
Abstract
Aim:
To evaluate the effect of leaving excess adhesive around orthodontic brackets on the shear bond strength and on the enamel–adhesive interface characteristics.
Materials and Methods:
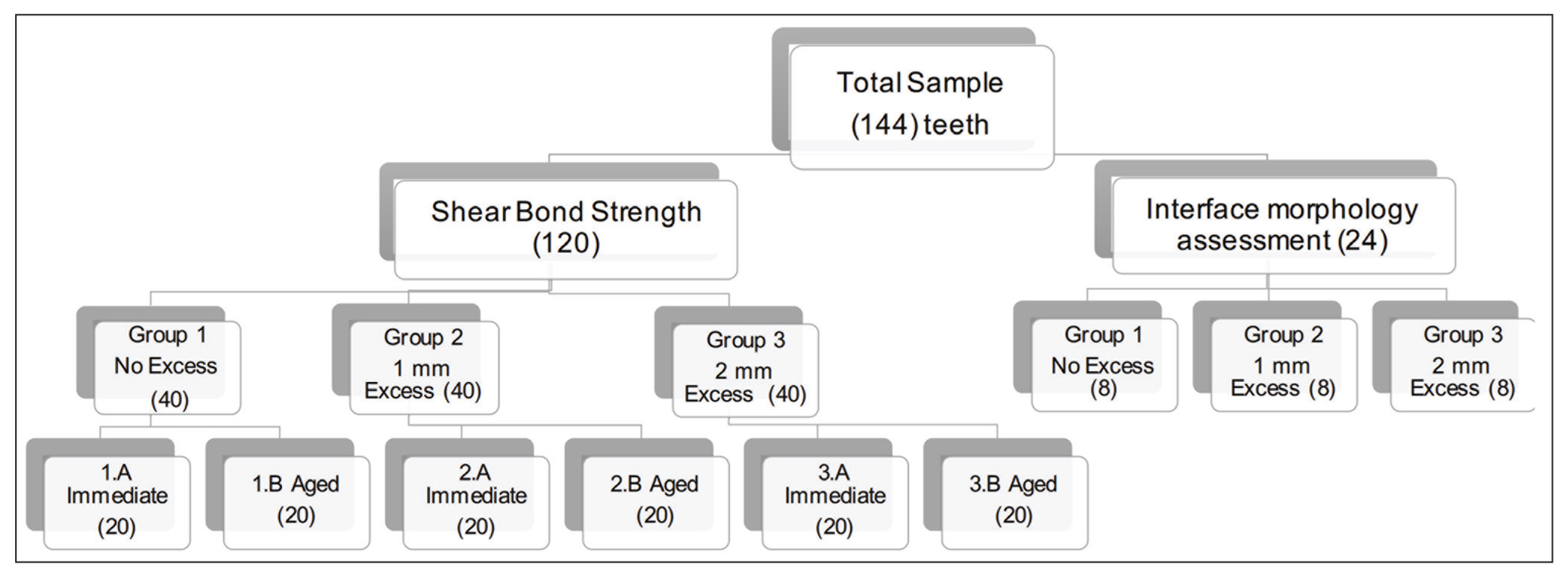
One hundred forty four human premolars were randomly divided into two groups according to the test performed. For the shear bond strength, 120 teeth were bonded with stainless steel orthodontic brackets using Transbond XT light cure adhesive composites. After positioning the bracket and before light curing, excess adhesive was removed according to the test group: group 1, all excess adhesive was removed (0 mm excess); group 2, 1 mm excess adhesive was left; group 3, 2 mm excess adhesive was left; shear bond strength was measured immediately and after three months of natural aging using a universal testing machine; and adhesive remnant index scores were also evaluated. For the enamel–adhesive interface characteristics, 24 teeth were bonded with stainless steel orthodontic brackets using Transbond XT light cure adhesive composites mixed with Rhodamine B fluorescent dye, excess adhesive was removed in the same manner according to the test groups, and teeth were evaluated using confocal laser scanning microscopy.
Results:
Time did not significantly affect the bond strength results (P = .888) but the amount of excess adhesive significantly affected the results (P < .05). Interaction terms were not significant (P = .337). In both immediate and aged conditions, group 1 (0 mm excess) presented the highest bond strength results (MPa; P < .05). No significant difference was found in adhesive remnant index scores or enamel–adhesive interface characteristics.
Conclusion:
Excess adhesive around orthodontic bracket does not increase shear bond strength.
Introduction
Bond strength of orthodontic brackets to tooth surfaces is a primary factor in achieving satisfactory orthodontic treatment. Bonded orthodontic attachments must resist the multiaxial/mechanical forces occurring as a consequence of treatment, as well as those produced by normal mastication and occlusion. 1 As the product of these and other sources of stress in orthodontics varies in magnitude and direction over time, the adhesive interface often becomes a focal point where they are concentrated. A failure of the bond under these shifting forces can have consequences for the outcome of the entire treatment.
The introduction of acid etch technique by Buonocore 2 in adhesive dentistry led to the development of direct bonding of orthodontic brackets by Newman in 1965, 3 which is now considered to be the most popular bonding system in orthodontics. The technique consists of the application of a bonding agent, often an unfilled resin, between the bracket and an enamel surface which has previously been prepared with an etching compound to roughen it superficially. This is followed by the application of a filled composite resin paste at the bracket base. Careful positioning of the bracket on the prepared surface by the clinician, along with firm pressure perpendicular to the plane of the enamel across its whole length results in good bond strength, with a minimal amount of material to remove on debonding, and optimal adhesive penetration into the bracket base. By maintaining even pressure over the bracket at this stage, any excess adhesive is typically forced out of the bonding zone and is readily removed before light curing. 4
Despite the advances in bonding materials and improvements in technique, bond failure is still a common event. Various approaches to decrease the bond failure rate have been introduced, including the use of new adhesive materials, refinement of bracket base designs, minimizing the number of spots in the interface between the bracket base and the prepared enamel where an adhesive might fail to continuously penetrate that space, creating tiny fracture-prone voids, through modifications to enamel etching procedures, or the replacement of chemical etching with sandblasting techniques, and the strengthening of the resins themselves through the addition of adhesion promoters. 5 With any and all of these methods, bond failures still occur and all of them have their own associated particular disadvantages. Similarly, all similar efforts involve adding an extra step to bonding, necessarily thereby increasing the complexity of an already technique-sensitive procedure; plus, in numerous cases the technical requirements for the successful execution of this sort of added work intended to reduce the base rate of bonding failures have been reported to raise issues of incompatibility. Without some radical change in the technology underlying this class of orthodontic procedures, and while acknowledging that incremental improvements in adhesive bonding of brackets to teeth will likely arise, the exigencies of actually accomplishing the basic task of achieving the required tooth movement, may simply force us to accept a certain rate of spontaneous bonding failures. This in turn suggests that developing methods of clinical practice which optimize the results achievable with the existing technical means may be the best real-world path for research to pursue.
It is not uncommon in a clinic to leave some amount of excess adhesive around the bracket upon bonding. 6 Whether left intentionally or accidentally, the excess adhesive often gets overlooked by orthodontists. It is believed that this excess adhesive may cause gingival irritation if it is located at close proximity to the gingival margin. 7 In addition, the potentially rough surface of composite on the tooth may provide an environment that favors bacterial colonization, thereby creating the potential increase of white spot lesions. 8 On the other hand, it is thought that leaving a slight bit of excess adhesive might be advantageous to ensure that the adhesive will be evenly distributed under the bracket so as to mitigate the possibility of any remaining voids. 9 Furthermore, it has been found that leaving some excess adhesive may prevent adhesive washout, thus protecting the tooth against white spot lesions and potentially benefiting the bracket bond strength. 10 It is not yet known whether the reported better retention of the adhesive material beneath the bracket benefits the bond strength or whether the increased surface area of the bracket by leaving excess adhesive increases the bond strength. As far as we know, the effect of leaving excess adhesive around orthodontic brackets on the bond strength has not been investigated. The aim of this study, then, was three-fold: to evaluate the effect of leaving different amount of excess adhesive resin around orthodontic bracket on shear bond strength (SBS) and the failure mode of orthodontic brackets, and for the consideration of the characteristics of enamel–adhesive interface through the use of confocal laser scanning microscopy (CFLSM).
Materials and Methods
Sample Preparation
One hundred forty four human premolars were extracted for orthodontic reasons and informed consent was obtained for their use in this study. The extracted teeth were visually examined to be devoid of caries, restorations, fluorosis, or abrasion. The extracted teeth were stored in distilled water until use (maximum six months). The teeth were divided into two groups, according to the test that they will undergo (Figure 1). Immediately before conditioning the enamel, the buccal surfaces were cleaned with rubber cup and pumice slurry to remove plaque and extrinsic stains.
The Experiments and Groups Used in This Study
Measurement of Shear Bond Strength
The 120 teeth used for this test were randomly assigned to three equal groups of 40 (Table 1). The roots of the teeth were embedded vertically in self-curing orthodontic resin (Dentsply, New York, USA), to facilitate bonding. The area where the bracket was to be bonded was etched in the same manner for all three study groups using 38% phosphoric acid (Pulpdent Corporation, Watertown, USA) for 30 s, followed by thorough rinsing with water. The teeth were dried with oil-free compressed air for 5 s until a frosted appearance was seen on the enamel surface. Next, a thin layer of unfilled bonding resin (Transbond XT primer; 3M Unitek, Marinova, USA) was applied with a microbrush applicator and the surface was lightly blown with air to ensure a uniform layer of primer remains before light curing for 20 s. Brackets were then bonded using Transbond XT light cure adhesive (3M Unitek, Marinova, USA) applied to the bracket bases and the brackets were pressed firmly onto the tooth. Excess adhesive was removed for each group as described in Table 1.
Description of Groups Undergoing Shear Bond Strength Testing

The bonding site and the amount of the excess resin were controlled using a customized puncher to create a window in a piece of adhesive tape of size corresponding to individual tooth and attached to each specimen prior to the bonding procedure. After seating the bracket into position, each bracket was then cured with a light-emitting diode curing light (3M Unitek, Monrovia, USA), for 20 s each on mesial and distal aspects at light intensity of 1600 mW/cm 2 . After bonding, all specimens were stored in distilled water at 37 °C.
SBS measurement was taken at two time points: after 24 h 20 teeth from each group were tested, and after three months of natural aging, the other 20 teeth were tested. Teeth were placed in distilled water in a covered glass jar and stored in an incubator at 37 °C. The water level was checked regularly and changed every week to prevent bacterial growth. Each specimen was subjected to a shear force for bracket debonding using a custom-made knife-edge blade attached to a universal testing machine (Instron, Norwood, USA) at a ramp rate of 1 mm/min. The load was then directed occluso-gingivally at the enamel–bracket interface. The results were recorded by the machine in Newton (N) and were converted to Megapascal (MPa) by the ratio of maximum load in Newton to the cross-sectional area of the bonded area in millimeters.
Failure Mode
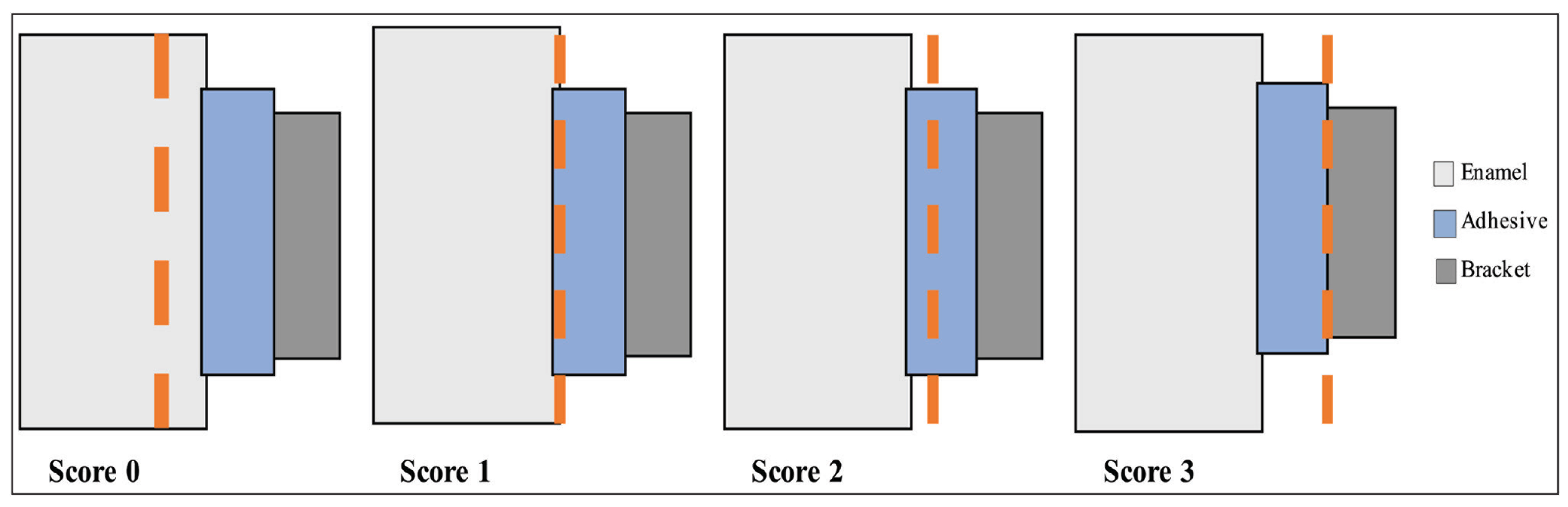
The debonded enamel surfaces were examined under 30× magnification with a digital microscope (Hirox-USA Inc., Hacken-sack, USA). A modified adhesive remnant index 11 (ARI; Figure 2) was used to determine the failure mode. All specimens that were subjected to shear test were analyzed in this way.
Modified Adhesive Remnant Index Used to Assess the Remaining Adhesive
Assessment of Enamel–Adhesive Interface Morphology
Twenty-four teeth divided into three groups of eight were used for this test. The teeth were etched and dried in the same manner as described for SBS testing, followed by the application with a microbrush applicator of a thin layer of unfilled bonding resin (Transbond XT primer; 3M Unitek, Marinova, USA) mixed with fluorescein dye. Then, the surface was lightly blown with air to ensure that a uniform layer of the primer remained before being cured with light for 20 s. After light curing, the brackets were bonded using a Transbond XT light cure adhesive (3M Unitek, Marinova, USA), which was mixed with Rhodamine B, an inert dye which facilitates visualization of resin under confocal microscopy, at a concentration of 0.1 mmol/L. Transbond XT paste was applied to each bracket base and pressed firmly onto each tooth; excess adhesive was removed as previously explained for each group.
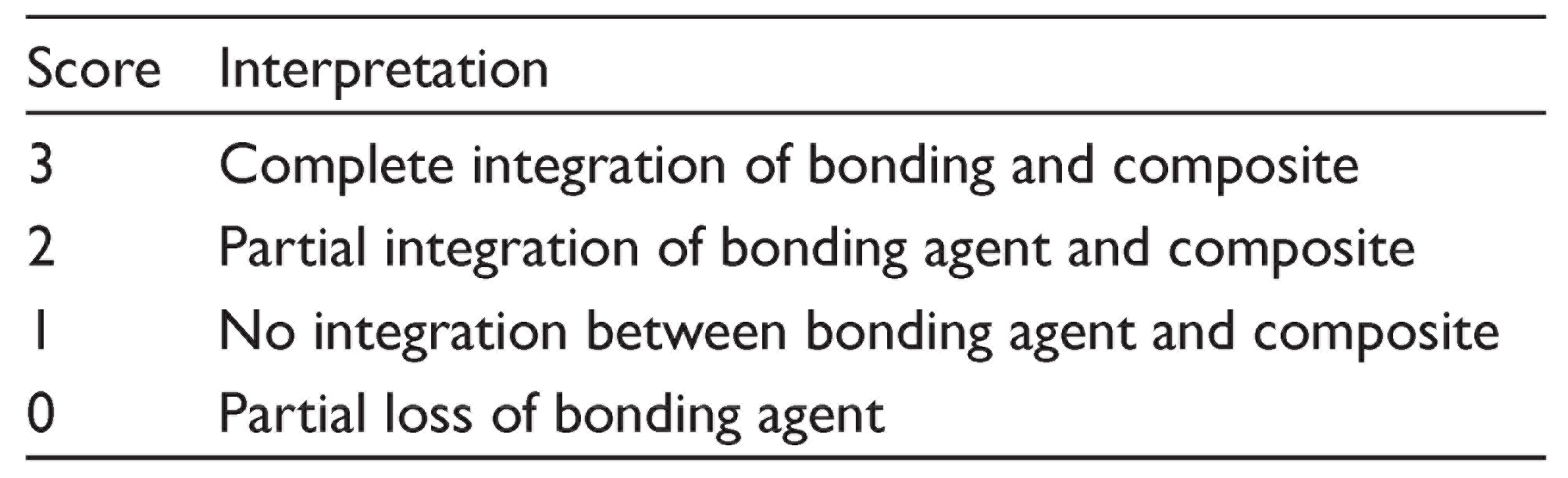
The bonded tooth surface was sectioned labiolingually parallel to the long axis of the bracket immediately after the bonding procedure to produce two sectioned slabs. The sectioning was accomplished under water coolant/lubrication with the use of a four-inch circular diamond wheel (MetLab Technologies Limited, UK) attached to a low-speed cutting machine (IsoMet, Buehler, Lake Bluff, USA). Prior to examination, each slab was hand polished using 180, 400, and 600 grit silicone carbide (SiC) papers and ultrasonicated between each paper grade for three min. A double labeling technique was used to facilitate the assessment of the enamel–adhesive interface using a CFLSM (Nikon Instruments Inc., Melville, USA) with a 20×/1.4 air objective lens. For the detection of Rhodamine B dye fluorescence, the slabs were excited with a 561-nm laser, and the fluorescence signal was detected using 600 to 630 nm emission filters. Fluorescein was excited at 488 nm and the emission was detected using a 500- to 520-nm filter. The integrity of Rhodamine B at the enamel–adhesive interface was examined at seven preselected areas. Of these, two areas were selected at the periphery of the interfaces, two at the periphery of the brackets, one area in the middle of the enamel–adhesive interfaces (mid-bracket), and the remaining two in between the periphery and middle of the brackets. A modified four-scale scoring system, reported by Celiberti and Lussi, 12 was used to analyze the enamel–adhesive interface integrity (Table 2).
Score System Used to Analyze the Integrity of Enamel–Adhesive Interface
Statistical Analysis
Data of SBS (MPa) were analyzed using a statistical software package (SPSS Inc., Chicago, USA). Two-way analysis of variance and Tukey₹s HSD (honestly significant difference) tests were applied to analyze the data. For the ARI and the enamel–adhesive interface characterization, the Pearson chi-square statistical analysis test was used. The significance level (i.e., α value) for all tests was predetermined at a probability value of .05 or less.
Results
Shear Bond Strength
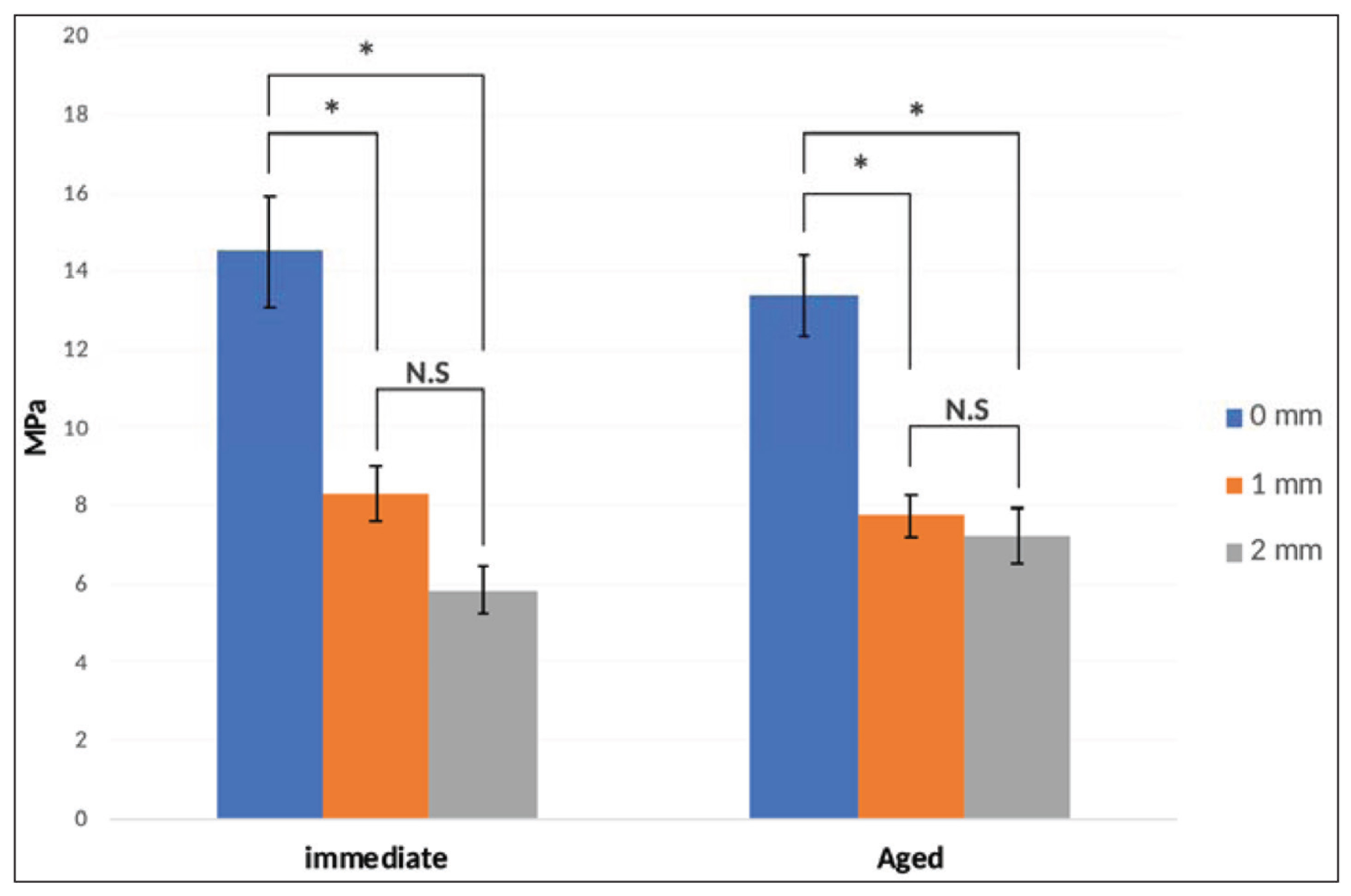
The descriptive statistics for the SBS are presented in Figure 3. No interactions were detected between time and excess adhesive amount on SBS as stated by the two-way analysis of variance (P = .337). The amount of excess adhesive induced significant variation in SBS results regardless of time (P < .05). Aging over time did not significantly affect the bond strength results (P = .888). Within a given time, statistically significant differences were found between the three test groups. Within each group, time did not significantly affect SBS results.
Mean Shear Bond Strength Over Different Storage Interval Times. The Vertical Bar Indicates Standard Error, Significant Differences Among Groups are Showed by Asterisks (P > .05)
Failure Mode
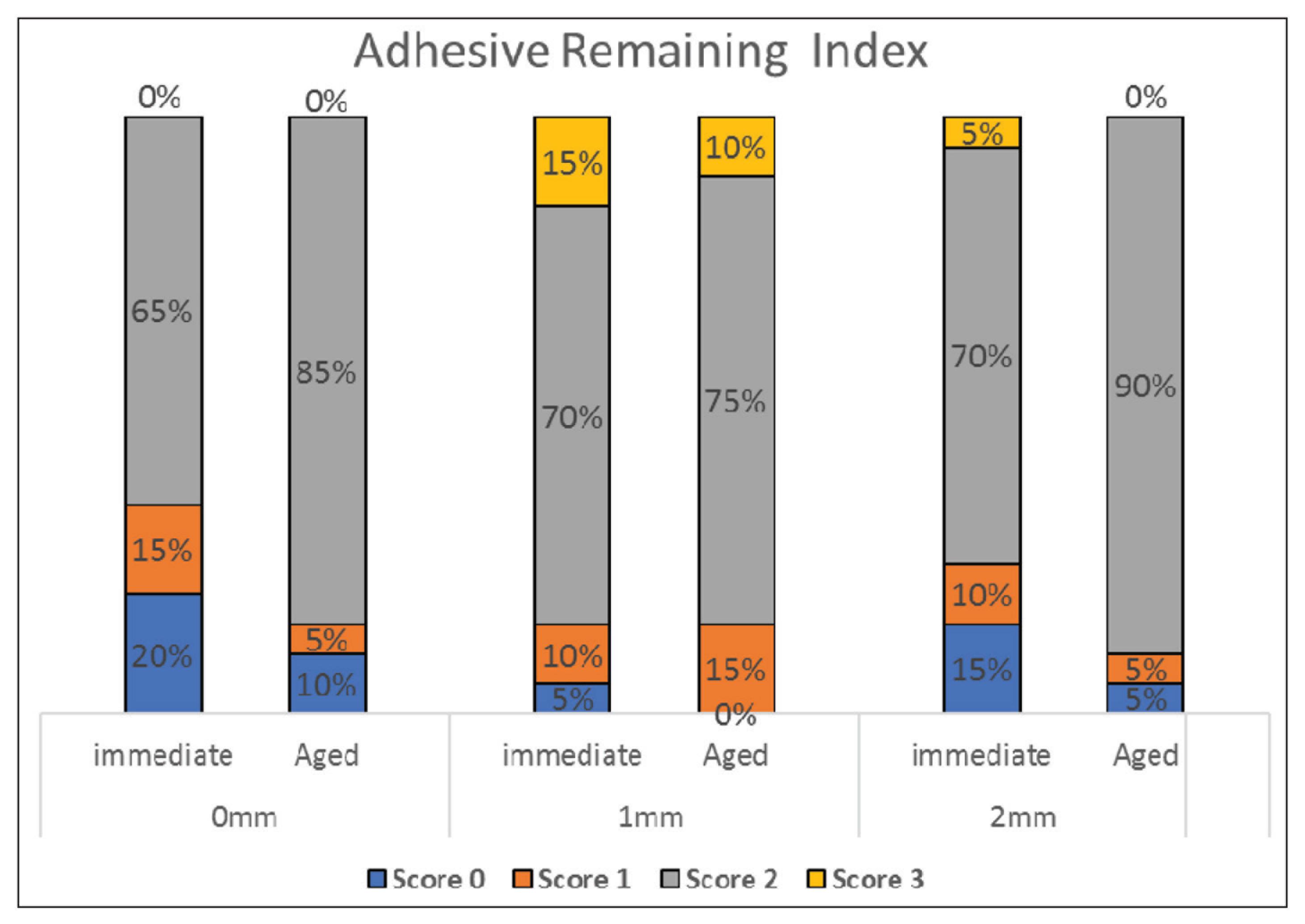
The chi-squared analysis at the two time points revealed no statistically significant difference in ARI scores among the three groups immediately or after three months of aging (Figure 4).
Adhesive Remaining Index for Test Groups Were Examined Immediately and After Three-Months of Aging Period. Data Presented as a Percentage of Each Failure Mode to the Total Failures
Assessment of Enamel–Adhesive Interface Morphology
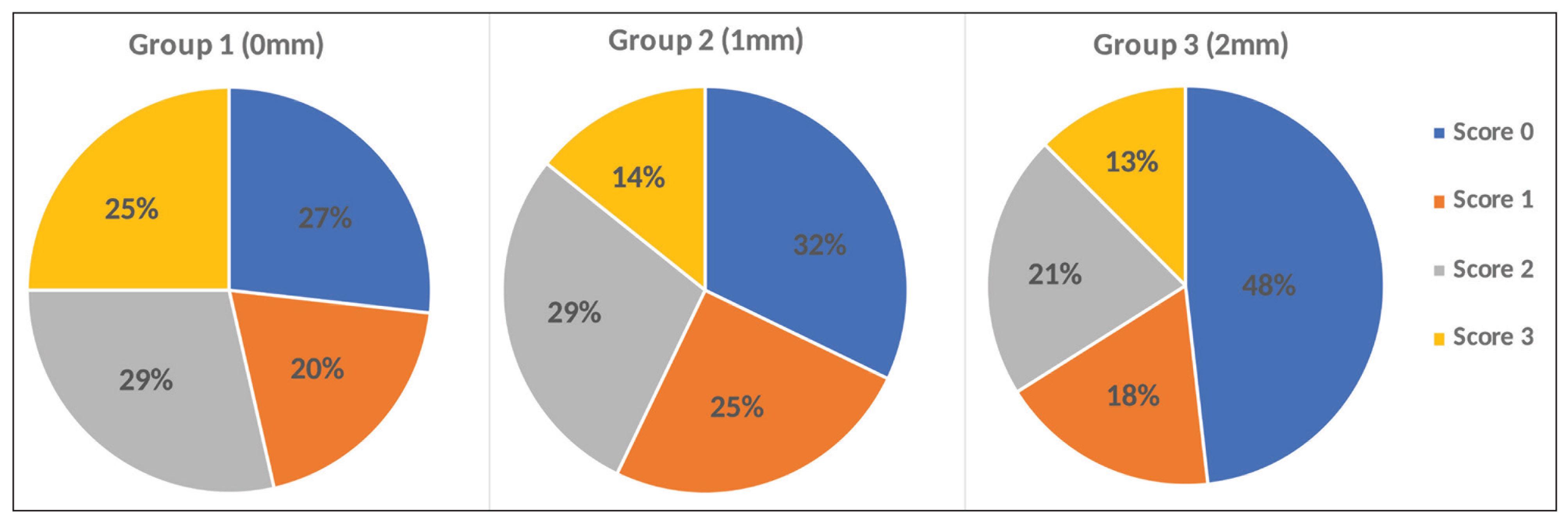
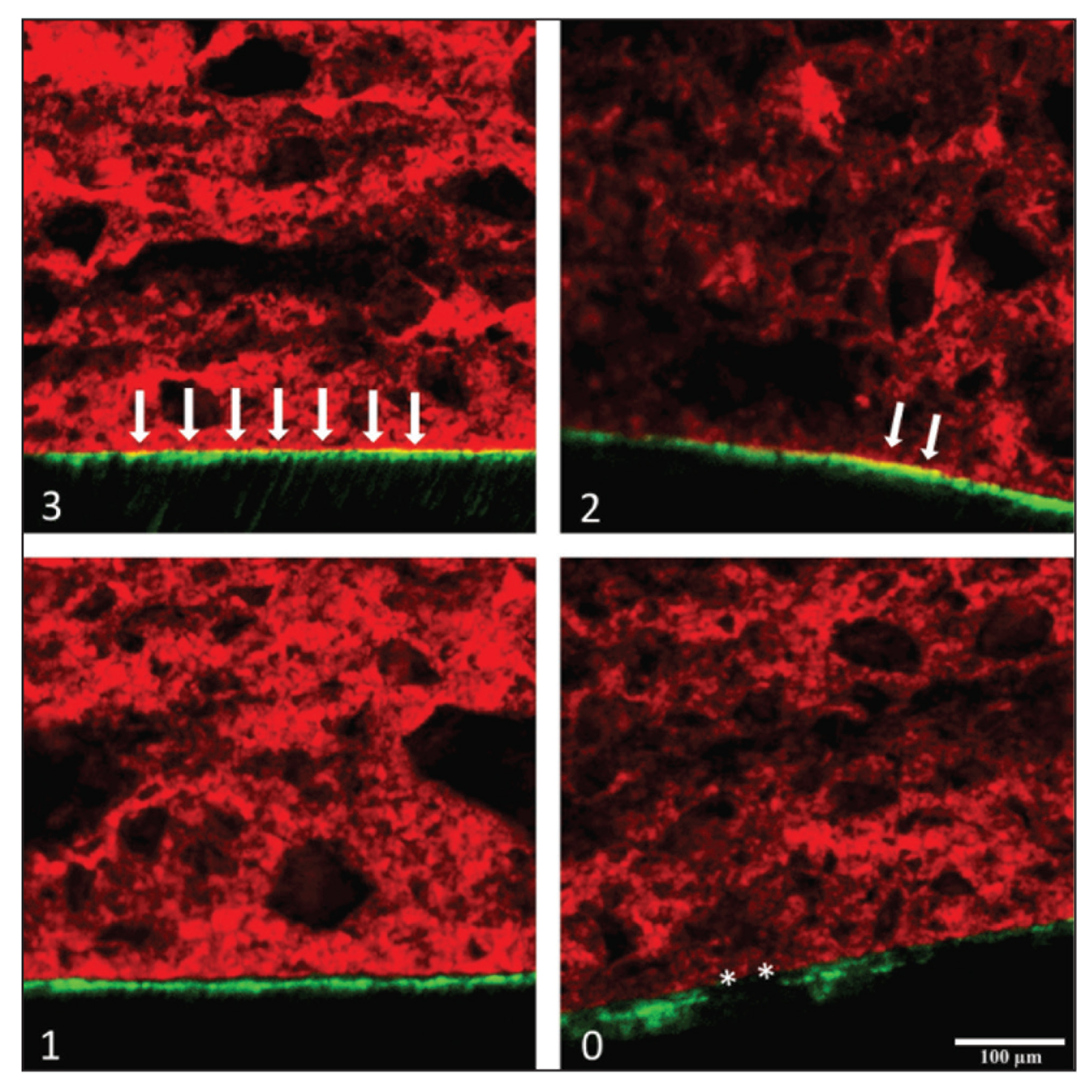
The differences in enamel–adhesive interface morphology between the three groups were not statistically significant (P = .215; Figure 5). Representative CLSM scans for each score are shown in Figure 6.
Percentage of the Enamel–Adhesive Interface Characterization Scores Obtained from Confocal Laser Scanning Microscopy Scans for Test Groups
Representative Confocal Laser Scanning Microscopy Scans (20×/1.4 Air Objective Lens) for Each Score Used to Evaluate the Enamel–Adhesive Interface Characterization. Image (3) Shows the Interface With Score 3; Image (2), Score 2; Image (1), Score 1; Image (0), Score 0. Arrows Indicate Integration of Bonding and Resin. The Asterisk (*) Indicates Areas of Bonding Loss
Discussion
There were three main aims of this study. The primary objective was to investigate the SBS of direct orthodontic bracket bonding when there is 0 mm excess adhesive, 1 mm excess adhesive, or 2 mm excess adhesive at two different time points. The failure mode was also investigated by means of ARI, along with enamel–adhesive interface morphology assessment.
It is traditionally recommended to remove excess adhesive material upon bracket bonding, because leaving excess adhesive does not improve esthetics and plaque tends to accumulate in these areas. 13 Nevertheless, a considerable amount of adhesive is often left on the tooth after bonding. 6 This could be because of busy clinical schedules, efforts to obtain ideal bracket positioning, or a belief on the part of clinicians that excess adhesive might aid retention or seal the enamel surface. Farrow et al. 10 reported better retention of adhesive material after mechanical challenges when additional adhesive material is added or excess adhesive is left behind. Although this observation did not decrease the incidence of demineralization in their study, 10 it was worth testing to know if the reported better retention of the excess adhesive could benefit the SBS.
The adhesion strength of orthodontic brackets bonded to enamel is affected by several factors. These include factors related to the adhesive, the morphology and size of the bracket bases, and the complex interactions of these different materials at the enamel–adhesive–bracket interface.14,15 The clinical perception is that the larger the brackets, i.e., the larger the bonding surface area, the better the bond strength. However, our results do not support this assumption: the larger bonding surface area did not increase the SBS. This demonstrates the complex relationship between base size and bond failure, as any increase in the bonding surface area does not result in linear increase in the ratio of applied force to failure. 16 The bond strength in this study was measured in Newton and then calculated in MPa, depending on the bonding surface area of each group. This was made possible because of three reasons: (a) The use of customized puncher allowed accurate reproducible bonding surface area for groups 2 and 3, (b) the brackets used for all groups are of the same base configuration, and (c) the debonding load was at the enamel–bracket interface which reduced the variation in load distribution pattern. For these three reasons, the actual bonding surface area can be accurately measured allowing the proper transformation of units from force (N) to stress (MPa).
In this study, the lowest bond strength was found in group 3 (2 mm excess adhesive), which was nearly 5 to 6 MPa. It was significantly lower than the 0 mm excess adhesive group but was close enough to the range that is considered to be clinically acceptable (6-8 MPa). 17 Similarly, the SBS in group 2 (1 mm excess adhesive) was 7 to 8 Mpa, which was also significantly lower than the 0 mm excess adhesive group. The presence of excess adhesive did not seem to benefit the SBS.
Throughout the years, efforts were taken to minimize the possibility of leaving excess adhesive. These efforts include the introduction of pigmented adhesives and flash-free adhesives. Pigmented color-change adhesives have distinct color that contrasts with the color of the enamel so they can be easily differentiated from the enamel during bracket placement.18,19 Studies reported no differences in SBS with these materials compared to conventional adhesives. 19 The use of flash-free adhesives remarkably decreased the excess adhesive material upon bonding 20 with comparable bond strength to conventional adhesives. 21 These findings may reflect the absence of association between the presence of excess adhesive and bond strength.
Debonding was undertaken at two time points: one at 24 h after bonding and the second after three months of natural aging. Although after 24 h debonding does not reflect the clinical scenario in which load would be applied shortly after bracket placement, this amount of time allows for the adhesive to mature to optimal bond strength.22–24 In this study, natural aging did not have any effect on SBS. The change in SBS from 24 h to three months was not statistically significant for any of the groups. This is in concurrence with the results of Trites et al., 25 who reported the same result in which the Transbond XT adhesive had no significant change in SBS between 24 h and three months.
No significant difference in ARI scores was found among the three groups at any time. Results of this study showed that the majority (n = 91) of adhesive failures occurred were mixed in nature (ARI = 2), where the adhesive was left on both the enamel and the bracket. Ideally, the adhesive failure should occur between the enamel and the bracket with little or no adhesive remaining on the tooth after debonding. The entire adhesive remained on the tooth surface (ARI = 3) in six teeth, indicating cohesive failure. This kind of failure is generally associated with increased time required to remove any excess and the risk of enamel loss. 26 On the other hand, a total of eight teeth failed by fracturing the enamel surface, four teeth from group 1, one tooth from group 2, and three teeth from group 3. It would be catastrophic for a situation like this to occur clinically. This finding was not statistically significant and these teeth were not amongst the highest-scored SBS value nor did they score a value exceeding 20 to 25 MPa, the force at which enamel fracture may occur during debonding. 27 Also, although all the samples were inspected for any cracks or deficiency before testing, these samples may have failed in this manner because of preexisting deficiencies or because the sample became desiccated during testing.
The adhesive layer quality at the enamel and orthodontic bracket interface is important in determining the success of bonding. Several factors may affect this bond including adhesive thickness, 28 filler content of adhesives, and the integrity of the interface complex. 29 In our study, score 3 was considered the ideal resin penetration and homogeneity, while score 0 was considered the poorest where partial loss of bonding occurs; both these extremities were registered amongst all study groups. Results showed no significant difference in adhesive characteristics among groups, and all three groups achieved the minimum required bond strength for bonding orthodontic brackets. These results may reflect how tag length and pattern may indicate the depth of etch but are not necessarily considered a parameter of clinical success. An ideal deep etching pattern ensures better resin penetration but does not absolutely ensure better adhesive retention. 12 In orthodontics, the bond between the enamel and orthodontic attachment is based on mechanical interlocking of adhesive to the treated enamel surface and to the mechanical undercuts at the bracket base. In our study, score 3 (ideal integration) was seen in all test groups; however, SBS was higher in group 1 (0 mm excess) compared to group 2 (1 mm excess) and group 3 (2 mm excess). This could be explained by the lack of mechanical retention offered by the bracket base along the entire bonding interface in groups 2 and 3.
This was an in vitro study; therefore, these results should be interpreted with caution, as they may differ from those obtained in the oral environment. Also, it would have been interesting to evaluate the SBS after a longer period of time to simulate the time of the average orthodontic treatment of 24 mo.
In conclusion, all teeth bonded with Transbond XT adhesives met the minimally acceptable SBS values in clinical standards. Particularly, bonding the brackets while leaving no excess adhesive showed higher SBS than the other groups with excess adhesive. The ARI scores and the enamel–adhesive interface characteristics were statistically similar among the study groups. Taken together, these results suggest that the presence of excess adhesive does not seem to benefit the SBS.
Footnotes
Acknowledgements
The authors would like to thank the College of Dentistry Research Center and Deanship of Scientific Research at King Saud University and College of Dentistry Research Center for supporting this research project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.