
Abstract
Aim:
Intraradicular post systems have become an important treatment method for endodontically treated teeth as they provide retention for restoration to the remaining tooth structure. The objective of the present in vitro study was to evaluate the effect of different fiber post-application techniques on the fracture resistance of premolars with flared root canals and no ferrule.
Materials and Methods:
Sixty freshly extracted, single-rooted mandibular premolars with no ferrule were endodontically treated by an experienced endodontist, and their root canals were experimentally flared. The specimens with flared root canals were divided into five groups according to fiber post-application techniques (n = 12): a prefabricated fiber post (G1), G1 + two auxiliary posts (G2), i-TFC post system (G3), G1 + quartz splint (G4), and Ribbond (G5). The data were analyzed with analysis of variance and Tukey tests.
Results:
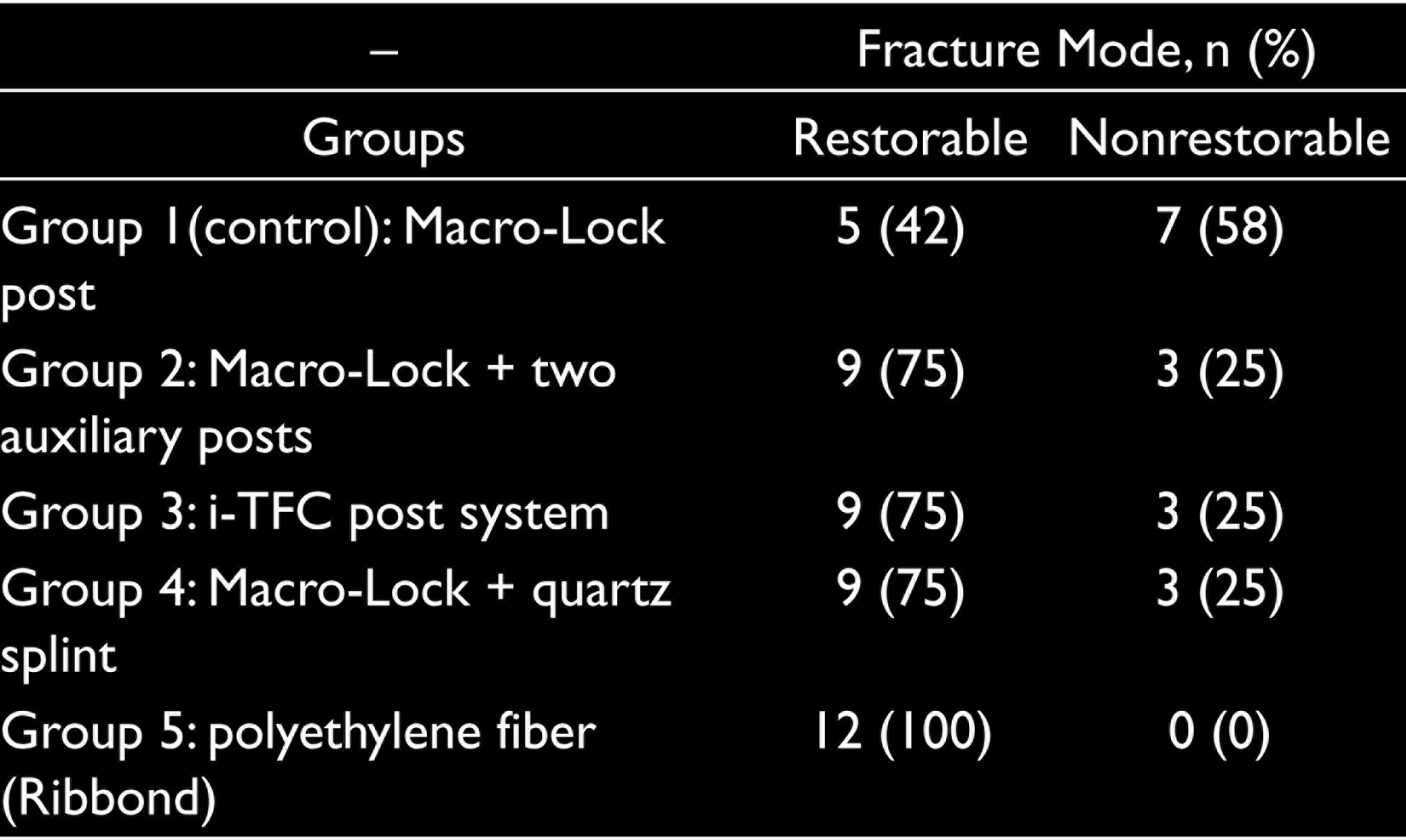
The findings were revealed that no significant difference was found among four groups, except G5 (P > .05), which demonstrated the lowest fracture resistance (P < .05). G2, G3, G4, and G5 exhibited dominantly restorable fracture pattern, whereas G1 exhibited nonrestorable fracture pattern.
Conclusion:
Within the limitations of this study, the placement of auxiliary posts, i-TFC post system, quartz splint placement, and Ribbond increased the incidence of restorable fracture compared with the controls.
Keywords
Introduction
The prognosis of endodontically treated teeth (ETT) depends not only on the success of root canal treatment but also on the success of the coronal restoration.1–4 The restorative procedures for ETT are quite challenging because of the alterations in the mechanical properties of the dentin and require technique sensitivity. 1 Furthermore, the root canal such as access cavity and root canal preparation, 5 extensive carious lesions, previous endodontic treatment, iatrogenic failures, root resorption, and removal of the previously placed posts.6, 7 It is known that the ETT with thin dentinal walls causing stability loss are more prone to fractures reducing the long-term success of the restoration. 8
Intraradicular post systems have become an important treatment method for endodontically treated teeth as they provide retention for restoration to the remaining tooth structure.1, 9 Favorable developments in adhesive dentistry have recently made fiber-reinforced resin posts (fiber post [FP]) more popular because of their advantages such as superior aesthetics and reduction in treatment time. 10 The use of FPs with an elastic modulus similar to dentin to restore the tooth effectively makes the ETT more resistant to fracture. 10 Laboratory and finite element analysis (FEA) studies also revealed that FP can protect remaining tooth structures against extensive fracture loads that can cause catastrophic (nonrestorable) failures.11–13 They facilitate creating a monoblock restoration that acts as a single unit against masticatory forces. 14 It is of great importance to improve the prognosis of ETT with weakened roots facing higher fracture risk by obtaining a better monoblock structure.15–17
The adaptation of the FP to post space may be considered as another factor influencing the prognosis of ETT. Although many FP systems come with size-matched drills provided by the manufacturer to increase the adaptation of the post to the root canal walls, alterations in root canal morphology may disrupt the adaptation.13, 18, 19 Because FPs have a circular cross-section, this adaptation is impaired particularly in root canals with elliptical cross-section and flared root canals because of carious lesions, trauma, or iatrogenic reasons. 18 In these circumstances, the film thickness of luting material changes depending on the root canal morphology 20 and increases at coronal third of the flared root canals, causing adaptation problems.13, 18, 19
Several techniques have recently been introduced to overcome post adaptation problems in flared root canals like Ribbond fibers, auxiliary FP placement along with the main post, prefabricated polyetheretherketone posts, composite resin reinforcement (relining), and anatomical FPs.21–23 Further, there is an alternative FP system (i-TFC; Sun Medical, Shiga, Japan) with sleeves made of braided fibers which can be slide apically or coronally to fit the root canal morphology and provide better adaptation. However, there is no consensus on the ideal post-application technique for restoring ETT with flared root canals, and the variations in the characteristics of these post types do not facilitate the determination of the ideal technique. Accordingly, the present in vitro study aims to evaluate the effect of different FP-application techniques on the fracture resistance of premolars with flared root canals. The null hypotheses were that (a) the post-application technique does not influence fracture resistance of premolars with flared root canals, and (b) the post-application technique does not influence the fracture pattern.
Materials and Methods
Specimen Preparation
This in vitro study with application number 2020/02-17 was approved by the Research and Ethics Committee of the Necmettin Erbakan University (Konya, Turkey). Sixty freshly extracted human single-rooted sound mandibular first premolars of similar size (buccolingually and mesiodistally) and shape with no cracks or caries were obtained. Only teeth with a minimum root length of 16 mm were selected. The width of the roots at the cementoenamel junction (CEJ) was measured using a digital caliper (Model CD-6BS; Mitutoyo, Tokyo, Japan) and recorded as 7.45 ± 0.85 buccolingually and 5.41 ± 0.37 mesiodistally. One-way analysis of variance (ANOVA) was used to analyze the samples, and no significant differences in sample dimensions (P = .75; P = .89, respectively) were found among the groups. The exclusion criteria were the presence of caries, restoration, previous endodontic therapy, or dental anomalies. The sample size (n = 12) was calculated with G* Power software (version 3.1; University of Dusseldorf, Dusseldorf, Germany), with an effect size (d) of 1.4, α of 0.05, and 1-β (power) of 0.80, according to previously published study 20 . Following extraction and cleaning, the teeth were examined using a stereoscopic loupe (EyeMag Pro S; Carl Zeiss, Oberkochen, Germany) to eliminate teeth with microcracks. The teeth were further examined with radiographs to confirm there were no cracks in the teeth. All teeth were stored in 0.1% thymol solution for one week and kept in distilled water to avoid dehydration throughout the experiments at room temperature. For standardization, all samples were fabricated by an experienced endodontist (MA) at Selçuk University (Konya, Turkey).
The crowns of the premolars were removed at the CEJ to eliminate the ferrule effect using a low-speed precision saw (Isomet 1000; Buehler, Lake Bluff, IL, USA) under copious water. For standardization, the root canal length was fixed to a length of 16 mm by removing the apical portion. Residual pulp tissue was taken off with barbed broaches (Dentsply Maillefer, Ballaigues, Switzerland), and the working length was measured using a number 10 K file (TFA; SybronEndo, Glendora, CA, USA) until the tip was seen at the apical foramen. Then, the mechanical instrumentation was performed using Protaper Universal (Dentsply Maillefer, Ballaigues, Switzerland) up to F5 (ISO size 50 with 5% taper) with 2.5% sodium hypochlorite irrigation (NaOCl) using an endodontic syringe (10 mL in total). As final irrigation, the smear layer was removed by 5 mL of 17% EDTA for 3 min, followed by irrigation with a sterile saline solution of 10 mL. After the irrigation, the root canals were dried with paper points (Protaper paper points; Dentsply Maillefer, Ballaigues, Switzerland). Single-cone obturation technique was performed with gutta-percha points (Protaper gutta-percha points; Dentsply Maillefer, Ballaigues, Switzerland), and AH Plus resin (Dentsply De Trey, Konstanz, Germany) was used for the sealing of the root canals. A noneugenol-based temporary filling material (Cavit; 3M ESPE, St. Paul, MN, USA) was applied to provide the coronal seal. After the endodontic treatment, the specimens were kept in 100% relative humidity at 37°C for 24 h. The similarity of the dentinal wall thicknesses was later confirmed with radiographs.
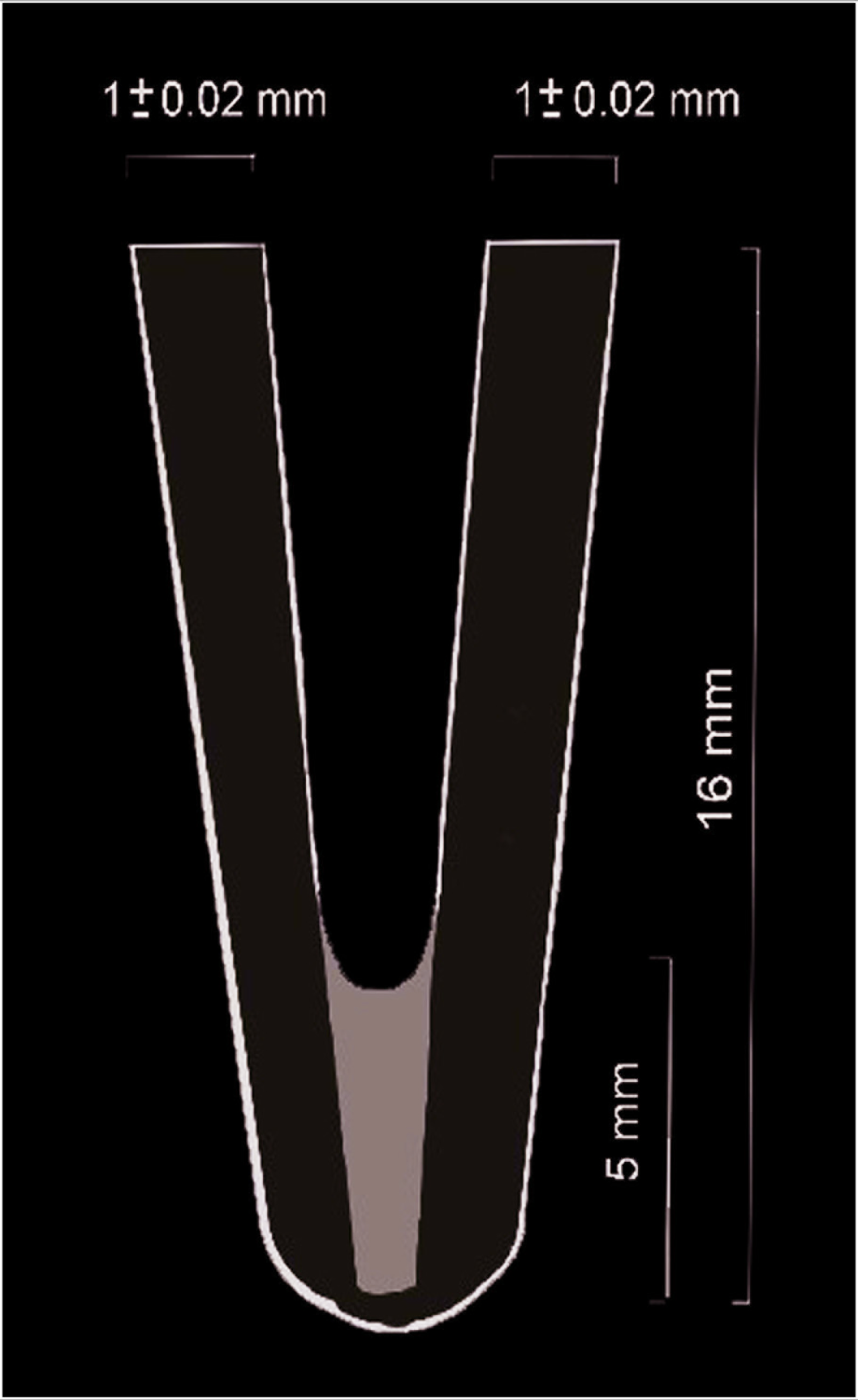
The specimens were mounted vertically in auto polymerizing acrylic resin blocks (Heraeus Kulzer GmbH, Wehrheim, Germany). The temporary filling material was removed by a spoon excavator. A post space with a depth of 10 mm was prepared for all specimens by removal of gutta-percha using Glidden drills with sizes three to five (Dentsply Maillefer, Ballaigues, Switzerland) and electrically heated pluggers (System B; Sybron Dental Specialties, Orange, CA, USA). In order to obtain flared canals, the root canals were enlarged by using high-speed tapered diamond burs (TR-12; MANI Inc, Toshigi-Ken, Japan) under copious water cooling. The peripheral dentin wall thickness was ensured with a digital caliper as 1 ± 0.05 mm at the coronal region (Figure 1). Prior to the luting of FPs, the root canals were cleaned with 2% NaOCl, followed by rinsing with water for 10 s, and dried with paper points.
Schematic Diagram of the Flared Root Canal Prepared for Experiments
Fiber Post Application
The specimens were randomly divided into five experimental groups using a computer algorithm regarding the post-application technique (n = 12).
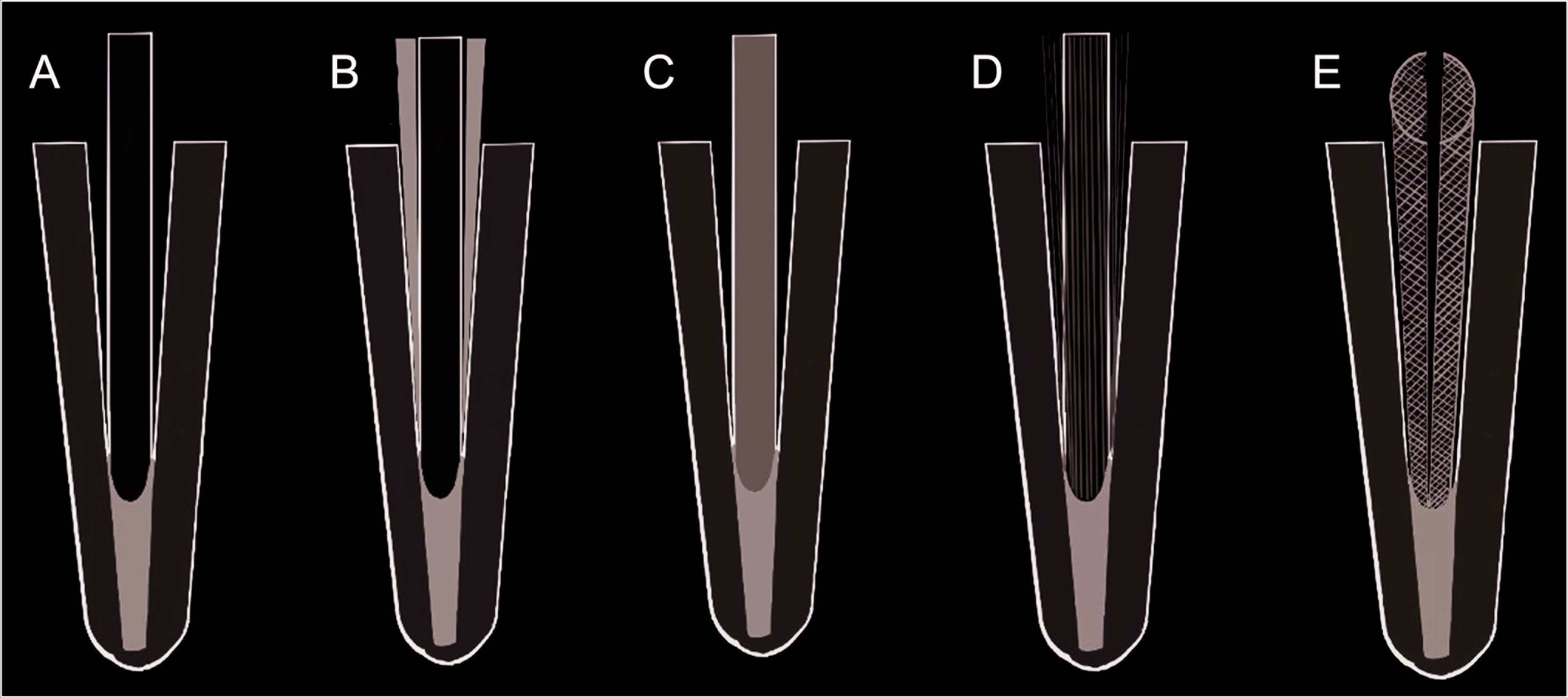
Group 1 (control): A prefabricated FP system with a diameter of 1 mm (Macro-Lock X-RO Illusion; RTD Inc, St. Egreve, France) was used (Figure 2A). It was ensured that all posts were extended the same length (3 mm) from the orifice of the root canal, and the complete seating of the post to its place was checked. Prior to luting, post space was cleaned with ethanol. An auto-mixing, dual-cure luting resin (Clearfil SA Cement; Kuraray, Tokyo, Japan) was injected into the post space via endo tips provided by the manufacturer, and then the posts were gently seated to full depth in the prepared spaces with finger pressure. After removal of excess resin, luting resin light-cured from above the post using a light-curing unit (Bluephase; Ivoclar Vivadent, MV, Schaan, Liechtenstein) for 40 s with a minimum intensity of 700 mW/cm 2 .
Group 2: Same FP in the control group was used as the main post, and two auxiliary FPs with a diameter of 0.4 mm (Fibercone; RTD Inc, St. Egreve, France) were placed into the prepared post space along with the main post (Figure 2B). The posts were luted as in the control group.
Group 3: The i-TFC post system with a diameter of 1.1 mm was used in this group (Figure 2C). The posts and the sleeves were cut to the required length: 10 mm for post space and 3 mm for core, 13 mm in total. Before polymerization, the sleeve was pressed in an apical direction to achieve better fitting to the shape of the flared root canal. After the sleeve was seated, the excess resin was discarded, and the luting resin was cured as in the control group.
Group 4: The Macro-Lock post, which was used in the controls, was used as the main post in combination with quartz splint (Quartz Splint Unidirectional; RTD Inc, St. Egreve, France; Figure 2D). The main post was cut to the required length and seated to full depth in the post space filled with the luting resin and positioned centrally, as in Group 1. Then, the quartz splint was placed around the main post to reduce the film thickness of the luting resin. After that, the excess resin was removed, and the luting resin was cured as in the control group.
Group 5: A polyethylene fiber ribbon-reinforced composite resin (Ribbond; Ribbond Inc., Seattle, WA, USA) was used as an anatomical post. The post space was filled with luting resin, and the Ribbond was inserted full depth into the prepared spaces (Figure 2E). The sleeve was seated following the removal of the resin cement excess with a small brush. After removing excess resin, the luting resin was cured as in the control group.
In the following step, a 4 mm-high core simulating the premolar tooth was formed to ensure the specimens’ uniformity. Following the post application, a composite resin (Filtek Z350 Restorative; 3M ESPE, St. Paul, MN, USA) was incrementally (horizontal increments in 2 mm) placed with a clear matrix band (Super Cap Matrix; Kerr Hawe SA, Bioggio, Switzerland) after universal adhesive (Single Bond Universal; 3M ESPE, St. Paul, MN, USA) application according to the manufacturer’s recommendations. 24 Specimens were stored in distilled water for 24 h.
Study Groups. (A) Group 1, Prefabricated Fiber Post, (B) Group 2, Placement of Auxiliary Posts Along with the Main Post, (C) Group 3, i-TFC Post System, (D) Group 4, Quartz Splint Placement Around the Main Post, (E) Group 5, Polyethylene Fiber (Ribbond) Application as a Custom Post
Fracture resistance testing and fracture mode analysis were performed by another researcher (ANK) who did not participate in sample preparation and blinded to group allocation to prevent any potential bias.
Fracture Resistance Testing
The prepared specimens were positioned on the lower plate of a universal testing machine (Instron, Canton, MA, USA). The occlusal surface of the specimens was subjected to a gradually increasing force until failure (1 mm/min). The force was directed parallel to the longitudinal axis of the post via a steel spherical tip with a 4 mm diameter, which was fixed to the upper plate. No pretest failure occurred. The value of the force causing the fracture was recorded in Newton (N).
Fracture Mode Analysis
The fracture modes of specimens were analyzed using a stereoscopic loupe (EyeMag Pro S; Carl Zeiss, Germany) under 4× magnification and divided into two groups according to the fracture modes: restorable (coronal fracture up to the CEJ level, cervical fracture, or composite core fractures), nonrestorable (coronal fracture below the CEJ level, a vertical fracture extending into the root).25, 26
Statistical Analysis
The data were analyzed using the Kolmogorov–Smirnov and Shapiro–Wilk tests to ensure a normal distribution. For fracture resistance data, one-way ANOVA and the Tukey tests were performed. All tests were analyzed using a statistical program (SPSS v20.0; IBM Inc., Chicago, USA) with the level of significance set at P < .05 and confidence level of 95%.
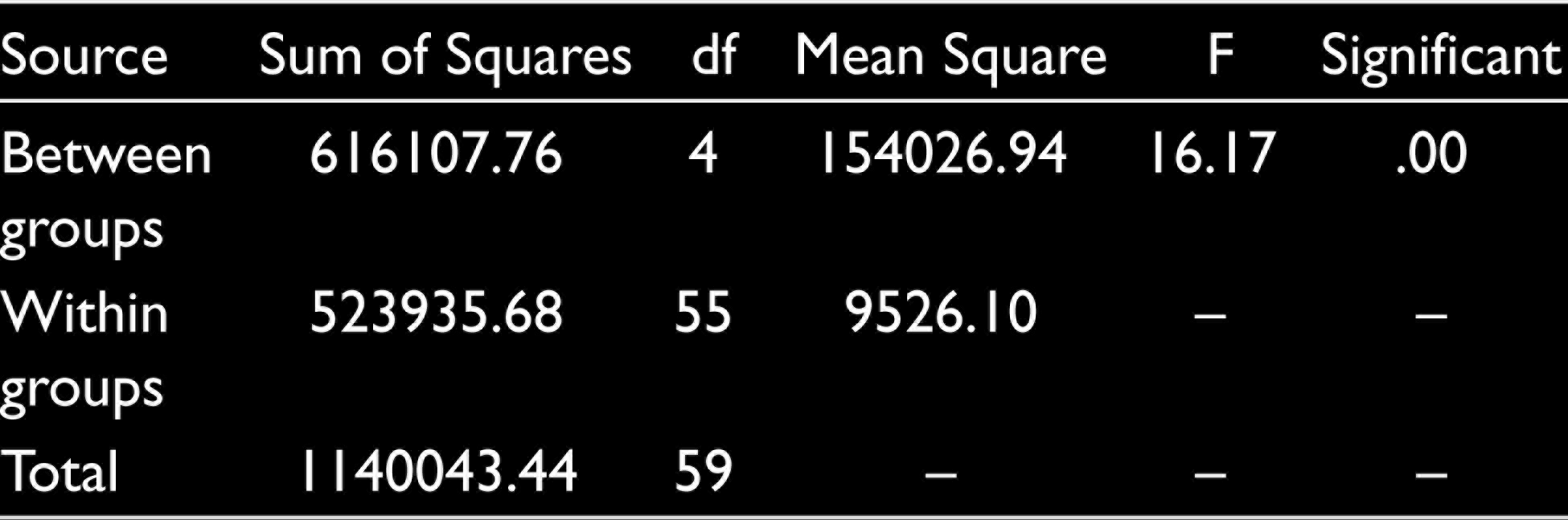
ANOVA Table for Analysis of Failure Loads
Results
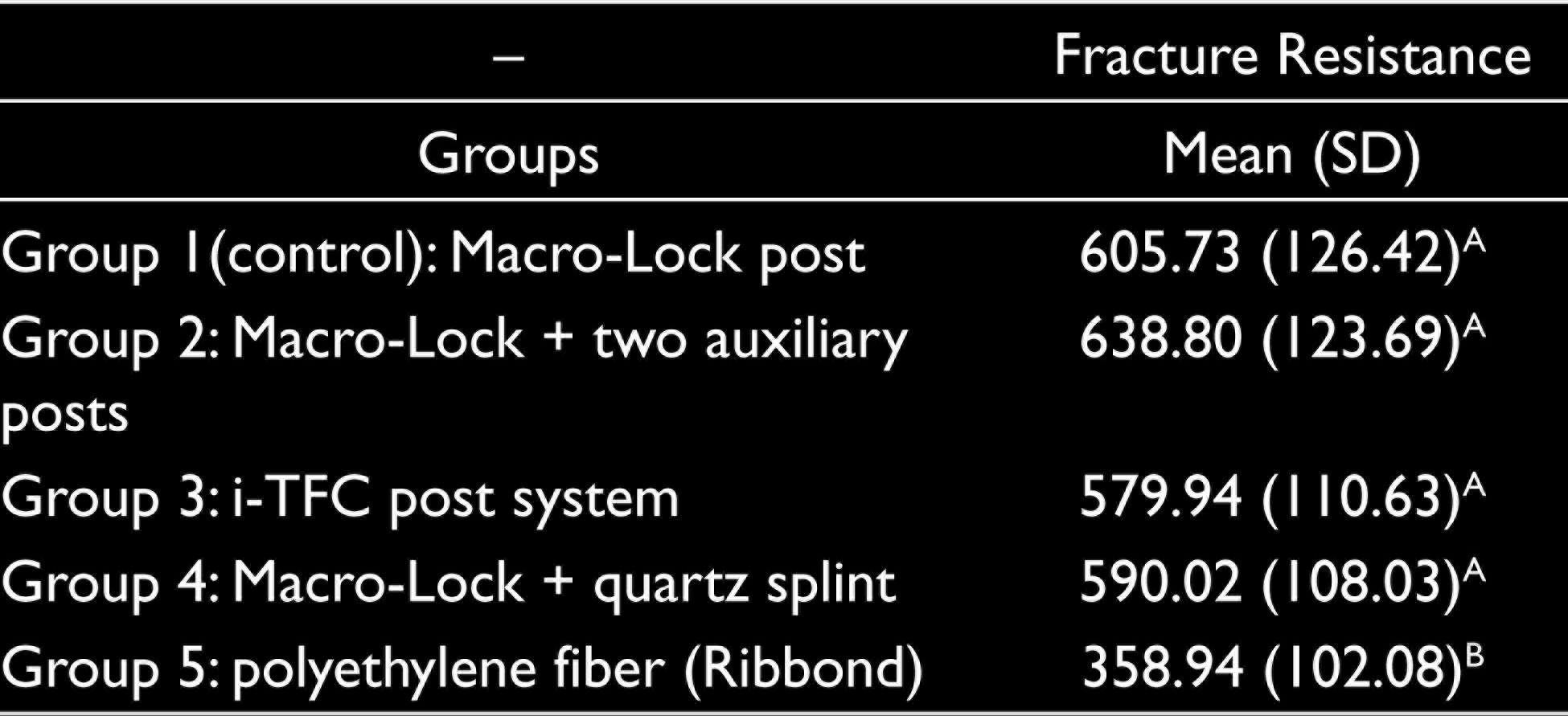
According to the Kolmogorov–Smirnov (P = .10) and Shapiro–Wilk (P = .08) tests, data were normally distributed, and therefore, parametric tests were performed. The ANOVA revealed a significant difference among the test groups (P < .05; Table 1). The mean fracture resistance values (N) with standard deviations and fracture modes after different post-application techniques were presented in Table 2. The lowest fracture resistance was detected in G5, the Ribbond group (P < .05). The placement of auxiliary posts (G2) slightly increased the fracture resistance compared with the control group but was not statistically significant (P > .05). According to the pairwise analysis, no significant difference was found among four groups except G5 regarding the fracture resistance (P > .05). The placement of auxiliary posts along with the main post (G2), the usage of i-TFC post system (G3), quartz splint placement around the main post (G4), and the Ribbond application as a custom post (G5) exhibited dominantly restorable fractures, whereas the controls mostly exhibited a nonrestorable fracture pattern (Table 3). It is noteworthy, despite having the lowest fracture resistance, all specimens of G5 (100%) exhibited a restorable fracture pattern.
Means of Fracture Loads with Standard Deviations (SD) Among the Study Groups
Distribution of Fracture Patterns Among the Study Groups
Discussion
Restoration of root canal treated teeth with wide root canals using post and core systems is still a challenging process as the mismatch between the wide diameter of the flared root canals and standardized rounded diameter of prefabricated post results in a thick cement layer. Furthermore, the restoration of these flared root canals may be a compromised treatment as the remaining tooth structure is too weak to tolerate the normal masticatory forces, and as a consequence, the teeth are liable to fractures. 27 The purpose of the present investigation was to evaluate the effect of different FP-application techniques on the fracture resistance of the premolars with flared root canals. The placement of auxiliary posts along with the main one (G2), the usage of i-TFC post system (G3), quartz splint placement around the main post (G4), and Ribbond application as a custom post (G5) did not create an advantage in terms of fracture resistance compared with the controls (G1); moreover, the Ribbond group exhibited the lowest fracture resistance. Therefore, the first null hypothesis that the post-application technique does not influence fracture resistance of premolars with flared root canals was rejected.
FP systems are extensively preferred to restore ETT because these FPs have an elastic modulus similar to the root dentin and produce monoblock restoration, resulting reinforcement in structurally compromised roots such as flared ones.8–11 The self-adhesive resin cement does not require any pretreatment of the tooth surface. Once the cement is mixed, its application steps are quite simple. Therefore, self-adhesive resin cement is often preferred for luting FPs and indirect restorations.19, 20, 28 However, the morphological differences in the root canal and radicular dentin must be considered. The high C-factor in root canals can cause higher polymerization shrinkage stress, decreasing the bond strength. 29 Furthermore, several studies stated that poor adaptation of the post to its space is likely to form air bubbles and voids that could result in displacement and failure.18, 26 Formation of these air bubbles and voids would be less probable if the film thickness of the luting resin was thinner and more uniform. Moreover, the development of the polymerization shrinkage stresses would be minimal in reduced film thickness. Xiong et al. 9 reported that the fracture resistance increased when the post was well adapted to the root canal walls of ETT. For this reason, application of custom posts or multi-post technique would positively affect the long-term prognosis of the restored ETT by increasing the post adaptation. According to Maceri et al., 29 the placement of auxiliary posts along with the main post (multi-post technique) would provide more successful filling of root canals with irregular morphology compared with the single post placement.
Various studies on the multi-post technique reach different results. Li et al. 30 stated that the combination of the main post with auxiliary FPs increased the fracture resistance of maxillary central incisors with flared root canals. They placed two or five auxiliary posts along with the main one and found increased fracture strength compared with the control group. Similarly, Fráter et al. 25 also reported that auxiliary post placement increased the fracture resistance of maxillary premolar teeth compared with single post application. On the contrary, in the present study, although using the multi-post technique provided a slight increase in fracture resistance compared with the control group, it did not create a statistically significant difference. Aggarwal et al. 26 examined the effect of the multi-post technique on the fracture resistance of mandibulary premolar teeth and reported that the multi-post technique did not provide an advantage over the single post application, which is consistent with the present study. The reason for these variations between studies can be attributed to being related to differences such as experimental design, luting material choice, and tooth selection. Similarly, no difference was found among the fracture resistance of specimens restored using the i-TFC post system and Groups 1, 2, and 4. According to the manufacturer’s data, the i-TFC post system has flexural strength and flexural elasticity characteristics almost identical to the dentin. It is reported that this feature is because of the fibers being braided similarly to the collagen network structure of the dentin. The findings of the present study confirm the previous study that the i-TFC system can be an alternative to the other post techniques in flared root canals with its ease of application. 24
In Groups 4 and 5, the post was formed with the aid of a fiber splint (Quartz Splint UD) and a polyethylene fiber ribbon-reinforced resin composite (Ribbond), respectively, and theoretically, post applications in these two groups can be considered as a custom post. 26 As with the multi-post technique, it can be thought that coiling the main post with quartz splint or forming an anatomical post with Ribbond would reduce the film thickness of the luting resin in the flared root canals, creating less polymerization shrinkage stress and providing a better adaptation. However, in the findings of the present study, placement of quartz splint around the main post did not improve the fracture resistance compared with the controls. A custom post can be created in accordance with root canal morphology by condensing woven fibers (Ribbond) into the post space. 26 Although the lowest fracture resistance was observed for Group 5, all specimens in this group exhibited restorable fractures, in accordance with the previous study. 26
The most common causes of failure in restored ETT are post fractures and fracture of the tooth itself.26, 31 Along with the fracture resistance, fracture pattern is also important in restoring the ETT after the fracture. Fractures above the CEJ can be treated with no problem; however, ETT that are fractured in a nonrestorable way (fractures below the CEJ, vertical fractures extending into the root) usually result in extraction. In the present study, placement of auxiliary posts, the i-TFC post system, coiling quartz splint around the post, and Ribbond as a custom post increased the incidence of restorable fractures, while the control group mainly exhibited nonrestorable fracture pattern. This finding is consistent with the previous studies.24, 29 Therefore, the second null hypothesis that the post-application technique does not influence the fracture pattern of premolars with flared root canals was rejected. Maceri et al. 29 stated that the multi-post technique decreases the incidence of nonrestorable fractures in line with the present study. On the contrary, Fráter et al. 25 concluded that post technique did not influence the fracture patterns.
Long-term prognosis of ETT depends primarily on the remaining tooth structure. Teeth with extensive tooth loss have reduced capacity to resist masticatory forces, and a post is essential to hold an artificial core that will restore the tooth.1, 32, 33 Dental practitioners believed that a post would reinforce the remaining tooth structure; 34 however, the volume of dentin remaining is of most relevance to tooth strength.9, 27 During post space preparation procedure, it is recommended that the remaining dentin should be preserved as much as possible. Resistance to fracture of ETT depends on the remaining root dentin thickness, especially in the buccolingual direction. 35 The cervical part of the root canal can be left overprepared and surrounded only by a thin dentinal wall. In addition, overpreparation of the root canal reduces fracture resistance as a result of extensive caries and recurrent caries.27, 36 Vertical root fracture of ETT with flared root canals represents a clinical dilemma, although the use of FPs has improved the prognosis. 37
The cervical band of a crown that encircles the parallel walls of the dentine extending coronally to the shoulder of the preparation is defined as a ferrule. The ferrule effect has been suggested to improve the integrity of the ETT with cast post-core. 38 However, in a more recent study, no benefit was reported with the additional ferrule preparation for a FP, composite core buildup, and composite crown in fracture resistance. 39 Contrary to the ETT with compromised structural conditions such as flared root canals, the use of a ferrule provides no additional benefit for fracture resistance. 40 Besides, it is often hard to find axial cervical tooth structure in flared root canals to be used for an efficient ferrule effect. 41 Thus, in this in vitro study, the specimens were prepared with no ferrule to achieve compromised tooth structure.
In the present in vitro study, different post-placement combinations were compared to reduce the polymerization stresses by decreasing the cement thickness. However, the auxiliary posts (G2) or Quartz Splint UD post (G4) groups, which had a thinner cement layer than the Macro-Lock group (G1), did not give an advantage regarding the fracture resistance (P > 0.05). Moreover, in previous research, 24 there was no significant difference between the fracture resistance of the i-TFC system and that of the other post systems (auxiliary posts and indirect anatomic post placements), supporting the findings of our study. The main limitation of the present in vitro study is that it was conducted without an artificial aging and cycling loading process simulating the clinical use. In terms of durability, the post-application techniques used in the present study could be performed after an artificial aging and a cyclic loading process to simulate clinical scenario better. Additionally, it would be beneficial to include a control group without a post placement to better determine whether post systems increase fracture resistance. The fracture failure strength could not fully reveal the clinical status of ETT. Durability should be taken into consideration for future studies on the investigation of post placement techniques.
Conclusion
This study demonstrated the effect of different post-application techniques on the fracture resistance of premolars with flared root canals. Within the limitations of the present study, it can be concluded that different post placement techniques did not increase the fracture resistance of endodontically treated weakened roots. However, it can be claimed that the placement of auxiliary posts along with the main post, the usage of i-TFC post system, coiling of quartz splint around the main post, and Ribbond as a custom post tend to increase the incidence of restorable fracture.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.