
Abstract
Aims and Objectives:
To determine the prevalence of congenital heart disease in patients with orofacial cleft in a Nigerian population.
Materials and Methods:
A retrospective review of all the case files of patients with orofacial cleft managed at the Dental and Maxillofacial Surgery unit of the Aminu Kano Teaching Hospital between 2007 and 2014. Data were analyzed using SPSS version 16.
Results:
A total of 133 patients with cleft lip and palate were seen during the period of study comprising 77 males and 56 females, giving an M:F ratio of 1:0.7. The age range was 15 days–36 years with a mean age of 6 years. There were five cases of congenital heart disease made up of two males and three females, giving a prevalence of 3.76 per cent.
Conclusion:
This study showed that the prevalence of congenital heart disease in patients with orofacial cleft was low. However, the need for routine echocardiography in all orofacial cleft patients especially children should not be overlooked.
Introduction
Orofacial clefts are one of the most common birth defects with a reported worldwide incidence rate ranging from 10 per cent to 22.1 per cent per 10,000 live births.1,2 A study carried out in Nigeria between 2006 and 2011 pooling data from the six geopolitical zones in Nigeria put the estimated prevalence rate of orofacial cleft at 0.5% per 1,000 live births. 3
From the surgeons’ point of view, it is essential to determine the presence of a background heart defect before any form of non-cardiac surgery because of the challenge of the complexity of the heart defect and the ability of the patient to compensate places on the anesthetist, the surgeon, and ultimately the ability of the patient to survive the surgery. 4 There is, however, a reported wide variation in the incidence of congenital heart diseases (CHDs) in children with orofacial clefts in different countries ranging from 5.4 per cent to 51 per cent in different studies. 5 To the best of the authors’ knowledge, only one study 6 was carried out in the northwestern geopolitical zone to determine the prevalence of CHDs in orofacial cleft. The study 6 determined the prevalence of CHDs to be 20 per cent in patients with orofacial cleft. However, that study had a sample size of 30 patients over a four-year period.
Orofacial clefts are divided anatomically into cleft lip (CL), cleft palate (CP), and cleft lip and palate (CLP), although various other classifications exist.2,3 Both the heart and palate develop in gestational weeks 5 through 9 as part of the cardio-craniofacial development module, which relies on complex signaling processes among interdependent embryonic tissues.7,8 Anomalous development of the heart and palate may occur as a result of shared genetic or environmental factors during embryogenesis. However, the molecular mechanisms underlying non-syndromic clefting are poorly identified and no genetic marker or environmental factor has been identified that is responsible for non-syndromic malformation of both the heart and palate.8,9
Aqrabawi 10 reported that a CHD was the most common associated anomaly (47%) observed in patients with orofacial cleft. Two studies11,12 from the southern part of Nigeria have shown the prevalence of CHDs to range from 9.5 per cent to 15 per cent.
This study was, therefore, conceived to determine the actual prevalence of CHDs in orofacial cleft and also to determine the association between the type of cleft and the congenital heart anomaly, considering the fact that a higher number of craniofacial cleft patients are seen in the maxillofacial surgery department.
Methodology
This study was a retrospective review of the case files of all patients with orofacial cleft taken to the Dental and Maxillofacial Surgery unit of Aminu Kano Teaching Hospital in Kano, Nigeria, between 2007 and 2014. These patients had also been recruited into the Smile Train program that was supporting cleft care and surgery in Nigeria. Ethical approval was obtained from the hospital ethics review board (AKTH/EC/2007/008). Informed consent had been obtained from all the patients studied.
All patients irrespective of age who had orofacial clefts during the study period were recruited into the study, while patients with missing information from their case notes were excluded from the study. Information was obtained using a questionnaire designed for the purpose for the study. All the pediatric patients with orofacial cleft routinely had an echocardiography carried out before surgical intervention, irrespective of symptoms, in order to rule out any associated CHD. While all the patients above 12 years of age with clinical signs and symptoms suggestive of a heart disease and abnormal ECG findings also had an echocardiography done.
The sample size was determined by the number of patients seen during the study period. A total of 145 patients were seen during the study period; however, the records of 12 patients were incomplete. Therefore, the sample size was 133 patients making 91.7 per cent of patients with orofacial cleft seen during the study period; hence, the sample size is considered sufficient for the study.
All data were pooled from the questionnaire designed specifically for the study, and the information collected included age, gender, type of cleft, presence of CHDs, and the type of congenital heart. The data were analyzed using SPSS version 16 and expressed using frequency tables and percentages. A chi-squared test was used to determine the association between cleft lip and palate and CHDs and a p-value of ≤ 0.05 was considered significant.
Results
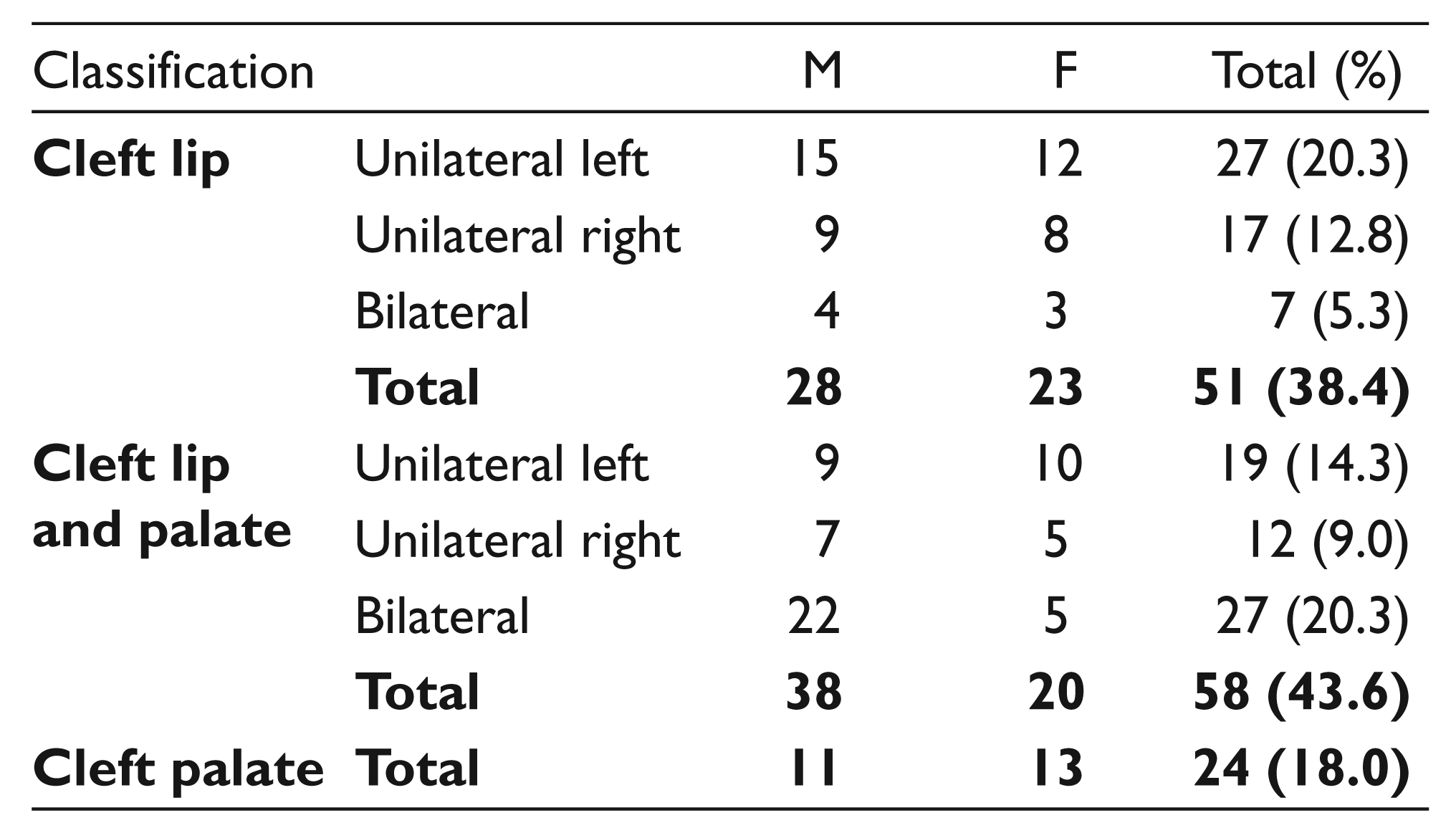
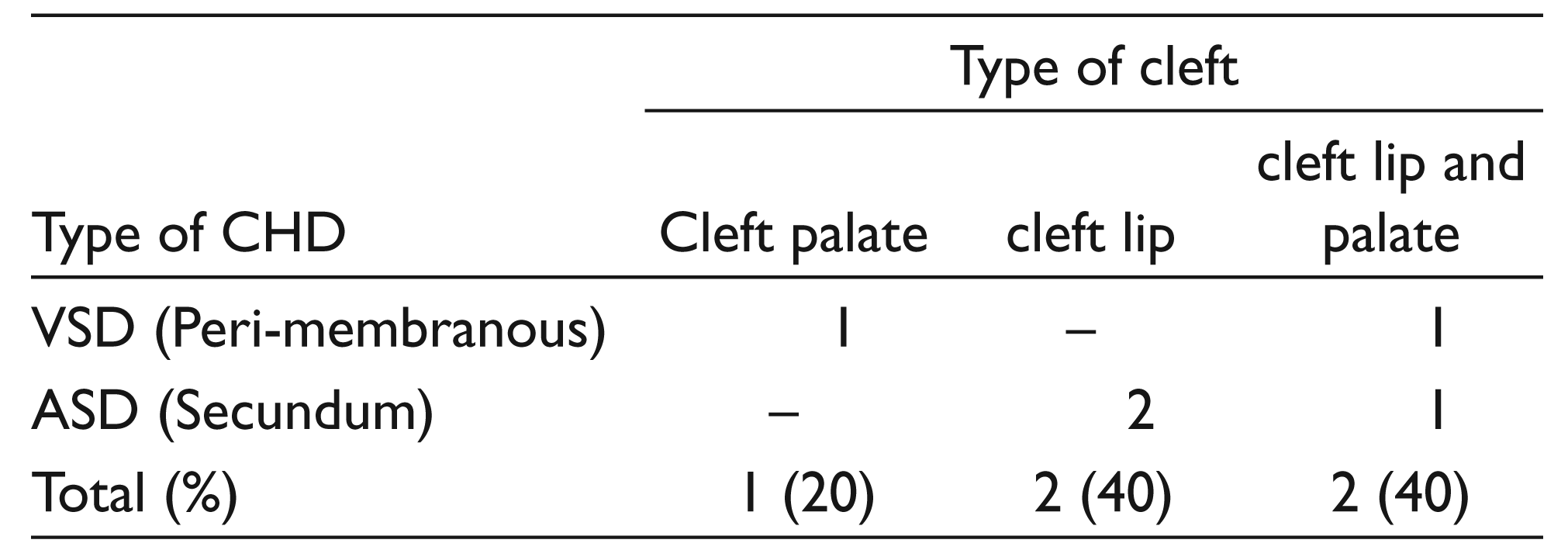
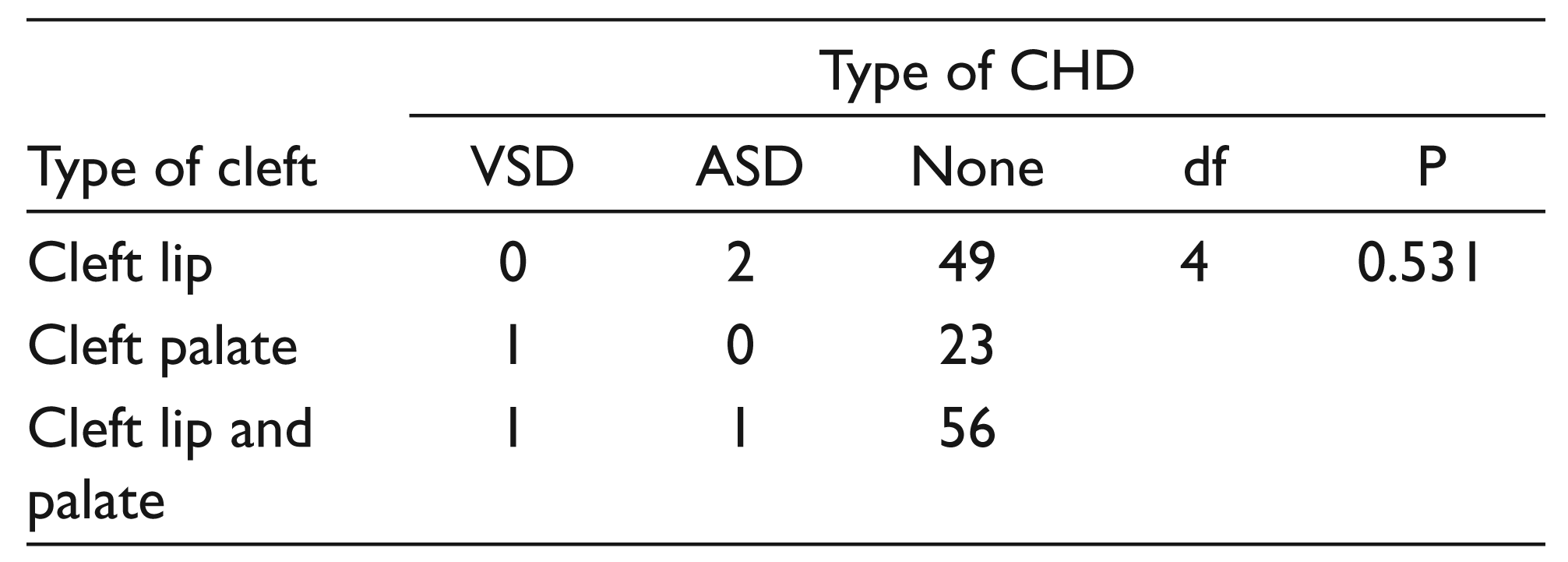
A total of 145 patients with cleft lip and palate were seen during the study period; however, only 133 of those patients had complete data and were recruited into the study. This was made up of 77 males and 56 females, giving an M:F ratio of 1:0.7. The age range was 15 days–36 years with a mean age of 6 years. There were five cases of CHDs made up of 2 males and 3 females, giving a prevalence of 3.76 per cent. The type of CHD was not significantly associated with the type of cleft lip and palate (see Tables 1–3).
Type of Cleft Versus Gender
Distribution of CHD Versus Type of Cleft
Association Between Type of Cleft and CHD
Discussion
This study found the prevalence of CHDs in orofacial cleft to be 3.76 per cent, with atrial septal defects (ASDs) occurring more commonly than ventricular septal defects (VSDs). However, the frequency of CHDs was equal in patients with cleft lip alone or cleft lip and palate.
This study was aimed at determining how common a CHD was in patients with cleft lip and palate. The study spanned over an eight-year period, and with a total of 91.1 per cent of the patients irrespective of age seen in the teaching hospital during this period being analyzed, these factors helped to add strength to the study. The limitation of this study is the fact that it was hospital based; in future, a community-based study could be carried out to determine the exact prevalence of CHDs in cleft lip and palate.
In this study, the prevalence of CHDs was 3.76 per cent which was far lower than what was reported by a similar study 6 from the same locality. The relatively lower prevalence rate noted in this study as compared to the study of Asani and Aliyu 6 could be attributed to the fact that the patients seen by those authors 6 were children under the age of 12 referred for echocardiography. However, patients seen in the maxillofacial surgery unit are usually individuals of all ages seen on their first encounter with the hospital, based on their diagnosis of orofacial cleft irrespective of cardiac symptoms, hence the larger sample size in this study.
The commonly occurring CHDs seen in this study were the ASD and the VSD with the former more in occurrence than the latter. No case of cyanotic CHD was identified in this study. This finding is similar to previous reports6,13,14 that an ASD is the most common congenital heart defect seen in patients with orofacial cleft. However, the molecular mechanism underlying the prevalent ASD and VSD in orofacial cleft has remained elusive. 13
CHD was found to occur with equal frequency in both CL and CLP, which means that the type of cleft did not necessarily correlate with the type of CHD (see Table 3). This is similar to the report by Barbosa et al. 15 This is however in contrast to other studies8,11,16 that have reported varying frequencies of cleft, with some reporting it to be more common in cleft palate and others reporting it to be more common in cleft lip and palate.
This study demonstrated that orofacial clefts are more common in males than females; however, the incidence of a CHD was more in females than males. This is in contrast to the study by Liang et al. 17 who found CHDs to be more common in males with orofacial cleft and also the studies by Sun et al. 5 and Sekhon et al. 18 that reported that malformations were more commoner in males with orofacial cleft than females.
This study has demonstrated that a CHD in cleft lip and palate though not common cannot be overlooked and the type of cleft does not necessarily determine the type of the CHD. Therefore, it is imperative that routine echocardiography for all patients with cleft lip and palate should be made a part of the health protocols for surgeons who see these patients because determining the presence of a background heart defect before any form of non-cardiac surgery can go a long way in helping the managing team determine the ability of the patient to compensate and ultimately the ability of the patient to survive the surgery.
Future research direction would be to carry out a community-based study involving the primary health care facilities and maternity homes with the aim of determining the exact prevalence of these CHDs as some children may die before being taken to the hospital.
In conclusion, this study shows that the prevalence of CHDs in patients with cleft lip and palate was low. However, the need for routine echocardiography in all orofacial cleft patients especially children should not be overlooked.
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
None.
Funding
None.