
Abstract
Aim:
To analyze the association between teeth brushing (TB) and interdental cleansing (IDC) frequency changes with gingival health status and the stage and grade of periodontitis.
Materials and Methods:
This cross-sectional study consisted of clinical examination and questionnaires. The questionnaires include demographic information and oral hygiene (TB and IDC) behavior. More than 18-year-old participants who underwent a periodontal treatment were randomly included. 548 individuals were classified as gingival healthy, gingivitis, and periodontitis according to the 2017 classification system. The degree of periodontitis was based on stage and grade systems. The data were analyzed by using Kruskal–Wallis and Mann–Whitney U tests.
Results:
The highest TB frequency (twice daily) was the highest in patients with gingivitis (83.7%) followed by healthy patients (82.9%) and patients with stage I periodontitis (52.2%). Compared to those who performed IDC daily, 18.9% of patients were healthy and 8.1% had stage II periodontitis. There was a statistically significant association between the oral hygiene behavior and periodontal health status of participants. Statistically significant association was seen between the TB and IDC with stage-grade of periodontitis. When the TB and IDC scores of different grade groups were compared at the same stage level, no statistically significant difference was found.
Conclusion:
This study showed that periodontal health status was positively correlated with TB and IDC frequency.
Introduction
Periodontitis is a chronic, multifactorial inflammatory disease that involves dysbiotic bacterial biofilms and manifests as advancing deterioration of the attachment apparatus. 1 Risk factors include smoking, diabetes mellitus, certain genetic factors, male gender, older age, and plaque accumulation.2–7 The accumulation of bacterial plaque is generally because of insufficient plaque control behavior. 8 Bacterial plaque accumulation is the main factor in the onset of gingivitis, and progression leads to periodontitis. The removal and control of plaque is critical to treat and prevent gingivitis and periodontitis. 9 Mechanical plaque control methods, e.g., teeth brushing (TB) and interdental cleaning (IDC), are suggested to remove dental plaque. 10
Oral care methods, which always include TB and IDC, can diminish the risk of periodontitis. TB is the most important method for effective plaque control. 11 It is considered an important adjunct to professional mechanical plaque removal. 12 In a systematic review conducted by Lertpimonchai et al., the frequencies of TB and going to dental visits were significantly associated with periodontitis. 8 However, TB fails to clean plaque entirely from the proximal area where periodontal diseases are prevalent. 13 Therefore, IDC devices are often recommended as an adjunct in regular oral hygiene. Various IDC tools, such as dental floss, wood sticks, interdental brushes, and single-tufted brushes, are used.11,14 Previous studies have suggested TB twice daily and dental flossing (DF) at least 2 to 4 times a week.15,16 A recent study revealed that daily DF was slightly associated with a lower prevalence of gingivitis and periodontitis.16,17
Periodontal diseases were reclassified according to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions because of some important deficiencies, including fundamental superposition and obvious pathobiology-based differences. 18 Periodontitis is described according to a staging and grading system. The stage (I-IV) identifies the severity and the complexity of periodontitis, while the grade (A-C) is used to predict event progression. In the presence of particular risk factors, such as smoking or the level of metabolic control of diabetes, grade may be increased.2,19
It has been found that there is an association between periodontal diseases and TB and IDC.8,10,12 However, it has not been investigated whether there is a relationship between TB and IDC and the severity and rate of progression of periodontal disease. In the light of this information, we hypothesize that TB and IDC could be associated with the stage of periodontitis and not with the grade of periodontitis. The aim of this study was to determine the change in oral hygiene behavior in gingival health and disease. In addition, this study aimed to determine the relationship between the stage and grade of periodontitis and TB and IDC frequency.
Materials and Methods
Setting and Design
This cross-sectional research was applied to patients who underwent periodontal treatment in the Department of Periodontology, School of Dentistry, Usak University, Usak, Turkey, between December 2019 and March 2020. The study involved clinical evaluation and a questionnaire. All questionnaires were completed after the clinical evaluation. The questionnaire was based on demographic information (i.e., age and gender) and oral health behavior (i.e., TB and IDC). The study was confirmed by the Local Ethics Committee of Usak University, and the written informed consent of all patients was provided prior to initiation of the study.
Sampling Criteria
G*Power 3.1 package program (SPSS Inc., Chicago, IL, USA) was used to determine sufficient sample size. When calculating the sample volume, type 1 error (α) = 0.05, effect size = 0.50, and test power (1 – β) = 0.80 were taken. Based on these calculations, it was defined that minimum 432 individuals would be necessary. A total of 548 individuals had been selected by the random sampling method to participate in this observational study. The inclusion criteria of this study were as follows: individuals (a) aged 18 years and older, (b) with high school or university education, (c) with a middle income level or above, and (d) at least 14 natural teeth. 20 The exclusion criteria of this study were as follows: individuals who (a) were current smokers or had a history of smoking; (b) were diagnosed with medical disorders, such as cardiovascular diseases, diabetes mellitus, immunological diseases, or rheumatoid arthritis; (c) were on any medication that could affect their periodontal conditions; (d) had received periodontal treatment in the past 6 months; and (e) had any incompatible restoration or prosthesis that increased plaque accumulation.
Intraexaminer Variability
Patients were evaluated by a calibrated periodontist (AD). Calibration exercise was performed in 12 nonstudy periodontitis patients for probing depths (PD) and attachment loss (AL). Intraexaminer variabilities were assessed after the completion of all measurements. The reproducibility of the parameters was verified by the kappa coefficient. The kappa coefficient was 0.81 for PD and 0.72 for AL.
Study Method
A total of 548 individuals were evaluated by a single clinician (AD) according to the new classification from 2018. 19 The whole mouth clinical periodontal examination included the plaque index (PI) and the presence of bleeding on probing (BOP) assessed 6 times per tooth except in the third molars. Patients were classified as having clinical gingival health, gingivitis, or periodontitis. The healthy control group consisted of 70 healthy periodontal volunteers. They exhibited a BOP score <10% with PD ≤3 mm and no sites with AL or radiographic bone loss.
A sum of 172 gingivitis patients with a BOP score ≥10 without AL or radiographic bone loss comprised the gingivitis group. The periodontitis group included 306 patients. Patients were diagnosed with periodontitis if interdental AL was detected in ≥2 nonadjacent teeth or buccal or oral AL ≥3 mm with PD ≥3 mm was detected in ≥2 teeth. 21 The level of periodontitis was assessed according to the stage and grade system. Interdental AL at a region of maximum loss was used to grade periodontitis. With certain complexity factors, the stage may be increased. The grade, which assesses disease progression, was determined by reviewing past periodontal status or bone loss according to age.19,21
After periodontal evaluation, patients were interviewed for demographic information and oral hygiene behaviors using standardized questionnaires administered face-to-face by a single clinician who was blind to the periodontal classification of patients (FK). The oral health behaviors included the daily frequency of TB and IDC. The frequency of TB was categorized by 1 of 4 options: twice daily, once daily, less often than daily (i.e., every 2 to 3 days), and not brushing. Only one question was referred to patients about IDC frequency and it had 3 reply choices: no IDC, some IDC (1 to 6 days weekly), and daily IDC.
Data Analysis
Statistical analysis was performed with the software Statistical Package version 17.0 (SPSS Inc., Chicago, IL, USA). Prior to the analysis of the data set, the normality of the data was tested for the relevant variables using the Kolmogorov–Smirnov and Shapiro–Wilk test to determine which statistical method should be used. A P value of 0.05 was considered statistically significant. The nonparametric Kruskal–Wallis and Mann–Whitney U tests were used for different stage and grade classification, because the data were not normally distributed.
Results
Data were collected from 548 patients. The average age of all patients was 42.63 ± 12.35 years, and the ages ranged from 18 to 70 years. The study population comprised 304 (55.47%) women and 244 (44.53%) men. The demographic information (i.e., gender and age) of individuals according to periodontal status is shown in Table 1. The age distribution of the patients was examined. Among patients aged 19 to 39 years, 51.6% had gingivitis and 32% had stage I periodontitis. Among patients aged 40 to 59 years, 29.6% had stage III periodontitis and 20% had stage II periodontitis. A proportion of 41.5% of the patients aged 60 years and over had stage IV periodontitis. There was a statistically significant relationship between periodontal status and age (Table 1) (P < .05).
Demographic Features (Gender and Age) of Individuals According to Periodontal Status
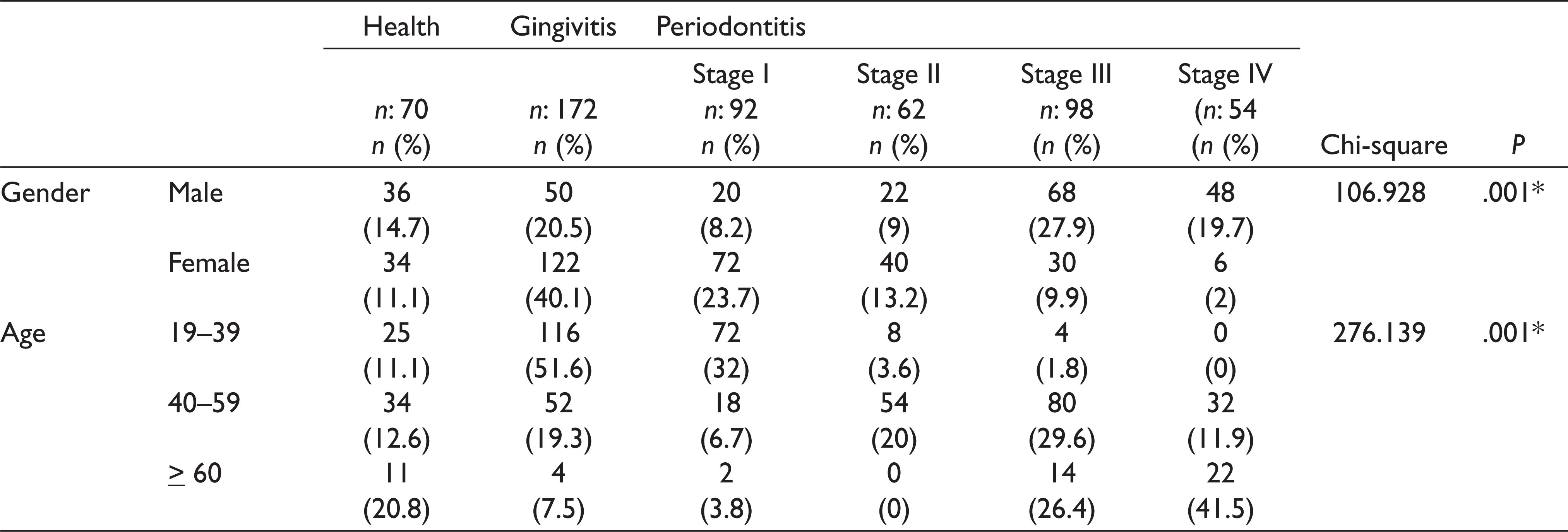
The relationship between periodontal status and gender was examined; among male patients, 27.9% had stage III periodontitis, 20.5% had gingivitis, and 19.7% had stage IV periodontitis. Among female patients, 40.1% had gingivitis and 23.7% had stage I periodontitis. There was a statistically significant relationship between periodontal status and gender (Table 1) (P < .05).
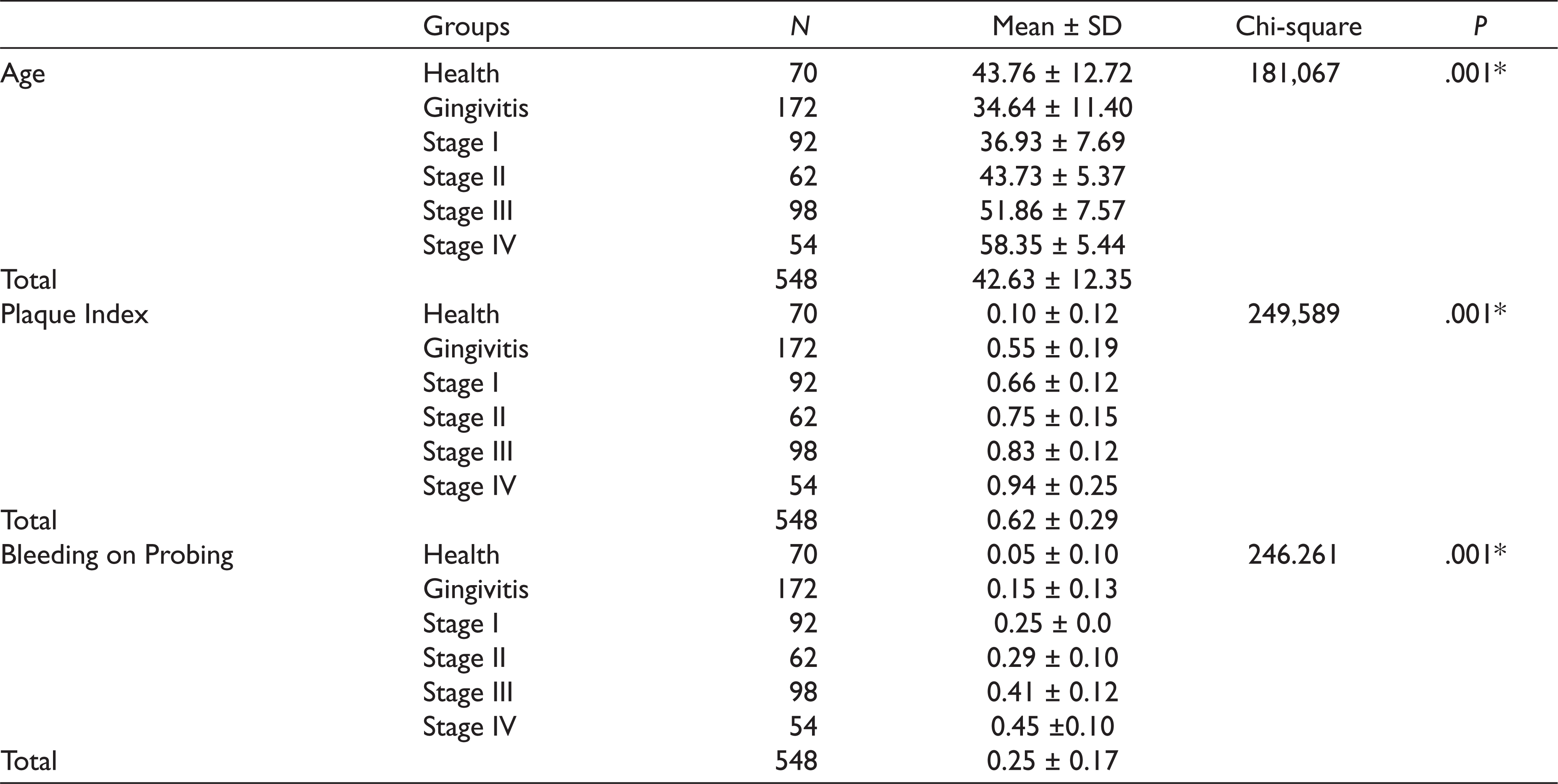
The distribution of the mean age, plaque index, and BOP parameters according to periodontal status are shown in Table 2. The mean age of the participants in the gingivitis group (34.64 years) was significantly lower than the mean age of the participants in stage I, II, III, and IV periodontitis and healthy groups (36.93, 43.73, 51.86, 58.35, and 43.76 years, respectively). The mean age of the participants in stage III periodontitis group (51.86 years) was significantly lower than the mean age of the participants in stage IV periodontitis group (58.35 years) and was significantly higher than the mean age of the participants in the healthy group (43.76 years). There was a statistically significant difference in the mean age among the groups (P < .05). The mean PI of the participants in the gingivitis group (0.55) was significantly lower than the mean PI of the participants in the stage I, II, III, and IV periodontitis groups (0.66, 0.75, 0.83, and 0.94, respectively) and was significantly higher than the mean PI of the participants in the healthy group (0.10). There was a statistically significant difference in the mean PI among the groups (P < .05). The mean BOP score of the participants in the gingivitis group (0.15) was significantly lower than the mean BOP score of the participants in stage I, II, III, and IV periodontitis groups (0.25, 0.29, 0.41, and 0.45, respectively) and was significantly higher than the mean BOP score of the participants in the healthy group (0.05). There was a statistically significant difference in the BOP score among the groups (P < .05; Table 2).
The Distribution of Mean Age, Plaque Index and Bleeding on Probing Parameters According to Periodontal Status
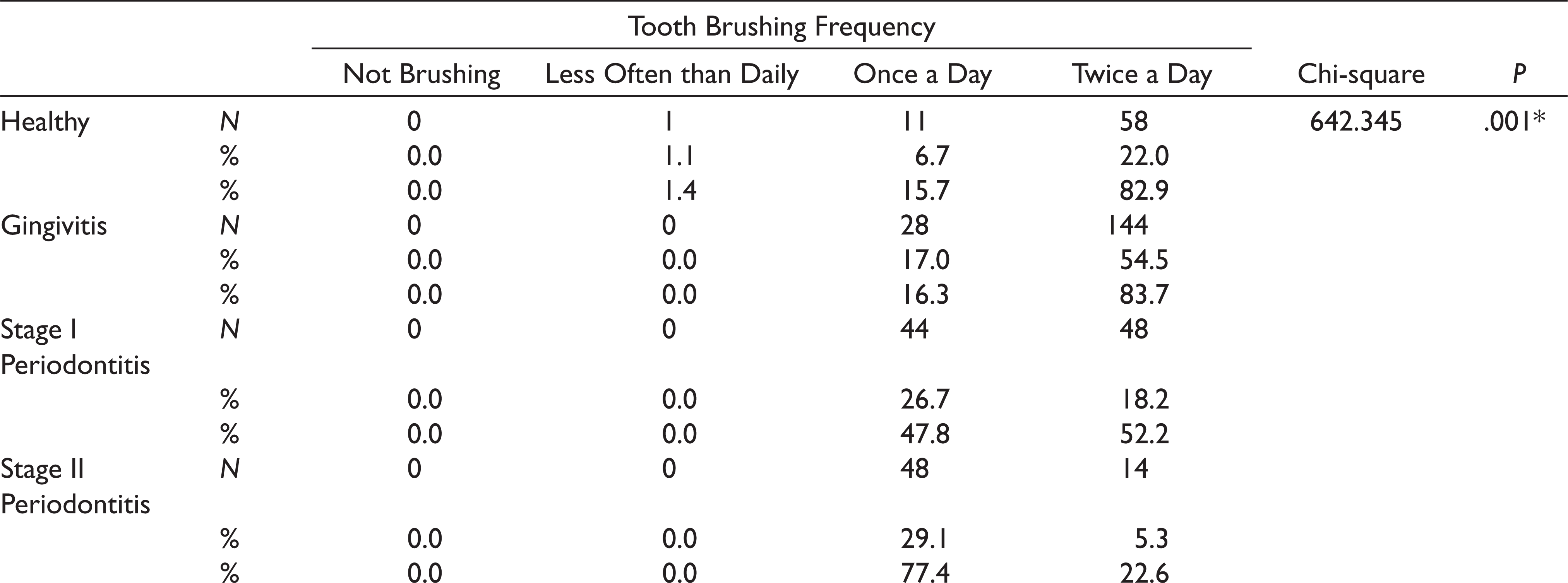
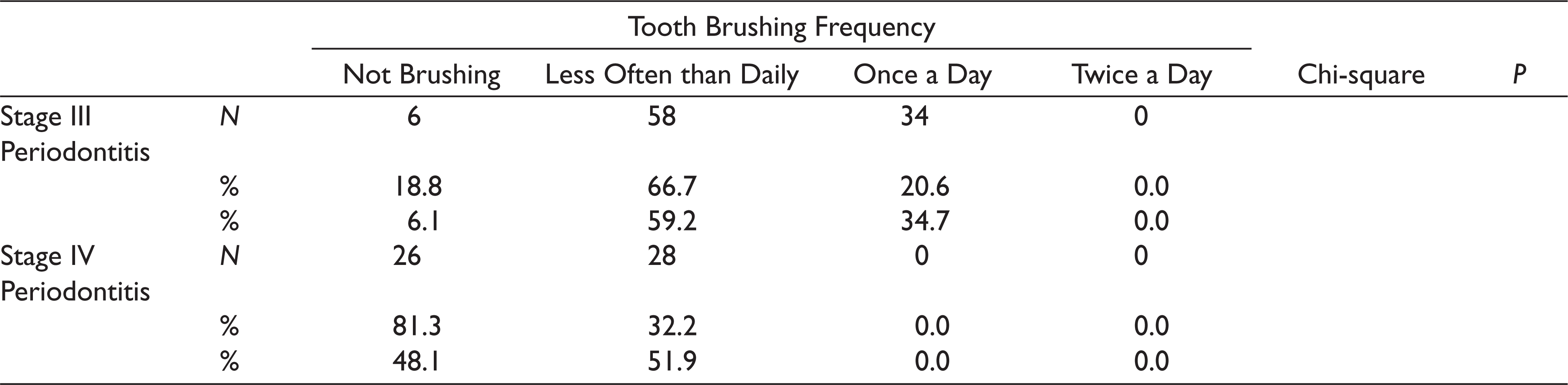
The distribution of patients in the periodontitis stage groups, gingivitis group, and healthy group according to TB is shown in Table 3. The highest TB frequency (twice daily) was highest in the gingivitis group (83.7%) followed by the healthy (82.9%) and stage I periodontitis (52.2%) groups. A proportion of 77.4% of stage II periodontitis patients brushed once daily, and 59.2% of stage III periodontitis patients and 51.9% of stage IV periodontitis patients brushed less than daily. There was a statistically significant difference in TB frequency among the groups (P < .05).
Tooth Brushing Frequency According to Periodontal Status According to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions 18
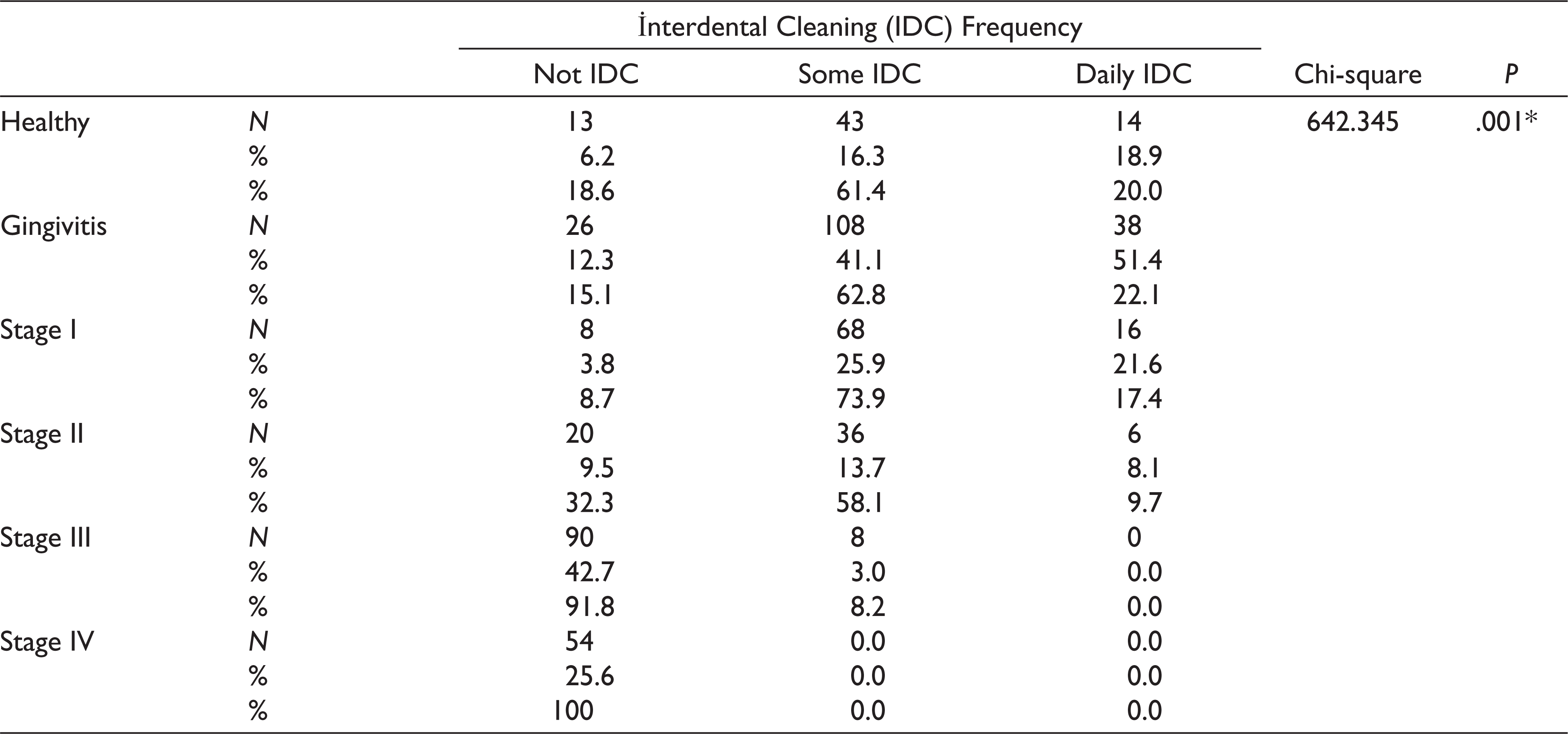
The distribution of patients in the periodontitis stage groups, gingivitis group, and healthy group according to IDC is shown in Table 4. The highest IDC frequency (daily) was highest in the gingivitis group (51.4%) followed by stage I periodontitis (21.6%) and healthy (18.9%) groups. A proportion of 61.4% of healthy patients, 62.8% of gingivitis patients, 73.9% of stage I periodontitis patients, and 58.1% of stage II periodontitis patients used an IDC device sometimes. A proportion of 91.8% of stage III periodontitis patients and 100% of stage IV periodontitis patients never used an IDC device. There was a statistically significant difference in IDC frequency among the groups (P < .05).
Interdental Cleaning Frequency According to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions 18
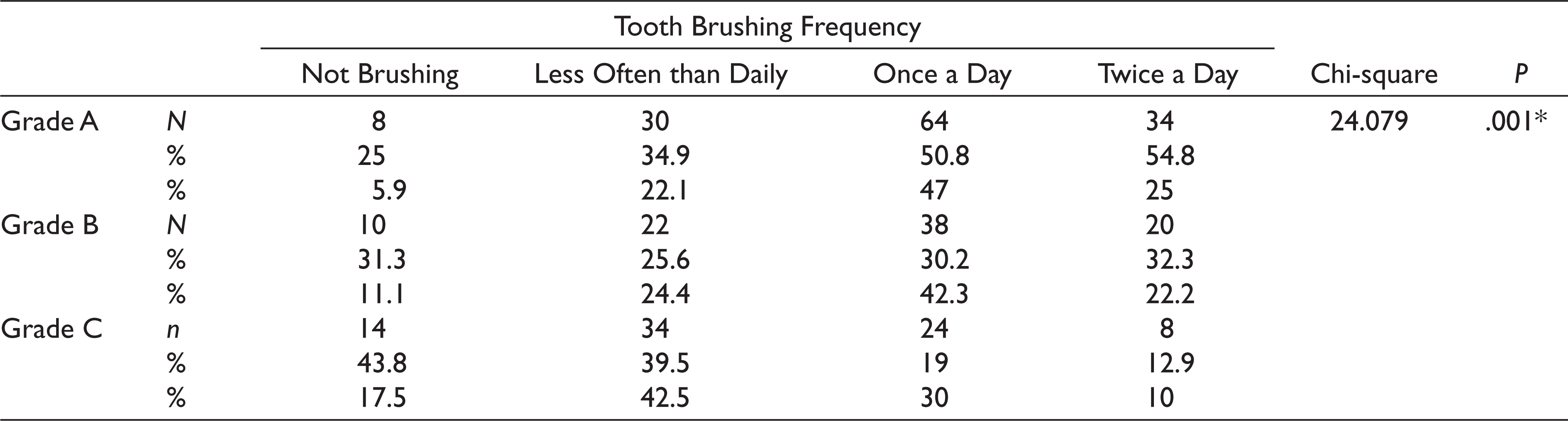
The distribution of periodontitis grade groups according to TB is shown in Table 5. A proportion of 47% of grade A periodontitis patients and 42.3% of grade B periodontitis patients brushed once daily, and 42.5% of grade C periodontitis patients brushed less than daily. There was a statistically significant difference in TB frequency among the periodontitis grade groups (P < .05).
The Distribution of Grade Amongst Groups According to the Tooth Brushing Frequency
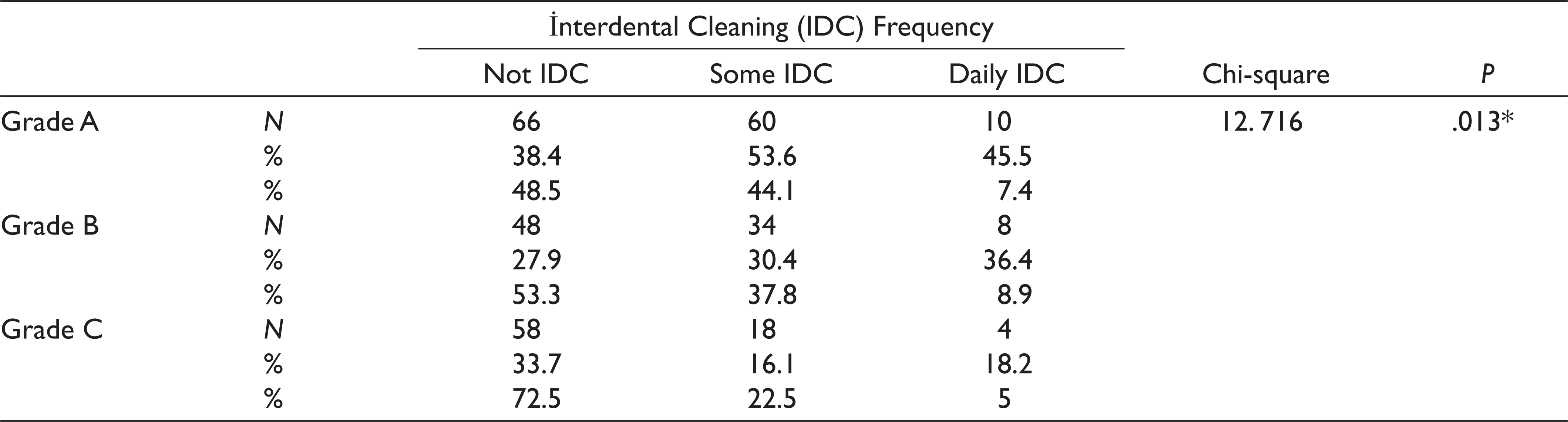
The distribution of periodontitis grade groups according to IDC is shown in Table 6. A proportion of 48.5% of grade A periodontitis patients, 53.3% of grade B periodontitis patients, and 72.5% of grade C periodontitis patients never used an IDC device. A proportion of 44.1% of grade A periodontitis patients, 37.8% of grade B periodontitis patients, and 22.5% grade C periodontitis patients used an IDC device sometimes. There was a statistically significant difference in IDC frequency among the periodontitis grade groups (P < .05).
The Distribution of Grade Amongst Groups According to the Interdental Cleaning
The distribution of periodontitis grade groups in patients with the same stage according to TB and IDC frequency is shown in Table 7. There were no statistically significant differences among grade groups in patients with the same stage (P > .05).
The Distribution of Grade Amongst Groups in Same Stage According to the TB-IDC
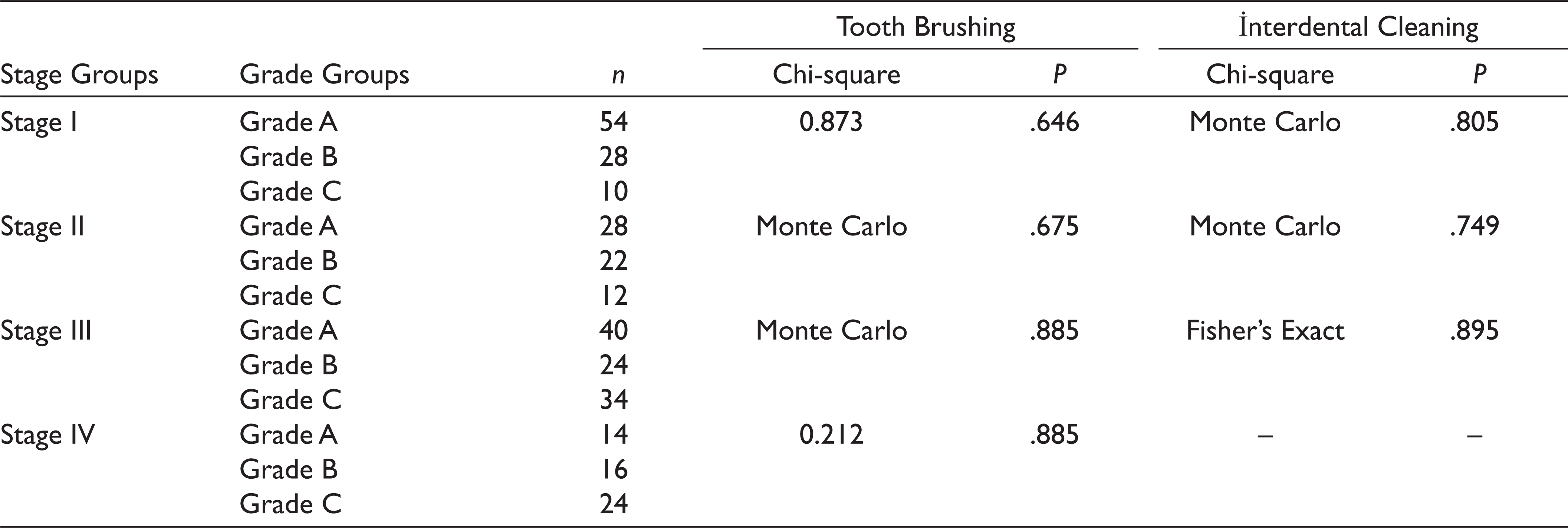
Abbreviations. TB, tooth brushing; IDC, interdental cleaning.
Discussion
Dental plaque accumulation and inadequate personal oral hygiene behavior are common and significant risk factors of periodontitis. 8 Mechanical breakdown of dental plaque, via TB and IDC, is essential to control periodontal diseases.17,22,23 TB has been recognized as a basic self-care behavioral activity to protect oral health. 24 DF and interdental brushing are commonly used IDC techniques.11,25,26 According to previous studies, TB and IDC were associated with decreased risk of periodontal diseases.16,22,23,27 The association of decreased risk of periodontal diseases with TB and IDC has been investigated in the research according to the 1999 classification. However, there is no research on the association of TB and IDC and periodontal disease according to the new classification.
In this study, frequent TB and IDC were associated with a lower severity of periodontal diseases. The highest TB score (twice daily) was highest in the gingivitis and healthy control groups, and a lower TB score was found in stage III and stage IV periodontitis groups. The highest IDC scores were highest in the gingivitis, stage I periodontitis, and healthy control groups, and lower IDC scores were found in stage III and stage IV periodontitis groups. There was a statistically significant difference in TB and IDC frequency among the groups (P < .01). Our results suggested that TB and IDC behavior were positively correlated with periodontal health status. Although a previous report stated that oral hygiene habits were not associated with periodontal disease, a recent review revealed that less frequencies TB was associated with advanced periodontal disease.27,28 A study by Harvey et al. revealed that plaque and gingival scores were reduced by TB. 24 Similarly, a study by Lee et al. demonstrated that TB and IDC benefit oral health by reducing the severity of periodontal disease. 15 Our study shows the importance of TB and IDC in periodontal health. The cause of this condition is thought to be the development of gingival inflammation as a result of increasing plaque accumulation. Gingival inflammation in a susceptible host progresses to periodontal disease as a result of AL and bone loss. 29
According to our results, TB and IDC were inversely associated with the severity of periodontitis. Individuals with stage I and II periodontitis had higher TB and IDC frequency than individuals with periodontitis of other stages. There was a statistically significant relationship between TB and IDC and the stage of periodontitis (P < .01). Lower TB and IDC frequency were associated with higher stages of periodontitis. This study indicated that the severity and extent of periodontitis was associated with lower TB and IDC frequency. Periodontitis is an inflammatory disease, and its severity is associated with moderate and heavy deposits of plaque and calculus. 30 Dental plaque accumulates on the surfaces of the teeth, leads to inflammation of the gingiva, and may progress to periodontitis.31,32 In a study by Sakanaka et al., supragingival plaque was found to be associated with periodontal inflammation severity. 33 Participants who brushed their teeth regularly had an almost 34% lower rate of periodontitis. 8
Our results were verified by a study conducted by Bernabe et al., TB frequency was negatively associated with the PD. 34 According to previous studies, DF is lightly related to a low prevalence of periodontitis. 16 Similarly, TB and IDC were associated with a low prevalence of periodontal disease in a study by Lee et al. 15 In an 11-year study done on 1025 adults in Finland, a significant relationship was found between TB and periodontal pocket depth. 12 Similarly, infrequent TB has been significantly associated with periodontitis. 27
Our data showed that TB and IDC frequency in different periodontitis grade groups were associated with the progression rate of periodontitis, while TB and IDC frequency in different periodontitis grade groups in patients with the same stage were not significantly associated with periodontitis progression rate (P > .05). There was no significant relationship between TB and IDC frequency and disease progression rate in patients with the same AL. However, despite the level of attachment, only the rate of disease progression was compared to the rate of TB and IDC, and the disease progression rate was significantly correlated. This finding is because of the fact that there is a direct relationship between plaque accumulation and AL, and other factors have a secondary effect.
In the previous classification, known as aggressive periodontitis, the frequency of TB and IDC of other individuals in the group was similar with individuals with a high disease progression rate in the new classification. This observation is because of the fact that periodontitis is a multifactorial disease, and as a result of bacterial challenge, host inflammatory responses, and bone and connective tissue metabolism differences from person to person, the onset of the disease and the rate of progression vary.35–38 Advanced bone destruction occurs because of familial and genetic predispositions in individuals with a high disease progression rate. 39 It has been suggested that the amount of microbial plaque is consistent with periodontal tissue destruction in these individuals.40,41
The relationship between periodontal disease and TB and IDC frequency were evaluated in previous studies, and the conclusion of our study was compatible with that of former studies. In addition, the severity and complexity of periodontitis and the rate of progression of periodontitis was evaluated with the new classification, but no studies have been conducted on this subject before. To the best of our knowledge, this is the first study showing the association of the stage and grade of periodontitis with TB and IDC frequency.
Conclusion
This study showed that periodontal health status was positively correlated with TB and IDC frequency. TB and IDC frequency were associated with the severity and progression of periodontitis but not associated with the progression rate of periodontitis at the same AL. Regular TB (i.e., twice daily) and IDC (i.e., some or more) may help prevent periodontal disease and the progression of periodontitis.
Clinical Relevance
Scientific Rationale for Study
TB and IDC are basic self-care methods. However, there is no sufficient evidence on association between oral hygiene behavior and stage and grade of periodontitis.
Principal Findings
Stage and grade of periodontitis was related with TB and IDC, whereas grade of periodontitis in the same stage was not related with TB and IDC.
Practical Implications
Periodontal health status was positively correlated with TB and IDC frequency.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.