
Abstract
Abstract
Introduction: Fixed orthodontic therapy is considered to be one of the important risk factor for plaque accumulation, since various orthodontic components serves as the retentive areas for plaque accumulation and thus increasing the risk of caries and periodontitis. Therefore these patients must be encouraged to maintain good oral health throughout the treatment.
Objective: To investigate the effects of reinforced oral hygiene instruction programme with and without professional tooth cleaning on the plaque accumulation and gingival health of orthodontic patients wearing fixed multibracket appliances.
Material and Methods: Forty patients with fixed orthodontic appliances in the age range of 12–28 years were divided randomly into Group I (n=20) and Group II (n=20). Group I received oral hygiene instructions and Group II received similar instructions supplemented with one sitting of professional tooth cleaning. The plaque and gingival index were recorded at the baseline (before the instructions), after 4 and 8 weeks in both the groups. At each visit all the instructions were reinforced in both the groups.
Results: Intergroup comparison showed significant decrease in the mean plaque score at 4 weeks in Group II (p<0.01), but no significant difference in the mean plaque score at 8 weeks and mean gingival scores at 4 and 8 weeks between both the groups. Within the group comparison, showed that the mean values of both the indices showed significant decrease after 8 weeks in both the groups (p<0.01).
Conclusion: Reinforced oral hygiene instruction programme with or without professional prophylaxis can lead to efficient control of plaque accumulation as well as improvement in the gingival health of orthodontic patients wearing multibracket appliances. However, provision of professional tooth cleaning should be based on individual plaque control needs.
Keywords
Introduction
Successful orthodontic treatment lies in correcting occlusion in the best possible manner so as to improve aesthetics and function but without affecting the pre-existing health of teeth and supporting tissues. 1 However, maintaining a good oral hygiene during orthodontic treatment is challenging. This is because the brackets, archwires and other components provide retentive surfaces that encourage plaque accumulation and thus increase the pathogenicity of microbes. Numerous studies have proved that orthodontic patients have an increased risk of developing gingivitis and periodontal disease.2-8 This can be attributed to the lack of education and motivation provided to the patients by the treating orthodontist.9-12 Recent surveys carried on orthodontic patients have shown that knowledge, attitude and practice of oral hygiene among orthodontic patients are poor and there is a need of better education and motivation.12, 13 Hence, increasing their awareness by carrying out preventive programs is the need of the hour.1, 14-18 Studies have shown that if adequate plaque control measures are taken, minimal periodontal disease, bone loss and caries will occur during the course of fixed orthodontic treatment.19, 20 However, these studies differ largely with respect to content, design and duration and the methods of oral hygiene motivation. 21 Whereas some compared verbal or written or visual-based methods for motivation, others have compared techniques like indicator dyes or showing live bacteria to patients under a phase contrast microscope.21-25 Some recent studies have suggested text messaging or an app-based approach to be applied to the conventional protocol.26-29 Still others have compared powered and manual tooth brushes, and fewer have evaluated the efficiency of toothpastes and mouthwashes with different ingredients and oral irrigators on gingival health and plaque elimination.30-34 The results of all these studies are somewhat conflicting as to what should be the most appropriate oral hygiene program. To overcome some of these problems, we designed a study in which a simplified oral hygiene instruction (OHI) program without any elaborate equipment was used and reinforced at periodic intervals. Furthermore, for maintaining a healthy periodontium, professional tooth cleaning is required for majority of the orthodontic patients. However, most studies have tested OHIs alone or combined with other modalities of plaque removal, and little work if any has been done to analyze the combined effects of oral hygiene motivation and professional prophylaxis. 35 The aim of the present study was to investigate the effects of reinforced OHI program with and without professional tooth cleaning on the plaque accumulation and gingival health of orthodontic patients wearing fixed multibracket appliances.
Materials and Methods
Following approval from the institutional research and ethical committee and obtaining informed consent, 50 patients who were undergoing multibracket fixed orthodontic therapy in the Department of Dentistry, Govt. Medical College and Hospital, Chandigarh were examined. However, only 40 (25 female and 15 male) patients in the age range of 12 to 28 years were selected using the below-mentioned criteria.
Inclusion criteria:
Being under multibracket orthodontic treatment involving both the arches for a minimum period of 6 months and planned to last for at least 6 months from the beginning of the study Good general health condition Full complement of permanent dentition Absence of any active periodontal disease and caries
Exclusion criteria:
Patients who had been under treatment for less than 6 months Medically compromised patients Patients who were mentally or physically challenged Patients with cleft lip and palate where oral hygiene regimen could be compromised
All patients were being treated by the same orthodontist and with the same fixed orthodontic system (Gemini, MBT prescription, 0.018-inch slot, 3M Unitek) applied with a light cure bonding agent.
Recordings
The oral hygiene condition was evaluated by recording plaque and gingival indices at the baseline and at 2 subsequent visits.
Plaque Index
Plaque index (PI) 36 was evaluated on all the 3 facial surfaces (mesio-facial, facial, and disto-facial) on selected teeth, that is, upper and lower anterior teeth and premolars using a mouth mirror, a light source and a dental explorer. Molars were not included. PI was not calculated for lingual surfaces as no attachments were used. Scoring was as follows: 0, no plaque; 1, film of plaque adhering to free gingival margin and adjacent area of tooth, which could be seen in situ after application of disclosing solution or by using a probe on tooth surface; 2, moderate accumulation of soft deposits within the gingival pocket or tooth and gingival margin that can be seen with naked eye; and 3, abundant soft matter within the gingival pocket and tooth along with the gingival margin.
PI for one tooth was calculated by adding the scores of 3 surfaces and dividing by 3 (number of tooth surfaces). Mean PI for individual was calculated by adding values for each tooth and then dividing by the number of teeth.
Gingival Index
To assess the severity of gingivitis, gingival index (GI) 37 was evaluated on the 3 facial surfaces (mesio-facial papilla, fascia margin, and disto-facial papilla) on selected teeth, that is, upper and lower anterior teeth and premolars. A blunt instrument such as periodontal probe was used to assess the bleeding potential of the tissues, using sufficient lighting and a mouth mirror. Score 0 was given for absence of inflammation or normal gingival; 1 for mild inflammation, slight change in color, slight edema and no bleeding on probing; 2 for moderate inflammation, moderate glazing, redness, edema and hypertrophy and bleeding on probing; and 3 for severe inflammation, marked redness and hypertrophy, ulceration and spontaneous bleeding. GI for one tooth was calculated by adding the scores of 3 surfaces and dividing by 3 (number of tooth surfaces). The mean GI for an individual was calculated by adding values for each tooth and then dividing by the number of teeth.
After baseline recording, all patients were randomly divided into 2 groups of 20 patients each. Group I received comprehensive OHIs only, and Group II received OHI and professional tooth cleaning.
Oral Hygiene Instruction
At first, all patients were shown the quantity and location of plaque in the oral cavity by staining their teeth with 2 tone disclosing solutions (AlphaPlac) and were informed how the plaque is formed, the composition of plaque, its effect on gingival and oral health and also the importance of its removal. After that, all the patients were demonstrated Bass Brushing technique on typodonts with multibracket appliances. 38 Immediately after, the participants were asked to reproduce the brushing technique. Patients were instructed to brush their teeth thrice daily after each major meal for a minimum duration of 3 minutes.
Similar oral hygiene regimens have been used previously and were found to be successful in patients with fixed orthodontic appliances.39, 40 In our study, we also evaluated the effect of professional cleaning along with reinforced OHIs.
After receiving OHIs, patients in group II received professional tooth cleaning. After the first appointment, both the groups were called at 2 subsequent appointments, at an interval of 4 weeks. At each of the later appointments, repeated motivation and instruction in oral hygiene care were given to all the patients in both the groups, and PI and GI were recorded. One single blinded examiner performed all the recordings.
Statistical Analysis
Student’s t test was used for comparison of mean values of both the indices between 2 groups at different stages of follow-up and a paired t test was performed on all tested variables to evaluate the differences between the 2 successive readings from the baseline within 2 groups.
Results
On intergroup comparison, the baseline values of PI and GI showed no significant difference (Table 1). However, at 4 weeks, a statistically significant decrease was found in mean PI of Group II vs Group I (P < .05), with no statistically significant difference at 8 weeks. GI showed no statistically significant difference between the 2 groups at all visits.
Intragroup analysis showed a decrease in mean PI of 0.1933 ± 0.232 (P < .001) at 4 weeks and of 0.2394 ± 0.313 at 8 weeks in Group I, both of which were highly significant (Table 2). The mean GI in group I showed statistically nonsignificant decrease at 4 weeks but progressed to statistically significant decrease of 0.1463 ± 0.220 (P < .01) at 8 weeks. In Group II, mean PI showed a highly significant decrease of 0.3387 ± 0.328 (P < .001) at the first visit and of 0.2974 ± 0.339 (P < .001) at the second visit. Similarly, GI decreased by 0.2167 ± 0.226 (P < .000) at 4 weeks and by 0.1638 ± 0.184 (P < .001) at 8 weeks. Both were highly significant.
Discussion
Orthodontic treatment in patients wearing multibracket appliances introduce additional plaque retention sites on tooth surfaces, thus encouraging proliferation of cariogenic bacteria and periodontopathic microorganisms. This leads to chronic hyperplastic gingivitis, white spot lesions, decalcification, and cavity formation. Therefore, it is important to ensure a high standard of oral hygiene in these patients to extend the long-term benefits of orthodontic therapy. Because of the paucity of studies comparing the effect of OHI alone and OHI with professional tooth cleaning on gingival health of these patients, the present study was undertaken. Our study showed that reinforced OHI program with and without professional tooth cleaning reduced the PI and GI as compared with baseline.
Optimal oral hygiene requires thorough and clear instructions, adequate tools and patient motivation. In our study, we followed oral hygiene program which was comprehensive and complete in itself, yet quick, repeatable and easily acceptable to the patient. The armamentarium used was minimal, consisting of disclosing solution, tooth brush and a typodont, thus making this more user friendly and economical. The advantage of this program is that it can be done in both private practice and hospital settings and can be easily carried out by dental auxiliaries.
Comparison of Mean Values of Plaque and Gingival Index at Baseline, After 4 Weeks and After 8 Weeks in Group I and Group II
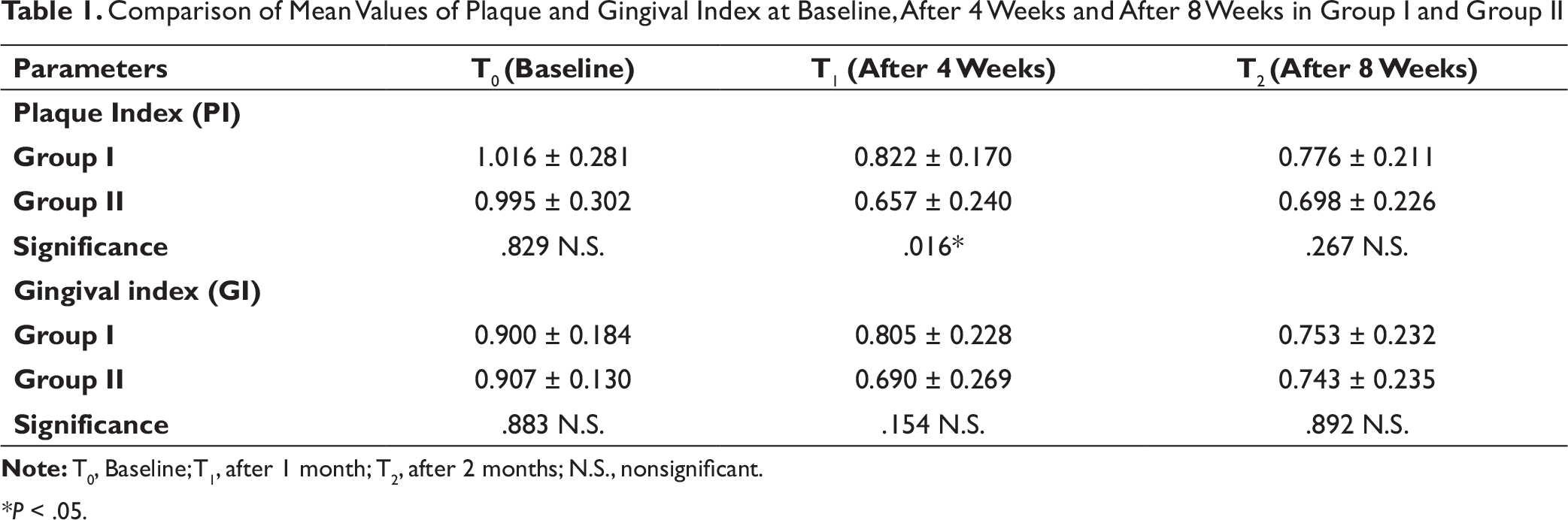
*P < .05.
Mean Changes of Plaque and Gingival Index at Different Time Interval Within Each Group
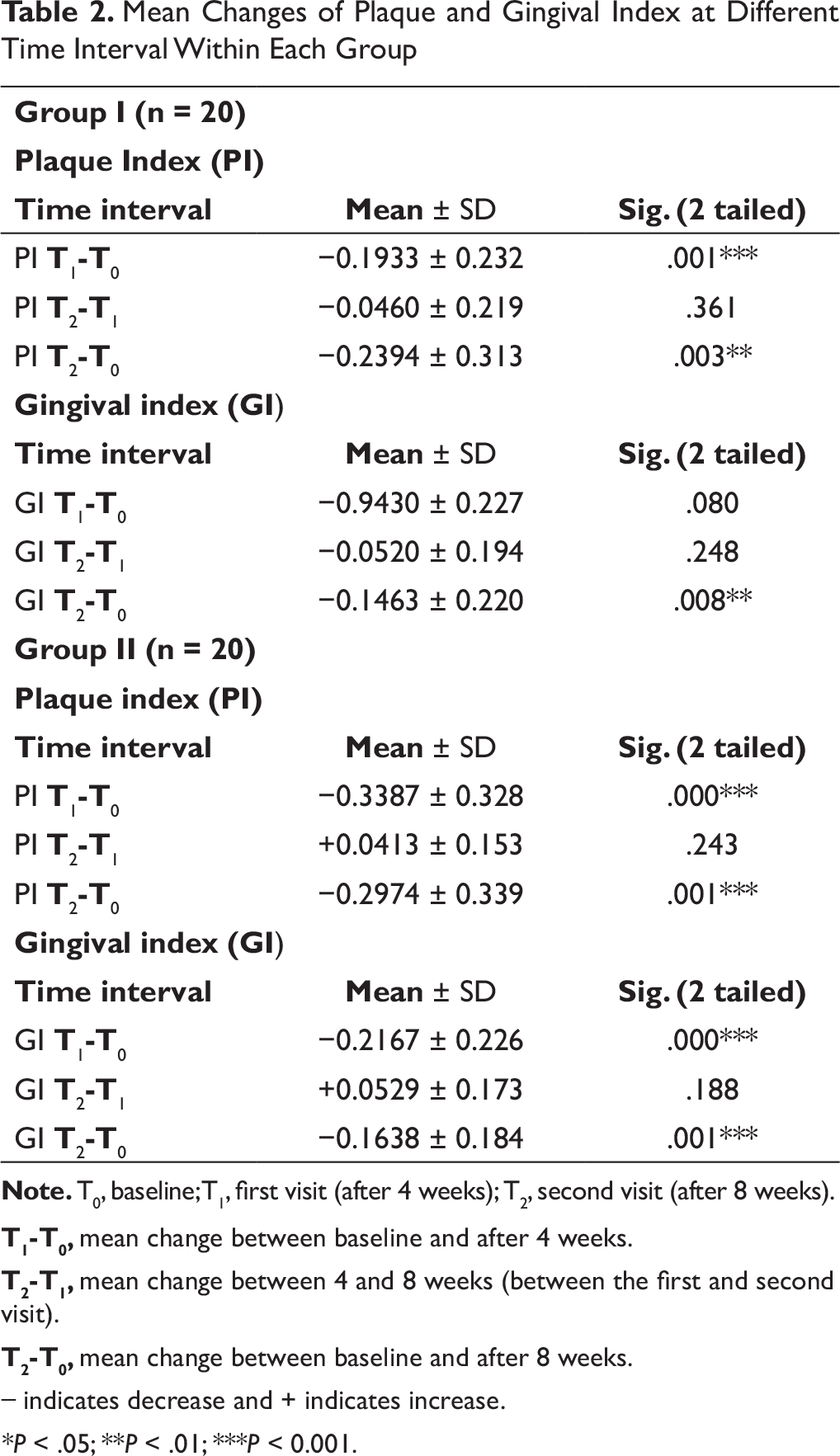
T1-T0, mean change between baseline and after 4 weeks.
T2-T1, mean change between 4 and 8 weeks (between the first and second visit).
T2-T0, mean change between baseline and after 8 weeks.
*P < .05; **P < .01; ***P < 0.001.
Intergroup comparison (Table 1) showed significant reduction of PI at 4 weeks in Group II than in Group I, with no significant difference at 8 weeks. This could be attributed to the effect of professional prophylaxis, which thoroughly removed plaque and debris in Group II. Thus, reinforcement of OHIs made patients in Group I more compliant to maintain oral hygiene, resulting in similar PI at 8 weeks. Furthermore, GI was not significantly different between the 2 groups at both visits, suggesting the role of repeated OHIs.
Group comparison (Table 2) showed that Group I, which received OHIs only, showed highly significant decrease of PI at the first visit, which was after 4 weeks, and significant decrease at the second visit. This is in accordance with many studies.1, 17, 40, 41 GI, on the other hand, showed no statistically significant decrease at 4 weeks, but at 8 weeks, it reached a statistically significant level. Possible explanation for no significant decrease in GI in Group I at 4 weeks could be that the gingival inflammation takes time to resolve as patient gradually adopts the oral hygiene regime.
Group II, which received professional tooth cleaning in addition to OHI, showed a very highly significant decrease in both PI and GI score at the first visit as well as second visit. The plausible explanation for a significant decrease in both the indices could be nonreliance on patient compliance as professional prophylaxis helped in removal of plaque and debris. Furthermore, reinforcement of OHIs added to the level of results obtained.
These results are in accordance with the study by Huber et al who showed that monthly OHI was effective in significantly reducing the visible plaque and gingival accumulation, and monthly rubber cup prophylaxis had a negligible effect on the plaque scores as well as gingival health. 20 However, he found that monthly rubber cup prophylaxis had a significant effect in reducing the gingival migration, which, however, was not examined in our study.
The results of this study revealed that a comprehensive oral hygiene program resulted in significant improvement in plaque control and gingival health irrespective of professional tooth cleaning. Similar studies found no therapeutic effect of dental prophylaxis for the prevention of gingivitis. 42 Zimmer in 2004 showed that initial prophylaxis consisting of patient motivation, instructions in oral hygiene and oral hygiene checkups is sufficient in most of the patients, and extended prophylaxis (regular mechanical professional tooth cleaning) prevents decalcification only in the high-risk group. 43 This study shows that professional prophylaxis need not be included as a mandatory step in the oral hygiene regime, rather comprehensive OHIs along with its reinforcement is the key to good oral hygiene of orthodontic patients wearing multibracket appliances. However, for some patients in whom compliance for some reasons remains a problem, professional prophylaxis should be included. This could result in saving of resources in terms of time and money.
Conclusions
A comprehensive OHI program with or without professional prophylaxis can lead to efficient control of plaque accumulation as well as improvement in the gingival health in patients with fixed orthodontic appliances. However, the need for professional tooth cleaning should be based on individual plaque control needs.
As orthodontists and their staff play a key role in guiding patients to perform proper oral hygiene frequently and effectively, with this study we hope to encourage orthodontists to incorporate effective oral hygiene programs and their reinforcement as an integral part of the orthodontic treatment protocol.
Footnotes
Acknowledgment
We would like to thank Dr Dinesh Walia, Associate Professor, Department of Community Medicine, Government Medical College and Hospital, Chandigarh for carrying out the statistical analysis for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.