
Abstract
Aim:
To compare the effect of mylar strip and glycerin topical application on the surface roughness of composite, compomer, and carbomer during polymerization.
Materials and Method:
Each of 45 disc-shaped specimens of Z250, Dyract, Carbomer, were prepared according to manufacturer’s instructions and molded in silicone rubber molds by one operator (5 mm diameter × 2 mm thickness; n = 135). Each restorative group was divided into 3 groups as oxygen group (control), mylar strip, and glycerin group (n = 15). In the control group, specimens were light cured in the open air for 40 s, whereas in the test groups they were covered either with a mylar strip or a drop of glycerin solution and cured for 40 s. Glycerin was rinsed off before polishing. Sof-Lex discs were used for polishing before the surface roughness measurements by a profilometer. The obtained data were statistically analyzed using two-way analysis of variance at a confidence level of 95% (P < .05).
Results:
The mean surface roughness values of composite, compomer, and carbomer polymerized in air, through mylar strip and glycerin showed no statistically significant difference (P > .05).
Conclusion:
Mylar strip and glycerin application did not affect the surface roughness of the composite, compomer, and carbomer. Polishing may mask the effect of different curing conditions.
Introduction
Resin-based dental restorative materials have evolved over the course of time due to increasing demands on both esthetics and mechanical properties. In pediatric dentistry, compomers, composite resins are frequently preferred for primary teeth restorations with adhesive systems to comply with clinical success requirements. 1 However, in pediatric practice, glass ionomer cements still maintain their vital role due to their remineralization effect on demineralized carious tissue.2-4 A decade ago, nanofillers were integrated into glass ionomer cements and a new restoration material carbomer was developed. It was claimed to remineralize hydroxy apatite and form flouroapatite crystals. 5
Despite all the progress in resin-based restorative materials, the polymerization stage poses a problem due to interference of oxygen in the air causing oxygen inhibition layer. This resin-rich uncured layer disrupts the surface texture leading to a porous and weak structure that affects the marginal adaptation as well. Researches have demonstrated that the removal of residual monomers can be accomplished by finishing and polishing. However, this might not eliminate this layer completely and remnants would affect the quality of the restoration adversely.
Hence, complete removal of oxygen inhibition layer has been in the interest scope of researchers and different techniques have been developed and tested and are still being investigated.6-9 One of the most recommended techniques is curing of the resin-based restorative material through a mylar strip to avoid air exposition. This is easy to apply for interproximal restorations but in clinical situation occlusal surfaces are hard to cope with. 9 Lately, topical application of glycerin was investigated to be used on occlusal surfaces and marginal of indirect restorations both in solution and gel form and the results are promising.9-10 Up-to-date curing through these two techniques has been tested; however, mostly surface hardness and marginal adaptation have been examined on different resin-based materials. Yet its effect on surface roughness has not been investigated.
Since, the surface roughness of restoration plays an important role in retention of plaque and change in oral microbiota, the purpose of the present study was to compare the effect of mylar strip and glycerin topical application on the surface roughness of composite, compomer, and carbomer.
Materials and Methods
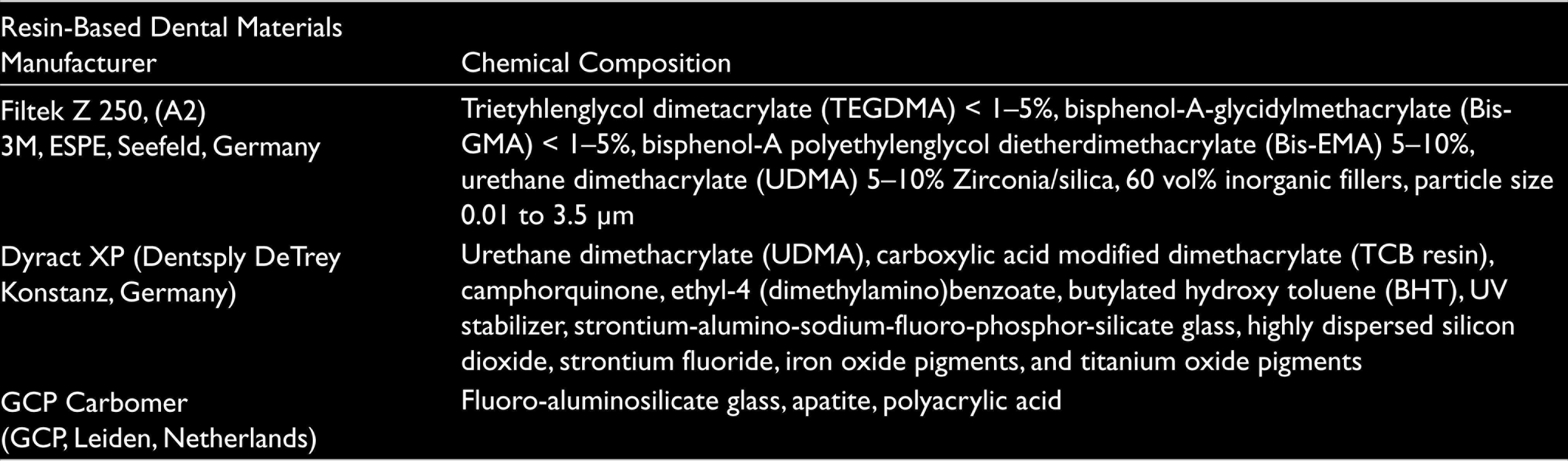
This study was designed as an in vitro research. A2 shades of universal hybrid composite Z-250 (3M ESPE, Seefeld, Germany), a compomer (Dyract XP, Dentsply De Trey, Konstanz, Germany), and carbomer (GCP, Leiden, Netherlands) were prepared as tested materials. The chemical compositions of these materials are listed in Table 1.
Chemical Composition of Restorative Materials
For this purpose, one operator completed the specimen preparations in one week.
Each of 45 disc-shaped specimens of Z250, Dyract, and carbomer were prepared according to the manufacturer’s instructions and molded in silicone rubber molds (5 mm diameter × 2 mm thickness; n = 135). The molds were placed on flat glass plates on top of mylar strips and filled with tested restorative materials. The material was gently pressed with another glass plate against the mold to extrude excess material. Each restorative group was polymerized under different curing conditions. Hence, they were divided into 3 groups as control, mylar strip, and glycerin group (n = 15).
In the control group: Specimens were light cured in the open air for 40 s.
In mylar strip group: All specimens were covered with a mylar strip and cured for 40 s.
In the glycerin group: All specimens were covered with a drop of glycerin and then cured for 40 s. Glycerin was rinsed off before polishing.
A LED Elipar Freelight 2 (3M ESPE, Germany) with a wavelength of 430-480 nm at a light intensity of 1200 mW/cm2 was used for polymerization of the composite and compomer. Carbomer was polymerized with Elipar S10 LED (3M ESPE, Seefeld, Germany) curing light in accordance with manufacturers recommendations. In all groups, the distance between the light source tip and the space was maintained at 1 mm. After curing, all specimens were rinsed with water and dried naturally. 4 grades of Sof-Lex discs (rough, medium, fine, and ultra-fine, 3M ESPE, St. Paul, USA) were used for polishing before the surface roughness measurements.
The surface roughness (Ra) was measured by a profilometer (MarSurf PS 10, Czech Republic), and measurements were recorded for each restorative material that was cured through oxygen, mylar strip, and glycerin solution. 3 measurements were taken from 3 different points on the surface of each specimen. The average Ra was automatically determined using the graphical-centerline method with a cutoff of 80 µm according to the American Society of Magazine Editors (ASME) Standard Y14.36, 2002.
Statistical Analysis
The obtained data were statistically analyzed using twoway analysis of variance at a confidence level of 95% (P < .05) using SPSS Statistics 15 (IBM Corporation, USA). Then, pairwise test was used for multiple comparisons.
Results
The mean surface roughness values per restorative material are shown in Table 2. There was a statistically significant difference among the 3 materials. Composite resin demonstrated the lowest surface roughness value of 0.33 µm followed by the compomer with a value of 0.50 µm, whereas the carbomer had the highest surface roughness value of 0.64 µm (P = .00) cured under 3 different conditions.
Mean Surface Roughness Values of Composite, Compomer, and Carbomer Polymerized Under Three Different Curing Conditions Namely Oxygen, Mylar Strip, and Glycerin Groups
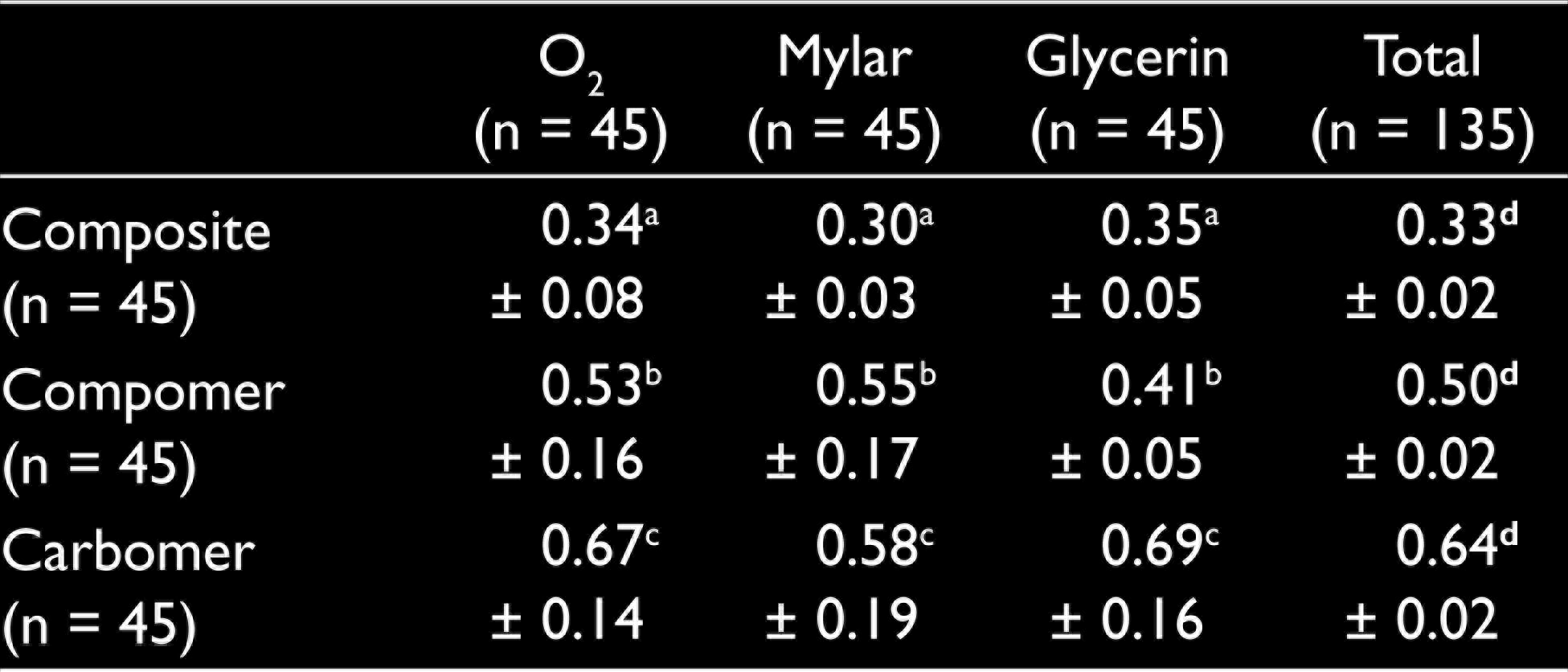
When curing conditions were compared for all 3 restorative materials, mean surface roughness values showed no statistically significant difference (P ˃ .05).
The mean surface roughness values of composite polymerized in air, through mylar strip and glycerin, were 0.34 µm, 0.30 µm, and 0.35 µm, respectively, and there was no statistically significant difference noted.
In the compomer group, surface roughness values were recorded as 0.53µm, 0.55µm, and 0.41µm, cured in air, through mylar strip and glycerin, respectively. No statistically significant difference was found among curing conditions. The carbomer group showed no difference among oxygen, mylar strip, and glycerin groups, where the values of surface roughness were 0.67 µm, 0.58 µm, and 0.69 µm.
Discussion
In pediatric dental practice, with the introduction of minimal invasive dentistry, resin-based restorative materials are the choice of clinicians for their high esthetics and mechanical properties. Despite these advantageous features, polymerization problems still remain a problem leading to shrinkage, weak wear resistance, and disruption in surface textures. One such cause of polymerization problem is the formation of the oxygen inhibition layer. Hence, the prevention of formation of the oxygen inhibition layer has been a challenge for researches. Mylar strips, use of helium gas, and topical application of glycerin have been investigated to eliminate the oxygen that yielded promising results.6-9, 10 In the dental literature, application of glycerin has been shown to improve the wear resistance of composite resins as well as marginal adaptation of adhesively luted composite inlays. 8 Microhardness was evaluated in most of the studies since it is an indirect method for evaluating the relative degree of the polymerization effect. 11 Surface roughness might be an alternative way of assessing the polymerization degree as well. Thus, the present study focused on evaluating the surface roughness after curing in air as the negative control group and through mylar strip and glycerin solution.
The degree of polymerization is influenced by parameters such as filler content, color, initiator, light intensity, and curing time.12-14 In the present study 3 different restorative materials, namely a hybrid composite, a polyacid modified composite resin, and a nanofiller integrated glass ionomer carbomer, were examined to see the effect of different curing conditions on surface roughness. The intensity of the LED and curing time was kept the same as in the aforementioned factors affecting the polymerization capacity.
The mean surface roughness of tested restorative materials varied based on their different chemical compositions. Composite had the lowest surface roughness followed by the compomer, and the highest values were reported for the carbomer group. However, curing conditions did not affect the surface roughness of the composite, compomer, and carbomer. In the present study, following polymerization of all the specimens through 3 different curing conditions, polishing was completed. Thereafter, surface roughness measurements were recorded. The use of a mylar strip and the application of glycerin did not affect the mean surface roughness values which may be due to the polishing of the specimens prior to surface roughness measurements. Our results are in line with the study of Park et al which demonstrated that microhardness of the composite resin did not differ after curing in air, through mylar strip and glycerin because the specimens were polished prior to microhardness measurements. 7
Polishing is strongly recommended after resin-based restoration polymerizations to remove the residual monomer and have a higher quality of surface. Increase in the surface roughness of dental materials encourages plaque retention. The critical mean surface roughness for adhesion and colonization of bacteria has been reported to be 0.2 µm. In order to optimize the longevity of restorations and esthetics, surface roughness should be minimized by polishing. A sequence of abrasive particles from coarse grit gradually decreasing toward fine grit is recommended as an ideal polishing protocol. 15 In the present study, 4 grades of Sof-Lex polishing disc system were used.
The present study was an in vitro design research; hence, oral cavity conditions are not mimicked. The presence of saliva and the temperature of the oral cavity are not reflected on the given results. Within the limitations of this study, it was concluded that the mylar strip and glycerin application did not affect the surface roughness of the composite, compomer, and carbomer. Polishing still remains adequate for the removal of uncured resins and corrects the surface texture of resin-based restorations. Further studies both in situ and in vivo are required to conclude about the effects of different curing regimens to different restorative materials to elevate the clinical success rates.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. Research Lab of Istanbul Aydin University Dental Faculty was used for the surface roughness measurements.