
Abstract
Aim:
Bruxism is defined as the involuntary recurrent masticatory muscle activity characterized by gnashing, grinding, clenching of teeth, and/or pushing the mandible. Factors creating its etiology are peripheral (morphological) or central (physiopathological and physiological), and exogenous. Recently, among physiological factors, depression and bruxism were considered to be related. A definitive treatment method does not exist for bruxism; however, botulinum toxin-A (BT-A) application is an up-to-date and effective way of treatment. The present study is aimed to evaluate the levels of depression in bruxism patients treated with BT-A application.
Materials and Methods:
A total of 25 individuals (23 females and 2 males) who were diagnosed as bruxism patients were included in the study. 25 U of BT-A for each masseter muscle was injected into the patients. Patients were prospectively observed for a possible change in depression levels by using Beck’s Depression Inventory. The inventory was implemented before and six months after the BT-A application. Depression levels before and six months after the injection were compared. A paired t-test was used to compare “before” and “after” treatment values. One-way analysis of variance and post-hoc Tukey tests were used to evaluate the change in Beck’s Depression Inventory scores according to age groups.
Results:
The mean total score was 7.80 ± 8.10 before the treatment and 7.16 ± 6.52 six months after the treatment. The decrease in the mean score was not statistically significant (P > .05).
Conclusion:
In conclusion, despite the decrease in the mean Beck’s Depression Inventory scores, a statistically significant decrease in the depression levels of patients was not observed.
Introduction
Bruxism is defined as the involuntary recurrent masticatory muscle activity characterized by gnashing, grinding, or clenching of teeth and/or pushing mandible. 1 The epidemiology of bruxism is not clear because of different diagnosis strategies and the studies conducted in various populations.2,3 The prevalence of “bruxism” was stated as 8% to 31.4% in general. 4
It was suggested that the etiology of bruxism might be multifactorial, and psychosocial, physiological, and exogenous factors may affect the occurrence of bruxism. 5 Bruxism is considered to have two different forms as “awake bruxism” and “sleep bruxism” with different etiologies. It was shown that awake bruxism may result from anxiety or psychosocial disorders. 6 A series of studies have stated the relationship between bruxism and personality, psychosocial factors, and anxiety. 7 The relationship between the occurrence of bruxism, anxiety, and depression symptoms was shown by Gungormuş et al. The outcomes of anxiety and depression were higher in the individuals with bruxism. 8
There is not a definitive diagnosis method for bruxism. However, polysomnography (PSG) is considered the golden standard. Among some of the other methods used are electromyography, self-reporting by the patient, and clinical examination. A new system for grading bruxism evaluations was introduced by Lobbezoo et al. in 2018. The suggested grading system is as follows: (a) Possible sleep/awake bruxism is based on a positive self-report only. (b) Probable sleep/awake bruxism is based on a positive clinical inspection, with or without a positive self-report. (c) Definite sleep/awake bruxism is based on a positive instrumental assessment with PSG and ecological momentary assessment/experience sampling methodology, with or without a positive self-report and/or a positive clinical inspection. 9
Bruxism may be hazardous for stomatognathic structures. 10 Pathologies considered to be caused by bruxism are abrasion of teeth, hypersensitivity or pain, mobility, cracks, problems observed in dental restorations, implants, and dentures.11–14 Besides, hypertrophy in masticatory muscles, fatigue and pain, and temporary or chronic headaches may also be seen. 15 Although it is not possible to state a direct temporomandibular dysfunction caused by bruxism, it may be indicated that it exacerbates symptoms like pain and locking of the temporomandibular joint.16–19
A consensus has not been established for the treatment of bruxism. Occlusal appliances, pharmacological treatments, behavioral therapy, and some other approaches are used in the management of bruxism. In recent years, it was stated that botulinum toxin (BT) could be used in the treatment of bruxism and the outcomes are promising. 20
Bruxism is also related to specific personality characteristics, especially high levels of anxiety and stress might be a risk factor for bruxism because of their probable effect on the quality of sleep.21,22 Studies have stated relationships between bruxism and anxiety, emotional stress, depression, and hostility in both human and animal studies.23–25 Some pathological emotional experiences result in parafunctional habits more often. It was proved that compulsive, controlling, and aggressive people are more vulnerable to developing bruxism. 26
In general, studies are conducted to evaluate the effect of stress on bruxism. The aim of the present study is to compare the depression levels of patients treated with botulinum toxin-A (BT-A) injections for bruxism-induced masseter muscle hypertrophy before and after the treatment.
Materials and Methods
Study Design
Patient Selection
This prospective observational study was approved by the Ethical Committee of Ankara University, Faculty of Dentistry. A total of 38 patients who applied to the Ankara University Faculty of Dentistry Hospital with teeth grinding complaints and diagnosed as probable bruxism according to self-report and clinical inspection were planned to deliver BT-A injection into masseter muscle at the Department of Periodontology and included in the study. Phase 1 therapy of all patients was completed before they applied for BT-A treatment. The planned BT-A injection was aimed to eliminate the muscle hypertrophy and/or the treatment of connected temporomandibular dysfunction.
The inclusion criteria were as follows: patients older than 18 years of age, patients with masseter muscle hypertrophy, patients with temporomandibular joint dysfunction resulting from muscle function, patients who were scheduled to receive intramuscular BT-A injection application for the treatment of muscle hypertrophy, and patients who signed informed consent to be included in the study.
The exclusion criteria included the following: Patients with advanced periodontal diseases, masseter muscle or parotid gland pathologies; previous parotid gland operation, benign/malignant tumors of the mandible, temporomandibular joint dysfunction other than muscle function; pregnant and breastfeeding women; and patients allergic to the components of BT-A.
Scales Applied
Demographic data was recorded, and Beck’s Depression Inventory (BDI) was applied to the included individuals to determine the depression levels before the study. 8 Inventory was re-applied six months after BT-A treatment. To determine bruxism, the Fonseca Anamnestic Index was used. 27 BDI is a questionnaire consisting of 21 items that assesses cognitive, behavioral, affective, and somatic components of depression. 28 Each answer is scored on a scale value between 0 and 3. Higher scores represent more reported depression and the highest possible score is 63. A score from 1 to 10 reflects that a person is not depressed (normal), 11 to 16 indicates mild mood disorder, 17 to 20 borderline clinical depression, 21 to 30 moderate depression, 31 to 40 severe, and 41 to 63 extremely depressive disorder. The inventory is a simple and comprehensible screening tool.
Treatment Protocol
All patients were informed about the possible side effects of BT-A injections, and signed informed consent forms were collected before the procedure. For each dose of 1.0 U/0.1 mL injection, 100 U frozen dried BT-A (Botox, Allergan, Inc., Irvine, CA) was diluted with 2 cc of saline solution and injected via 30 gauge injector. Three points were marked for the injection of the masseter muscle. All injections were prosecuted by the same periodontologist. A total of 50 U of BT, 25 U for each masseter, was applied. Patients were prospectively observed for a possible change in depression levels by using BDI. Patients were scheduled for follow-up appointments at 15 days, three months, and six months after the application.
Statistical Analysis
The level of significance was taken as 5% and the data were analyzed with SPSS (IBM SPSS for Windows, version 25) package. To define the relationships between the parameters, Pearson’s correlation coefficients were used. A paired t-test was used to compare “before” and “after” treatment values. One-way analysis of variance and post-hoc Tukey tests were used to evaluate the change in BDI scores before and after the treatment according to age groups.
Results
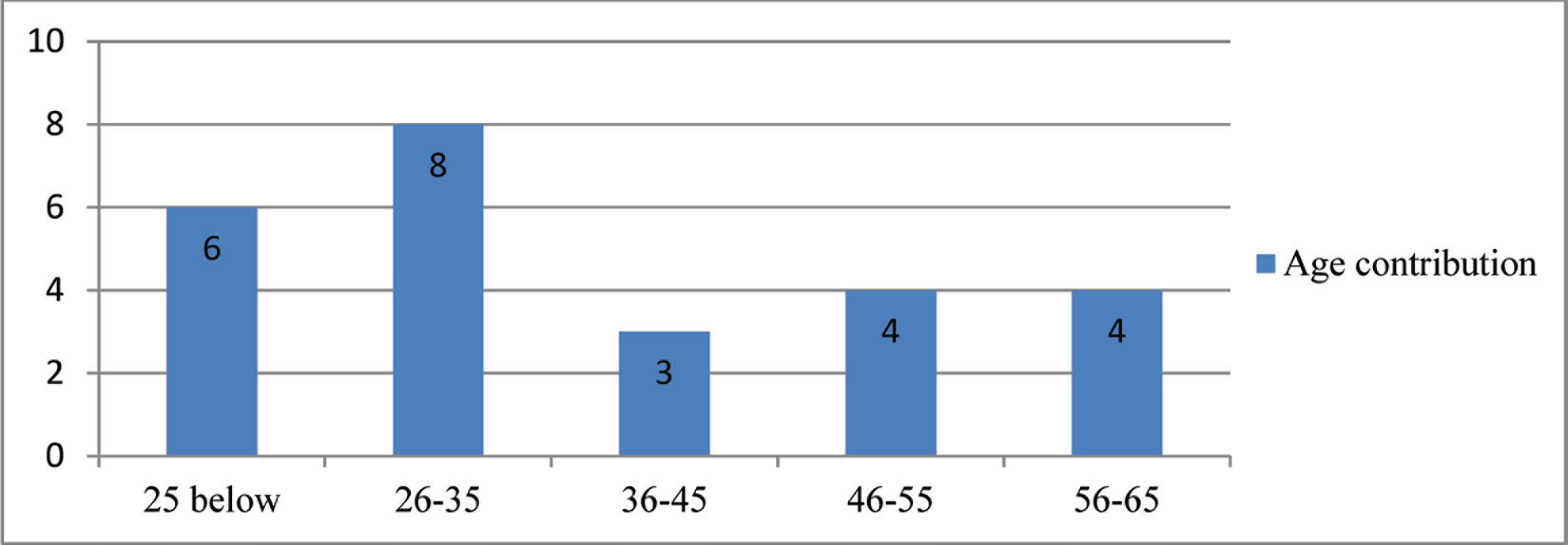
At the beginning of the study, 38 patients were included; however, as a result of the exclusion of noncompliant patients, the study was concluded with 25 patients (2 males and 23 females). The age of the patients ranged between 20 and 65 years, and the mean age was 32.25 ± 10.01 years (Figure 1).
Age Distribution of the Patients Included in the Study
According to BDI applied before the treatment, 19 individuals were considered normal, 3 presented with mild depression, and 3 with moderate depression. The results of the same inventory application six months after the treatment showed that 18 individuals were normal, 4 had mild depression, 2 were borderline, and 1 had moderate depression (Figure 2).
Classification of Patients According to the Beck’s Depression Inventory
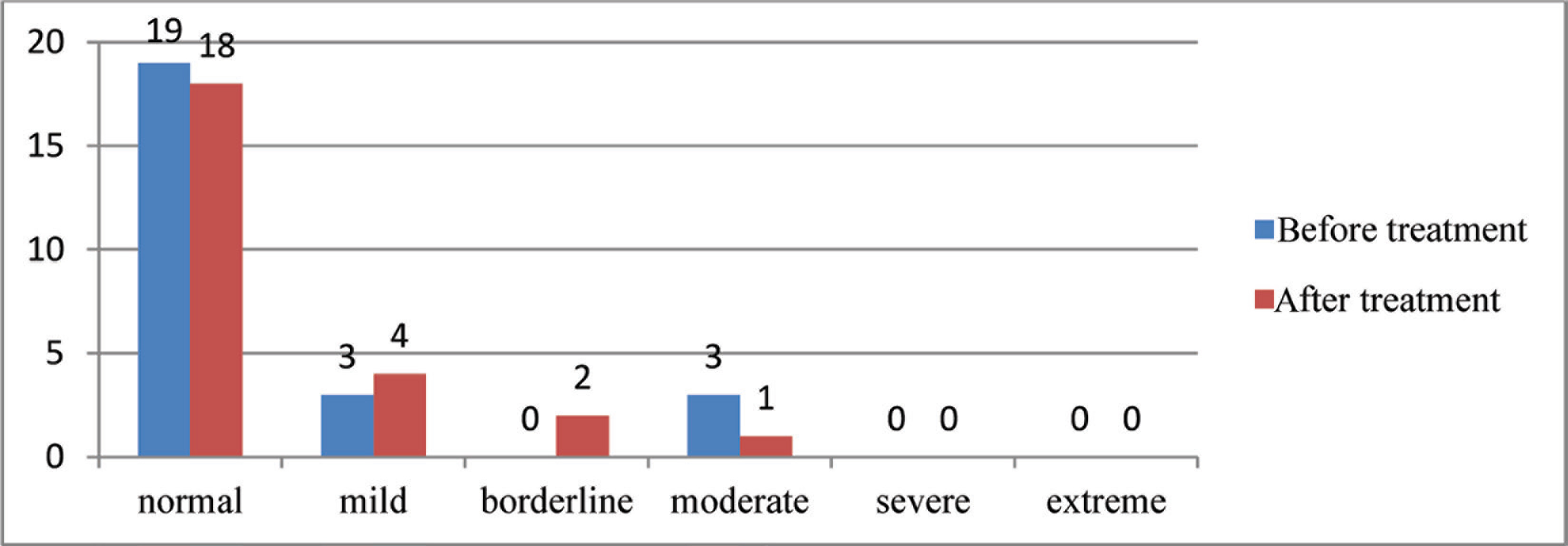
The mean BDI scores with the comparisons between before and after treatment values are presented in Figure 2. The mean BDI score was 7.80 ± 8.10 before the treatment and 7.16 ± 6.52 after the treatment. The decrease in the mean score was not statistically significant (P > .05; Table 1).
The Levels of Significance Between Total Beck’s Scores Before and After Treatment According to Paired t-Test

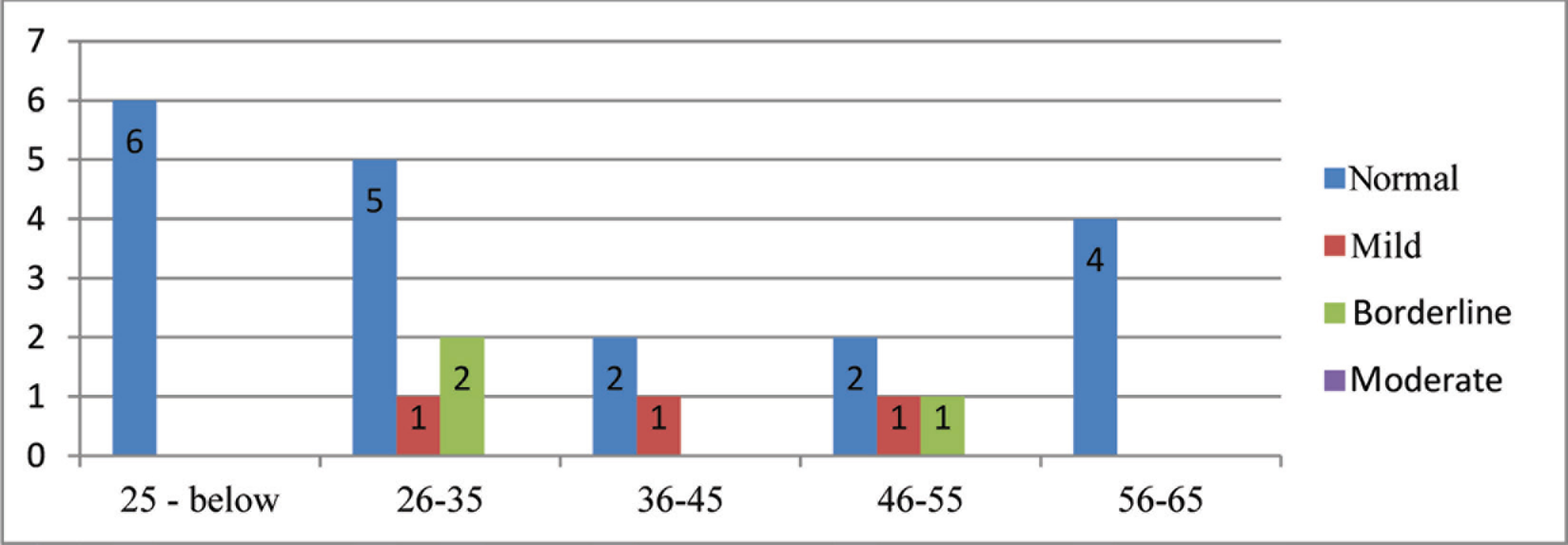
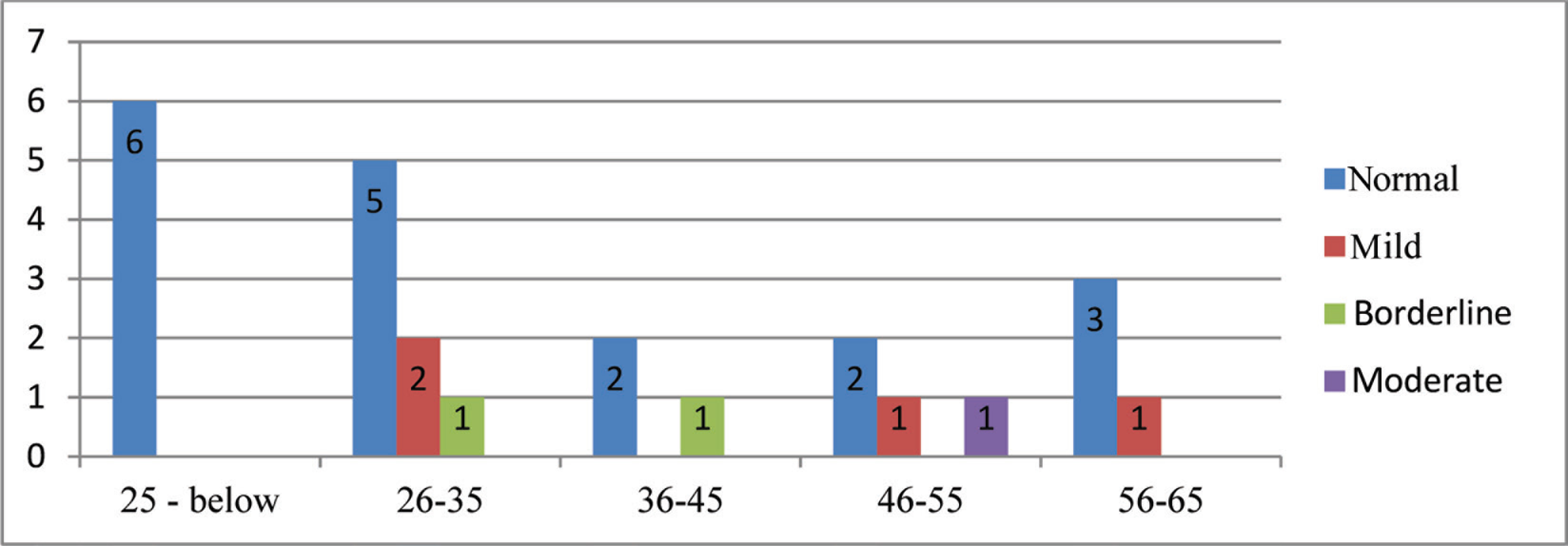
The mean BDI scores of before and after the treatment between age groups are presented in Figures 3 and 4, respectively. No statistically significant difference was found between age groups when the change in BDI scores before and after the treatment was evaluated (P > .05).
The Mean Beck’s Depression Inventory Scores of Patients Before Treatment Between Age Groups
The Mean Beck’s Depression Inventory Scores of Patients After Treatment Between Age Groups
Discussion
Modern life has brought along stress in these times. The prevalence of bruxism has increased with the development of civilization and the modern lifestyle. 29 Many studies regarding the relationship between bruxism and depression were conducted earlier. The relationship between the occurrence of bruxism and depression is still considered controversial because it has not yet been proved scientifically that depression exacerbates the severity of bruxism. In addition to that, some scientists stated that depressive symptoms are observed more often and severely in patients with bruxism.30,31 In a study regarding the relationship between anxiety, depression, and bruxism by Gungormuş et al., the outcomes of anxiety and depression were higher in the individuals with bruxism than the ones who did not have bruxism. 8
There is a strong correlation between temporomandibular disorders (TMDs) and bruxism. In a study conducted by Camparis et al., in a group of patients with sleep bruxism accompanied with or without TMD, a statistically significant difference was detected for physical symptoms. However, there were no significant differences in depression levels. 32 In another study, however, the comparison between patients with and without bruxism showed higher mean anxiety and depression scores. 8 Likewise, Manfredini et al. reported that individuals with bruxism were more depressive and anxious than the ones who did not have bruxism. 23 In a study by Molina et al., individuals with bruxism were shown to have higher levels of hostility than the ones without bruxism. 24 It was stated that experimentally triggered emotional stress induces brux-like activity more than the control group in a study conducted with rats. 25 Some pathological emotional experiences result in parafunctional habits and bruxism more often. It was proved that compulsive, controlling, and aggressive people are more vulnerable to developing bruxism. 26 Fernandes et al. showed that bruxism is a risk factor for pain-related TMDs which indirectly puts the patient at risk for depressive and nonspecific psychological symptoms, and yet the casual relationship between bruxism and depression could not be verified definitely. 31 In a study conducted among patients with pain from TMD, following the treatment with BT-A, a declination in the pain scores and an improvement in mood were observed. 33 Despite the decrease in the depression and anxiety scores of the patients treated for bruxism, we found that this difference was not statistically significant in our study. Although the outcomes comply with previous study results, the insignificance is considered a result of our small study population.
Generally, studies conducted are inclined to evaluate the effect of stress on bruxism. However, the alteration of depression resulting from treated bruxism has not yet been investigated. Our study is a pioneer regarding that matter. The limitation of our study was the lack of psychological support during the BT-A application for the treatment of bruxism. Our approach was to eliminate the physiological effects of bruxism. However, considering that stress is an important factor in the etiology of bruxism depending on the literature, it might be beneficial to include psychological support in the treatment protocol. Further research is needed to evaluate the relationship between stress and bruxism from this point of view.
Consequently, it is considered that different etiologies exist for awake and sleep bruxism which are various circadian rhythmic types of bruxism. It was suggested that the etiology of bruxism might be multifactorial, and psychosocial (i.e., stress and anxiety), physiological (i.e., genetics), and exogenous (i.e., alcohol consumption, smoking, medications) factors may affect the occurrence of bruxism. 5 Psychosocial factors are stated to be more effective in awake bruxism. 6 Bruxism diagnosis was established based on self-report and clinical examination in our study, but the golden standard of bruxism diagnosis that is PSG was not used. Hence, a distinction between sleep and awake bruxism could not be made. Further case-control studies with larger populations that differentiate sleep and awake bruxism should be conducted. Also, further studies should contain healthy individuals without bruxism to observe the changes of depression levels in normal population.
Conclusion
The scores of BDI, which evaluates the depression levels of bruxism patients treated with BT-A, decreased after the treatment compared to the beginning. However, the difference was not statistically significant. Treatments applied to eliminate the physiological impacts of bruxism are effective in reducing stress or anxiety, but are not adequate. The treatment of bruxism should be considered multidisciplinary, and the effectiveness should be increased by planning combined therapies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.