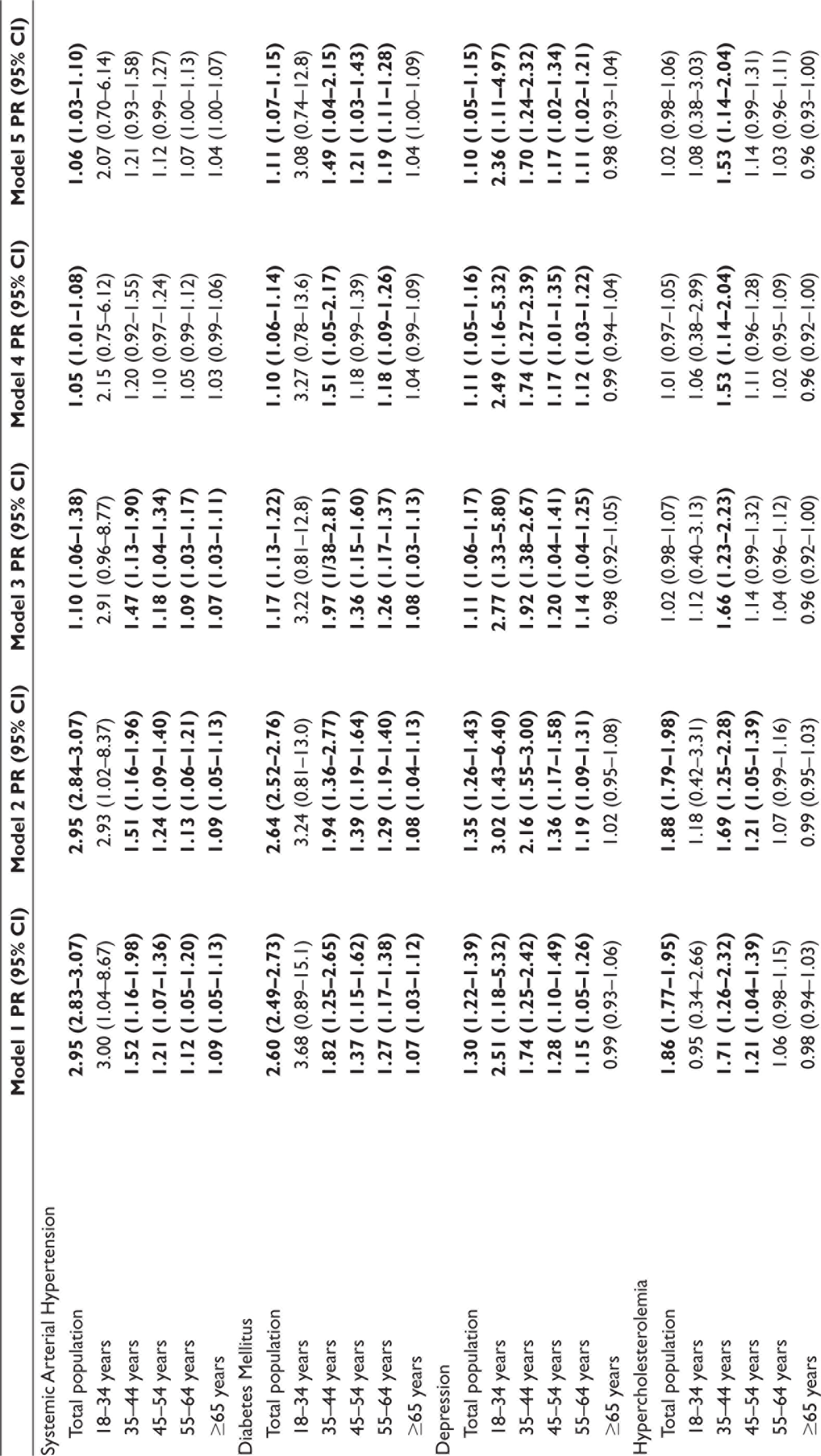
Tables 3a and 3b show the associations between health conditions and the loss of 13 or more teeth. After complete adjustment (Model 5), in 2013 and 2019, for the total population, we observed that all health conditions are related to a higher prevalence of tooth loss, except for hypercholesterolemia, which did not remain associated in 2019.
Associations of Systemic Conditions with Tooth Loss Greater than 13 Teeth, National Health Survey (Brazil, 2013).

Associations of Systemic Conditions With Tooth Loss Greater than 13 Teeth, National Health Survey (Brazil, 2019).
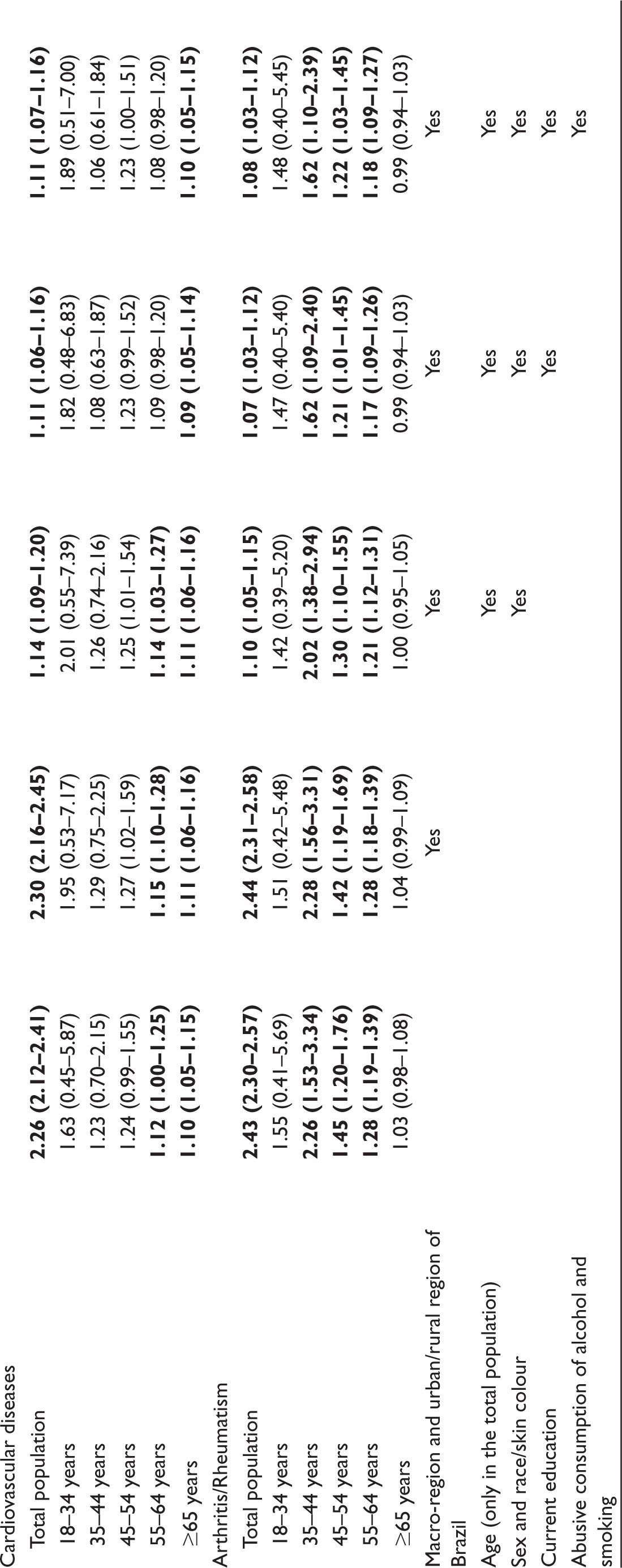
In the analyses stratified by age groups, after complete adjustment (Model 5), in 2013, SAH was associated with a higher prevalence of tooth loss in people aged 18–34 years, 45–54 years, and 55–64 years. DM and depression remained statistically associated in the age strata from 35 to 44, 45 to 54, and 55 to 64 years old, and hypercholesterolemia in age strata 18–34, 35–44, and 45–54 years. Arthritis/rheumatism was associated with age strata 35–44 and 45–54 years of age, but CVD only remained statistically significant in those aged 45–54 years old. We observed that with advancing age, in statistically significant age strata, there was a reduction in the magnitudes of associations (Table 3a).
In 2019, after complete adjustment (Model 5), we observed that SAH no longer represents a statistically significant exposure factor for tooth loss. DM remained statistically significant in the age strata from 35 to 44, 45 to 54, and 55 to 64 years old. Depression was statistically significant for tooth loss in all age groups, except for those aged 65 years and over. Hypercholesterolemia showed a statistically significant association with tooth loss only in the 35–44 years age group. CVD was statistically significantly related in people aged 65 years and over, and arthritis/rheumatism in the age strata from 35 to 44, 45 to 54, and 55 to 64 years old.
Discussion
Our study showed a strong correlation between systemic diseases with the loss of 13 or more teeth in the total population. As per WHO recommendation, the present study analysed 13 teeth as a minimum of twenty functional teeth are required for good oral health, 5 although it is not a consensus among similar studies.5,7,8,25 A synergistic effect on increasing tooth loss11,13 of those studied non-communicable chronic diseases has increased prevalence in recent decades13,26,27 and those may have low oral health index from caries or periodontal disease, having a multifactorial origin, lead to tooth loss.8,20,28
However, in our age-stratified analysis, only CVD was statistically associated with 13 or more teeth loss in the 65 years and older group (1.10: 95% CI: 1.05–1.15) in the 2019 analysis. This result suggests that old age is a higher risk factor for tooth loss than the presence of SAH, DM, depression, CVD, hypercholesterolemia, and arthritis/rheumatism,29,30 although other studies have found a good association between these diseases among the elderly.8,10,25,31 A presented varied results may be due to the varied sample size, age groups, statistical methods, confounding, and diagnostic factors. 10
A tooth loss association was higher in the 35–64 years group with a major effect by DM for both 2013 and 2019 as reported.7,27,32 An increased blood glucose level invited poor immune-inflammatory response mechanism that attracts bacterial pathogens in the periodontium and thus destruction of periodontal tissues. 9 Further DM leads to the accumulation of glycated substances in the cementum, causing impaired wound healing of periodontal ligament fibres and leading to tooth loss. 27
In France studies, SAH and more than 10 teeth loss were strongly associated under 65 years of age. 31 Similarly, in 2013, we found a significant relationship in people aged 18–64 years and the magnitudes of association decrease with increasing age, in case of more than 13 teeth loss and SAH. SAH may play a role in the increase of IgG level caused by P. Gingivalis, A. Actinomycetemcomitans, P. Intermedia, high-density lipoprotein cholesterol, and CRP, thus causing rapid evolution of the periodontal disease,8,21,25. In contrast, SAH could not have a significant relationship in any of the age strata in 2019, and only CVD had an association in the groups 45–54 years and 65 years or older in 2013 and 2019, respectively, and with weak magnitudes, as these diseases and Periodontitis share risk factors that strengthen a bidirectional theory.21,25
Hypercholesterolemia with neglected self-care, low-grade systemic inflammation, and reduced salivary flow which can consequently lead to tooth loss.9,33 In 2013, hypercholesterolemia was statistically associated with age strata 18–54 years old. However, in 2019, only people aged 35–44 years had a higher prevalence of 13 or more missing teeth. Thus, we observed that the results of 2013 and 2019 were different.9,33
In 2013 and 2019, depression and loss of 13 or more teeth was having a significant relationship in the age groups of 35–44 years, 45–54 years, and 55 and 64 years, and with increasing age, the magnitudes of associations decreased. Psychosocial factors, primarily neglected oral hygiene decrease immune response. The use of antidepressant drugs in such cases also reduces the salivary flow and thus more prone to periodontal bacterial pathogens.13,22,23
Similarly, arthritis/rheumatism with tooth loss was statistically significant in 35–54 years age groups in 2013 and 2019. Arthritis/rheumatism has impaired function of the NF-KB activator receptor signalling axis, osteoprotegerin and NF-KB activator receptor-binding protein. This may cause impaired osteoclast development and activation of mature osteoclasts. 34 This mechanism primarily causes alveolar bone loss and this could explain the observed associations from 35 to 54 years of age. 35
23.9% tooth loss (95% CI: 23.2–24.6) and 21.8% (95% CI: 21.3–22.3) were found in 2013 and 2019, respectively. Previously, in the 2003 and 2010 National Oral Health Survey, tooth loss was seen only in adolescents and adults, while comparing 2013 to 2019, we observed a reduction in all ages. Reduction in this frequency of tooth loss may be due to increased awareness of oral health,14,16,36 easy access to dental services in the last two decades16–18 and water fluoridation and widespread use of fluoridated toothpaste. 12 Until 2013, an accelerated financial expenditure was towards oral health, 17 which gradually reduced from 2013 to 2016 and the large drop in 2018.17,18
The limitation of our study is that it is a cross- sectional study, so we do not have control over temporal factors of exposures and outcome, and the observed associations may not reflect the actual causal relationship, requiring cohort and case-control studies to establish more concrete associations. The use of self-reported information can be considered another limitation of the study, although widely accepted in epidemiological surveillance studies.8,21
Conclusion
In conclusion, studied systemic disorders and more than 13 teeth loss have a good correlation in the Brazilian population in 2013 and 2019. The younger population (35–64 years age group) and older group (≥65 years) showed higher prevalence ratios for tooth loss. The presented systemic conditions are preventable with several available treatments for better control. Therefore, respective stakeholders need to focus on the prevention and control of such systemic diseases and primary dental care aiming at the Brazilian population with chronic and mental illnesses to improve oral health.
Footnotes
Acknowledgements
We are especially grateful to the Postgraduate Program in Public Health at the Federal University of Ceará, where our research was carried out. There was no source of funding for this research. All researchers were volunteers.
Authors Contributions
Erica Nobre Lima and Larissa Fortunato Araújo contributed to the conception, design, data acquisition and interpretation, performed all statistical analyses, drafted and critically revised the manuscript. Caroline contributed to the conception, to data interpretation and drafted and critically revised the manuscript.
Ethical Approval
The 2013 PNS was approved by the National Research Ethics Committee of the National Health Council on June 26, 2013, according to protocol 328,159 and CAAE 10853812.7.0000.0008. The 2019 PNS project was approved by Conep in August 2019, according to protocol 3.529.376 and CAAE 11713319.7.0000.0008. All survey respondents were informed, consulted, and agreed to participate in the interview. More information on ethical approval by the National Health Council of Brazil is available on the website
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.