
Abstract
Aim:
To assess the impact of definitive maxillary obturator prostheses on oral health-related quality of life (OHRQol).
Materials and Methods:
A presented prospective study comprising 50 patients with maxillectomy defects was selected for the study. Patients with any active or persistent lesion in relation to the defect site, restrictive mouth opening along with poor general health were excluded from the study. All the patients were rehabilitated with definitive maxillary obturator prostheses, respectively. These patients were subjected for assessment of OHRQol and obturator prostheses functioning. These assessments were done using three scales OHIP-Edent-19, obturator functioning scale (OFS-15) and a novel scale—maxillofacial prosthesis performance scale (MFPPS). The assessment was done on all the patients after 2 weeks and 3 months of prosthesis function. The data were tabulated and analysed using paired sample t-test and the Wilcoxon signed rank test for paired groups and unpaired sample t-test for independent groups.
Results:
The scores of OHIP-Edent, OFS and MFPPS for definitive maxillary obturator prostheses after 2 weeks were 37.56, 30.48 and 20.50. The scores of OHIP-Edent, OFS and MFPPS for definitive maxillary obturator prostheses after 3 months were 30.30, 24.26 and 16.10, respectively.
Conclusion:
Mean differences of OHIP-Edent (7.260), OFS (6.220) and MFPPS (4.400) were observed after 2 weeks and 3 months of obturator prosthesis function. These findings show significant improvements of prosthesis in terms of functional, physical, psychological and social parameters after long-term follow-up (3 months).
List of Abbreviations
DOP: Definitive obturator prosthesis
GOHAI: Geriatric oral health assessment index
HRQol: Health-related quality of life
MFPPS: Maxillofacial prostheses performance scale
OFS: Obturator functioning scale
OHIP-Edent: Oral health impact profile-Edentulous
OHRQol: Oral health-related quality of life
QOL: Quality of life
Introduction
Maxillofacial defects are generally caused by congenital or acquired influences. Orofacial trauma and surgical intervention for tumours were the two main criteria which were classified as acquired defects. These defects result in significant changes in the anatomic structures of the maxillofacial region. 1 Post-surgical maxillary defects lead to functional impairments such as fluid leakage, nasal sounds, nasal regurgitation and compromised chewing. These functional problems may affect oral health-related quality of life.2,3. Definitive obturator prosthesis is essential in re-establishing the form of the resected portion and in reconstructing the functional separation of nasal and oral cavities. It provides immediate improvement in speech intelligibility, the resonance of voice and swallowing activities. 4
One of the greatest challenges faced by maxillofacial prosthodontist in rehabilitating these conditions is their rate of disease occurrence and financial constraints. They are frequently associated with functional, physical, psychosocial and aesthetic impairments. 5 A classification system should be reliable, rationale and should be classifying the defects according to the rehabilitative needs. While another classification provides importance only on soft tissue and bony components restoration, the classification proposed by Okay et al. gives importance to the dentoalveolar restoration and rehabilitation. The prime consideration which was given in their classification was on Palatal defect extension and the stability for successful obturator retention. 6 He has described a scheme established on the maxillary defect in the horizontal planes. The main considerations of this classification system were obturator retention and stability. In modern years, oral health-related quality of life has gained enormous impact in cancer patients. Evaluation of the treatment success is greatly influenced by physical and mental strength of the patient.7,8
The present study investigated the oral health-related quality of life of patients with maxillary defects after prosthodontic therapy with definitive obturator. However, only a few cross-sectional studies have evaluated the change in quality of life in maxillofacial defect patients with intra-oral prosthesis. Hypothesis of this study was that maxillofacial prostheses (definitive maxillary obturator) improve the quality of life in patients with maxillary defects. The objectives of the present study were to establish and evaluate the specific questionnaire scale system for maxillofacial defects (maxillary defects), to evaluate the impact of definitive obturator prosthesis on oral health-related quality of life (OHRQol) in maxillary defects (okay classification) by oral health impact profile (OHIP-Edent), obturator functioning scale (OFS) and maxillofacial prosthesis performance scale (MFPPS).
Materials and Methods
Setting and Design
This study type was a prospective cohort study done in the period between 2015 and 2019. Fifty patients with maxillectomy defects who were selected with okay classification were selected for this study.
7
All the patients were rehabilitated with definitive obturator, respectively. The type of sample selection done in the study was systematic sampling design (probability sampling). The samples size was determined with the formula:
According to the formula, a minimum of 42 patients were required for the study to obtain the statistical analysis, but in the present study we have included 50 patients which are more than the required number. The ‘inclusion criteria’ of the study were maxillary defects having provision of definitive obturator after 6 months of surgery with age limit between 30 and 75 years. The ‘exclusion criteria’ of the study were any active or persistent lesion in relation to the defect site, restrictive mouth opening and the extensive size of the defect, heavy smokers, poor general health and unacceptable quality of prosthesis. No bias in the study was noted. There were no drop outs from the study at any point of time.
Questionnaire Method
The OHRQol was evaluated by means of the (OHIP-Edent-19) 8 (Questionnaire 1), OFS-15 13 (Questionnaire 2) and a novel MFPPS-10 (Questionnaire 3) with a standardized questionnaire after 2 weeks and 3 months of prosthesis function for all rehabilitated patients. Patients were asked serious of questions by using all three scales. Answers from the subjects will be in the form of a five-point Likert scale. Answers were recorded by a single operator.
The OHIP-Edent comprises of 19 statements derived from the OHIP using an item impact method. OHIP-Edent which includes seven subscales: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability and handicap. OFS comprises of 15 statements to evaluate the masticatory ability, speech, communication difficulties and cosmetic satisfaction. 8
Total OHIP-Edent scores ranged from 1 to 95. A five-point Likert scale is used and the highest score indicates function of the obturator prostheses with greater difficulties. Lower scores indicating maxillofacial prosthesis enhance the oral health-related quality of life.
OFS and the subscales scores would be calculated by summing the scores of the responses to the 15 items and items corresponding to the subscales. Total OFS scores ranged from 1 to 75. This scale suggests that lower scores indicate better oral health-related quality of life with maxillofacial prosthesis in terms of their psychological, family and social functioning.
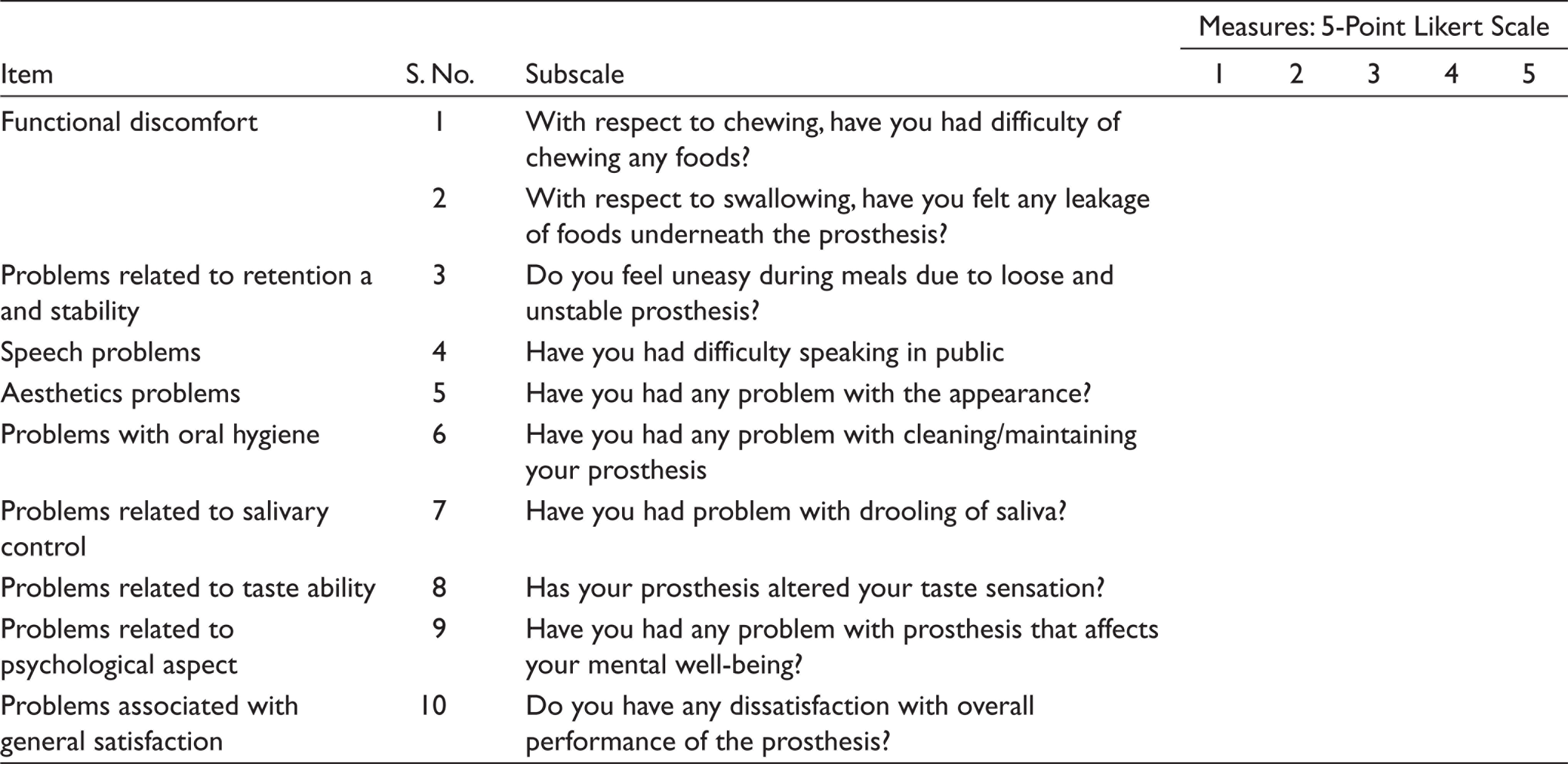
To assess the oral health-related quality of life for patients with maxillofacial defects novel scale known as MFPPS was developed. Validity and reliability were tested. MFPPS comprises of 10 statements which includes functional discomfort, retention/stability, phonetics, aesthetics, oral hygiene, saliva, taste ability, psychology and satisfaction. Internal consistency of the questions was assessed by Cronbach’s α test.
The MFPPS and the subscales would be calculated by summing the score of the responses to the 10 items and items corresponding to the subscales. Total MFPPS scores range from 1 to 50. This scale suggests that lower scores indicate significant improvement of oral health-related quality of life (OHRQol) with maxillofacial prostheses in terms of their functional, physical, psychosocial and aesthetics parameter.
Reliability of the MFPPS-10 questionnaire was evaluated using internal consistency analysis (Cronbach’s α coefficient). MFPPS has 10 questions, grouped as nine subscales or domains: functional discomfort, problems related to retention/stability, speech, aesthetics, oral hygiene, salivary control, taste ability, psychological aspect and general satisfaction.
Statistical Analysis
The collected data were analysed with IBM.SPSS statistics software 23.0 Version (USA). To describe about the data descriptive statistics, frequency analysis and percentage analysis were used for categorical variables. Mean and SD were used for continuous variables. The Cronbach’s α was used to check the reliability. To find the significant difference between the bivariate samples in paired groups, the Paired sample t-test and the Wilcoxon signed rank test were used and for independent groups the unpaired sample t-test was used. In all the above statistical tools the P value .05 is considered as significant level.
Results
Definitive Obturator Prosthesis by OHIP-Edent-19
The mean scores of oral health impact profile (OHIP-Edent-19) for 50 maxillectomy patients rehabilitated with definitive obturator prosthesis after 2 weeks and 3 months of follow-up were 37.56 and 30.30, respectively. A reasonable improvement was in subscales such as physical disability (M = 5.78/38.53%), psychological disability (M = 3.34, 33.40%), social disability (M = 5.16/34.40%) and handicap (M = 3.70/37%) after 2 weeks of prosthesis function. However, mean/average percentage score of other subscales such as functional discomfort (M = 5.42/36.13%), physical pain (M = 6.08/30.40%) and psychological disability (M = 4.08/40.8 %) indicates that there was a significant improvement only after 3 months of obturator function.
Psychological discomfort was the most prevalent OHRQol impairment with 40.8% of the patients followed by functional limitation (36.13%) and physical pain (30.4%). After rehabilitation, significant functional improvements (M = 5.42/64%) were observed only on long-term follow-up. Mean and standard deviation of each domain in OHIP-Edent scale scores are presented in Table 1.
Mean, Standard Deviation of OHIP-Edent Scale After 2 Weeks and 3 Months of Obturator Function: Paired Samples Statistics
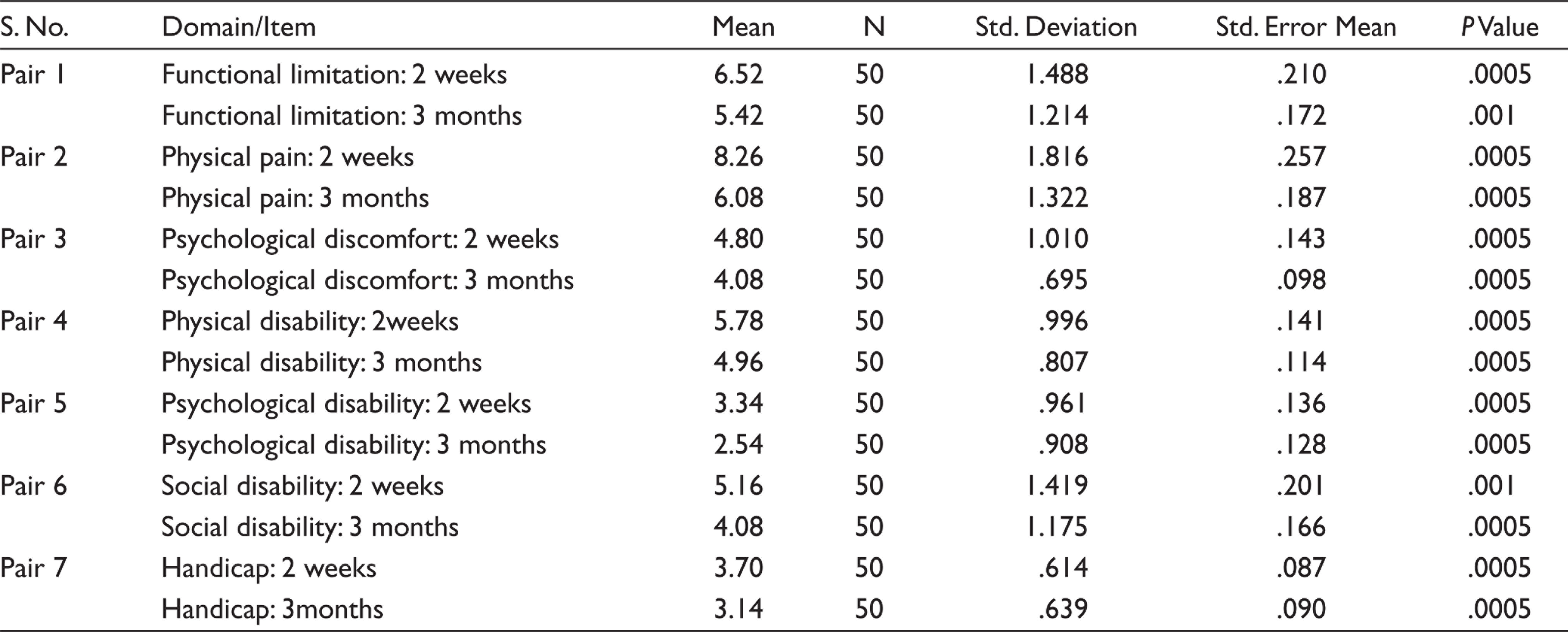
*P Value < .005 significant.
Significant improvements after rehabilitation were observed with regard to physical disability, psychological disability, social disability and handicap only after 3 months. Highest score was recorded for psychological discomfort because these patients were quite conscious of their disability and psychosocial distress caused by the disease. With regard to average percentage for OHIP-Edent-19 scale after 2 weeks and 3 months of follow-up stated that enhancement of chewing ability and prosthesis comfort requires minimum of (2 months) time frame to accommodate with new obturator prosthesis. While observing OHIP-Edent scale, highly significant difference (P value =.0005) was found in all parameters between 2 weeks and 3 months of prosthesis function.
Definitive Obturator Prosthesis by OFS
The mean OFS scores of 50 maxillary rehabilitated patients were 30.48 and 24.26 through 2 weeks and 3 months of prosthesis function, respectively. After 2 weeks of prosthesis function, mean/average percentage of score for parameters is as follows: chewing problems (M = 4.66/46.6%), speech problems (M = 13.72/45.7%), aesthetics problems (M = 1.86/37.2%) and miscellaneous problems (M = 10.24 /34.1%). Mean and standard deviation of each domain in OFS scores are presented in Table 2.
Mean, Standard Deviation of OFS After 2 Weeks and 3 Months of Obturator Prostheses: Paired Samples Statistics
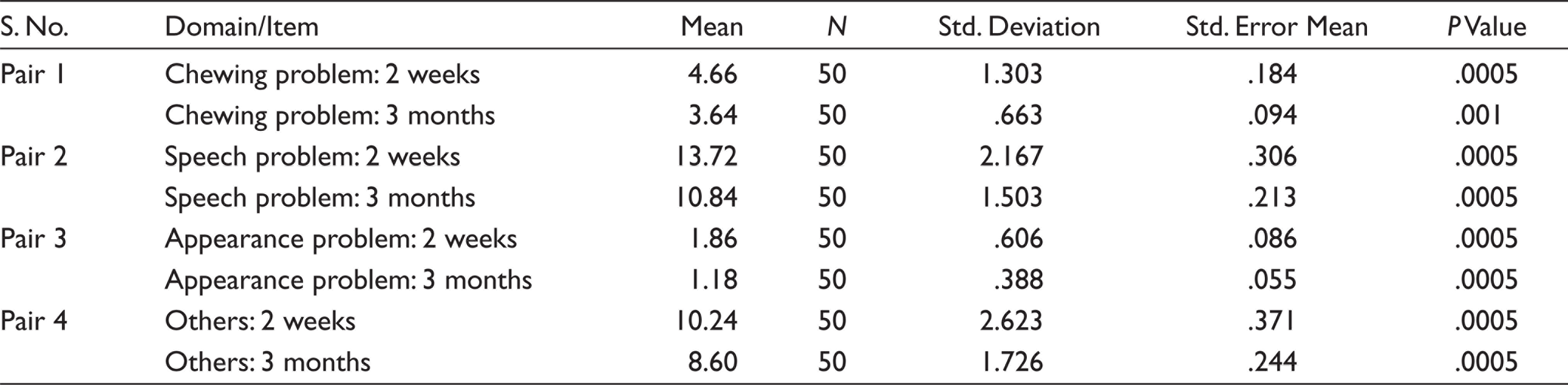
Similarly, mean/average percentage scores after 3 months of prosthesis function were chewing problems (M = 3.64/36.4%), speech problems (M = 10.84/ 36.1%), aesthetics problems (M = 1.18/23.6%) and miscellaneous problems (M = 8.60 /28.6%). The problems with chewing (difficulty in chewing and leakage of food during swallowing) were observed in 36.4% of the rehabilitated patients in OFS, the most prevalent impairment of OHRQol after 3 months of prosthesis function.
The observed clinical results specified that there was a significant improvement of 69% patients in chewing ability, speech adaptation, appearance and miscellaneous activities after 3 months when compared to 2 weeks (59.1%) of prosthesis function. This result supports that chewing and speech activities require minimum of 2 months to adapt to new prosthesis. We found that 36% of the patients experienced leakage while swallowing. This was the most common problem observed among the individuals. These results were in par with the studies conducted by Kornblith et al. (25%), Rieger et al. (20%) and Irish et al. (40%). Thus leakage while swallowing is a great concern in the patients with hemimaxillectomy even with their obturators in place.
After 2 weeks and 3 months obturator prosthesis function showed highly significant difference (P value = .0005) and was observed in all parameters of OFS.
This lower score indicates that maxillary definitive obturator prosthesis had better oral health-related quality of life in terms of their psychological, family and social functioning.
Definitive Obturator Prostheses by MFPPS
The mean MFPPS score of 50 maxillary rehabilitated patients shows 20.50 and –16.10 through 2 weeks and 3 months of prosthesis function, respectively. The mean/average percentage score of MFPPS shows for functional discomfort (M = 4.54/45.4%), retention and stability (M = 1.90/38%), phonetics (M = 2.26/45.2%), aesthetics (M = 1.78/ 35.6%), oral hygiene (M = 1.80/36%), and salivary flow (M = 1.90/38%), taste perception (M = 2.56/51.2%), psychological (M = 1.92/ 38.2%) and general satisfaction (M = 1.84/ 36.8%) after 2 weeks of prosthesis function. Perception of taste was the most prevalent OHRQOL impairment (51.2%), followed by functional discomfort (45.4%), phonetics (45.2%). The responses regarding impairment with psychological, oral hygiene, retention/stability and general satisfaction were significantly lower (36%–38%).
Mean, Standard Deviation of MFPPS After 2 Weeks and 3 Months of Obturator Prostheses: Paired Samples Statistics
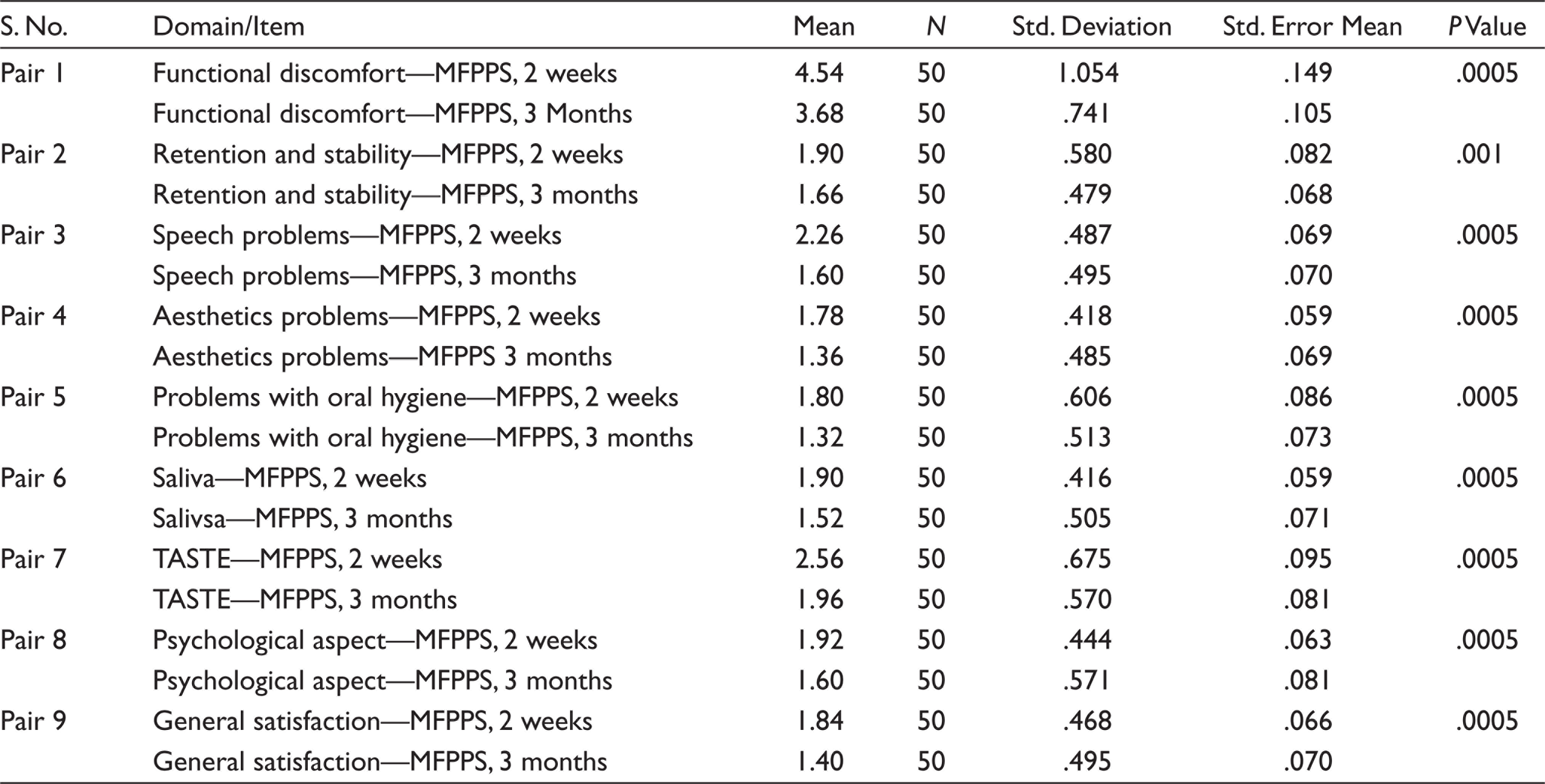
* P Value < .005 significant.
The mean/average percentage score of MFPPS shows for functional discomfort (M = 3.68/36.8%), retention and stability (M = 1.66/33.2%), phonetics (M = 1.60/32%), aesthetics (M = 1.36/ 27.2%), oral hygiene (M = 1.32/ 26.4%), and salivary flow (M = 1.52/ 30.4%), taste perception (M = 1.96/ 39.2%), psychological (M = 1.60 /32%) and general satisfaction (M = 1.40 /28 %) after 3 month of prosthesis function. Mean and standard deviation of each domain in MFPPS scores are presented in Table 3.
When comparing the average score after 2 weeks and 3 months of prosthesis function we can clearly state that all the parameters had shown dramatic improvement in MFPPS except for taste perception (39.2%). There was only marginal improvement in taste perception. Highly significant differences (P value = .0005) were observed in all parameters. Highest impact was recorded for taste perception problems. It shows a significant (P ≤ .013) reduction in MFPPS. Oral health-related quality of life improvement after prosthodontic therapy with definitive obturator prosthesis was 69%. The observed clinical results stated that there was a significant improvement with respect to prosthesis function, social and psychological aspects after 3 months when compared to 2 weeks. With regard to MFPPS, the definitive obturator prosthesis had a strong impact in maxillectomy patients.
Discussion
A very few studies had emphasis on OHRQol among patients using an intra-oral prosthesis.7–10 Smaller sample size was the main limitation of these studies. Usually, state of physical or psychological well-being and mortality measurements were seen in oral cancer patients, but OHRQol is considered more valuable in relation to psychosocial well-being of patient. In the present study, a total of 50 maxillectomy patients were investigated. This study had greater sample size when compared to previous studies.11,12 Hypothetically, major benefits of definitive obturator prostheses were to restore form, contour and function, retention, stability and support. Prosthesis retention is the most critical part in obturator prosthesis, but retention and stability of prostheses were compromised as the defect size increased, 11 resulting in compromised obturator function. Certain studies documented that obturator function was not related with the size of the defect.13,14
Numerous previous studies have used brown classification system to assess the oral health-related quality of life in maxillary defects. 15 In this study, okay classification was used. While other classification provides importance only on soft tissue and bony components restoration, the classification proposed by Okay et al. gives importance to the dentoalveolar restoration and rehabilitation. The prime consideration which was given in their classification was on Palatal defect extension and the stability for successful obturator retention. 10
In this study, an oral health impact profile-Edent-19, OFS and MFPPS-10 were utilized. These scales were designed to provide a comprehensive measure of the dysfunction, discomfort and disability attributed to oral facial conditions. This questionnaire system aids in comparing multiple study groups. The best OHIP-Edent domain percentage scores for the complete group were 25.4% for psychological disability, 27.2% for social disability and 30.4% for physical pain. The highest score was for psychological discomfort (40.8%). Results indicated that psychological discomfort improved only 60% but other subscales of OHIP scale scores have shown dramatic improvement of 70±5 % after 3 months of follow-up.
Psychological discomfort was the most prevalent OHRQol impairment with 40.8% of the patients followed by functional limitation (36.13%) and physical pain (30.4%). After rehabilitation, significant functional improvements (M = 5.42/ 64%) were observed only on long-term follow-up. Highest score was recorded for psychological discomfort because these patients were quite conscious of their disability and psychosocial distress caused by the disease. In this study, with regard to the average percentage for the OHIP-Edent-19 scale after 2 weeks and 3 months of follow-up stated that enhancement of chewing ability and prosthesis comfort requires minimum of (2 months) time frame to accommodate with new obturator prosthesis. While observing OHIP-Edent scale, highly significant difference (P value = .0005) was found in all parameters between 2 weeks and 3 months of prosthesis function. This indicated that maxillofacial prosthesis does seem to have an overall effect on oral health-related quality of life. Among the studies discussed pertaining to OHRQol in maxillectomy patients, only one study compared the OHRQol of general population with that of maxillectomy patients. With this report, oral function like phonetics, mouth opening, dry mouth, pain and deglutition was affected significantly in malignancies. 16 . It is reported in previous studies certain factors such as the extent and location of the resection, various cancer treatments, coping strategies of the patient, along with function of the prostheses and type of rehabilitation, play a significant role in determining the OHRQol. Previous studies reported the most common problems in patients rehabilitated with surgical or interim obturator prosthesis were leaching of foods, speech impairment and masticatory problem. These problems may lead to social negligence. With respect to swallowing, individuals who generated higher oral pressures were less likely to report leakage of liquids around the obturator. This indicates that a tight seal between an obturator and the hard/soft tissues of the maxilla would create an airtight space in which greater oral pressures could be generated.17,18
Mean/average percentage OFS scores after 3 months of prosthesis function were chewing problems (M = 3.64/36.4%), speech problems (M = 10.84/36.1%), aesthetics problems (M = 1.18/23.6%) and miscellaneous problems (M = 8.60/28.6%). The observed clinical results specified that there was a significant improvement of 69% patients in chewing ability, speech adaptation, appearance and miscellaneous activities after 3 months when compared to 2 weeks (59.1%) of prosthesis function. This result supports that chewing and speech activities require minimum of 2 months to adapt to new prosthesis. We found that 36% of the patients experienced leakage while swallowing. This was the most common problem observed among the individuals. Results of the present study were similar to other previous studies. Thus, leakage while swallowing is a great concern in the patients with hemimaxillectomy even with their obturators in place.12,13
For better psychosocial adjustment, speech and mastication, functioning of the obturator plays an important role in rehabilitation. This lower scores indicates that maxillary definitive obturator prosthesis had better oral health-related quality of life in terms of their psychological, family social functioning. Highest impact was recorded for taste perception problems. It shows a significant (P ≤ .013) reduction in MFPPS. Declined taste perception is caused by factors like surgical excision of maxillary segments, dental and systemic deterioration, atrophy of taste buds and medications. Rehabilitation with definitive obturator prosthesis enhances the masticatory efficiency, leading to improved taste perception. Difficulties in chewing compromise OHRQol and indicate a reduced oral well-being. Patient satisfaction and chewing ability (masticatory function) were the two key elements checked for the OHRQoL. Whenever masticatory function is not efficient, it is most likely to lead to compromised oral health-related quality of life. 4
Our study reported that the chewing efficiency significantly improved after 3 months of definitive prosthesis in all three scales (OHIP-Edent-19, OFS-15 and MFPPS-10) when compared to 2 weeks. Certain studies stated that learning to chew satisfactorily with new denture prosthesis requires at least 6 to 8 weeks (2 months). Patient will become discouraged unless they are explained about the learning period after the prostheses insertion. New memory patterns often must be established for both the masticatory muscles and the facial muscles. Once the pattern become automatic, chewing process will take place without conscious effort.
Speech problems usually are observed immediately after prosthetic rehabilitation. Older patients experience greater difficulties in adapting speech to new prosthesis and also need longer time to regain their normal speech. Speech adaptation to new prosthesis normally takes place within 2 to 4 weeks after insertion. 5 These results suggest the reestablishment of these domains at 3 months of prosthesis function. The muscles of the tongue, cheeks and lips must be trained to retain the obturator prosthesis in position on the ridges during mastication. In addition, salivary excess may impair functional comfort and make chewing and speech difficult during the initial period of obturator function. Finally, patients must understand that their appearance with new prosthesis will become more natural with time. A repositioning of the oral and facial muscles and a restoration of the former facial dimension and contour by the new prosthesis may seem like too great a change in the patient’s appearance. 5
MFFPS (novel scale) results provide strong evidence about good feasibility, measurement sensitivity, construct validity and predictability. When comparing maxillofacial defect rehabilitation with conventional prosthesis, it may possess many challenges to enhance the oral health quality of life in restoring the maxillofacial defect. This may be successfully achieved through sound theoretical knowledge, appropriate surgical technique, and surgical skill of the operator, maxillofacial prosthetic experience and team approach. Precise treatment planning and designing in fabrication of intra-oral prostheses could certainly enhance the quality of life of patients with maxillofacial. There is a significant improvement in mastication, speech, deglutition and appearance after rehabilitation with maxillofacial prostheses. Therefore, it is an essential pre-requisite for orofacial defects which in turns support the patient in resuming their normal social life.
Considering the limitations of the study the duration of the study can be evaluated for the oral health impact of the patients for 6 months and/or 1 year after the prostheses. Sample size may be considered more so that any variations in the results can be analysed.
Conclusion
Mean differences of OHIP-Edent (7.260), OFS (6.220) and MFPPS (4.400) were observed after 2 weeks and 3 months of obturator prosthesis function. These findings show significant improvements of prosthesis in terms of functional, physical, psychological and social parameters after long-term follow-up (3 months).
A highly positive association exists between oral health-related quality of life and MFPPS. Chewing ability and oral condition are the best determinants of OHRQol, predicting 46.4% of its improvement following a treatment. This association varies with time, but the factors of importance remain the same. The study can be further followed by increasing the number of sample sizes and also the duration of the study.
Footnotes
Future Scope
The future scope of this study includes analysing the oral health-related quality of life in patients receiving mandibular resection prostheses.
Author Contributions
S. Parithimar Kalaignan: Study conception, data collection, data acquisition and analysis.
Syed Ershad Ahmed: Data interpretation, manuscript writing.
Data Availability Statement
All data associated with this study are present in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Policy and Institutional Review Board Statement
The study protocol and informed consent form were approved by the ethical committee of the Vinayaka Mission’s Research Foundation, Salem (OHIP-Edent-19) and Tamil Nadu, India (Ref: VMSDC/IEC/Approval no. 069, dated: 15/7/2016).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Declaration of Consent
Informed consent was obtained for all participating patients. Definitive maxillary obturator was fabricated in the Department of Prosthodontics, Vinayaka Missions Sankarachariyar Dental College, Salem.
Questionnaires
| Item | S. No. | Subscale | Measures: 5-Point Likert Scale |
|||||
| 1 | 2 | 3 | 4 | 5 | ||||
| Functional discomfort | 1 | With respect to chewing, have you had difficulty of chewing any foods? | ||||||
| 2 | With respect to swallowing, have you felt any leakage of foods underneath the prosthesis? | |||||||
| Problems related to retention a and stability | 3 | Do you feel uneasy during meals due to loose and unstable prosthesis? | ||||||
| Speech problems | 4 | Have you had difficulty speaking in public | ||||||
| Aesthetics problems | 5 | Have you had any problem with the appearance? | ||||||
| Problems with oral hygiene | 6 | Have you had any problem with cleaning/maintaining your prosthesis | ||||||
| Problems related to salivary control | 7 | Have you had problem with drooling of saliva? | ||||||
| Problems related to taste ability | 8 | Has your prosthesis altered your taste sensation? | ||||||
| Problems related to psychological aspect | 9 | Have you had any problem with prosthesis that affects your mental well-being? | ||||||
| Problems associated with general satisfaction | 10 | Do you have any dissatisfaction with overall performance of the prosthesis? | ||||||