
Abstract
Objectives:
Immediate post-operative reconstruction of calvarial bone by cranioplasty prosthesis in calvarial bone fibrous dysplasia. An easy and economical method for reconstruction of the defect.
Methods:
Surgical excision of right parietal cranial space occupied lesion was performed followed by fabrication of immediate postoperative period cranioplasty prosthesis by using clear heat polymerized polymethylmethacrylate.
Results:
The cranial defect created during excision of calvarial bone fibrous dysplasia was immediately replaced by cranioplasty prosthesis which was fabricated in the immediate post-operative period using heat polymethylmethacrylate.
Conclusions:
Polymethylmethacrylate is a very reliable thermoplastic material that can be prefabricated or even placed immediately after post-operative period to produce a suitable prosthesis. Polymethylmethacrylate implants have been outmoded by computer-aided design and computer-aided manufacturing and newer 3-dimensional printed implants, but these newer methods are accompanied by higher expenses and timing issues.
Keywords
Introduction
Cranioplasty is a procedure of surgical restoration of congenital defects or acquired defects of the cranium, commonly after performing a craniotomy or craniectomy. The main indications for cranioplasty are for anatomical reconstruction, brain protection, and cosmetics. Other significant indications for cranioplasty are epilepsy, calvarial bone fibrous dysplasia, neurological disorders, and changes in cerebrospinal fluid dynamics. Cranioplasty is still a challenge because of the difficulties in exactly defining and reestablishing the bony defect. 1 Lots of replacement materials have been used for cranial prosthesis such as bone, auto/allografts, distinct biomaterials, and osteoinductive growth factors. Historically, it has been documented that gold plates were used for cranioplasty in the past. With a complex range of possibilities, the ideal synthetic material should be biocompatible, inert, nonthermal conducting, radio-transparent, nonmagnetic, lightweight, rigid, simple to prepare, easily applicable, and inexpensive. Polymethylmethacrylate (PMMA) is one of the inert materials which best meets most of these requirements. Strength-wise, PMMA is nearly equivalent to a bone and has better compression and stress resistance than hydroxyapatite. Furthermore, PMMA was shown to adhere to the dura mater without any reaction with the underlying tissue. 2 PMMA can be used in two forms: self-polymerizing and heat polymerizing. One of the advantages of self-polymerizing PMMA is that it can be molded intraoperative or prefabricated into the shape of the cranial defect. On the other hand, its disadvantage is heat production during polymerization reaction and possible release of a monomer that can be carcinogenic. In the present case, heat-polymerizing PMMA was used to overcome these disadvantages. The main advantage of alloplastic materials is that it is possible to fabricate the prosthesis within a short time. Thus, reducing operation time and complexity, and improving the final result. The purpose of this article is to describe a technique to fabricate heat-polymerizing PMMA prostheses by using an original resected diseased bone, within 48 hours of surgery. Also, we intend to demonstrate that these prostheses are relatively nonexpensive, and cosmetically and functionally acceptable alternatives to more expensive and complex 3-dimensional printed bone prostheses.1-3
Case Report
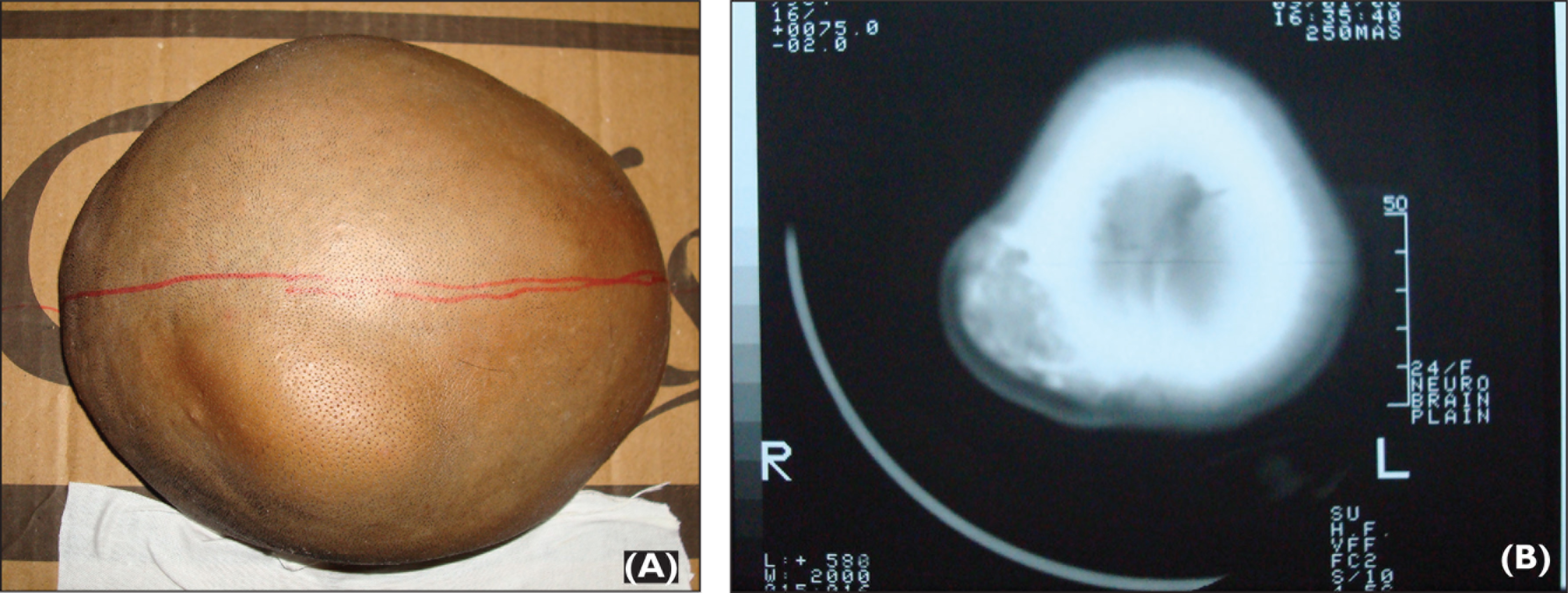
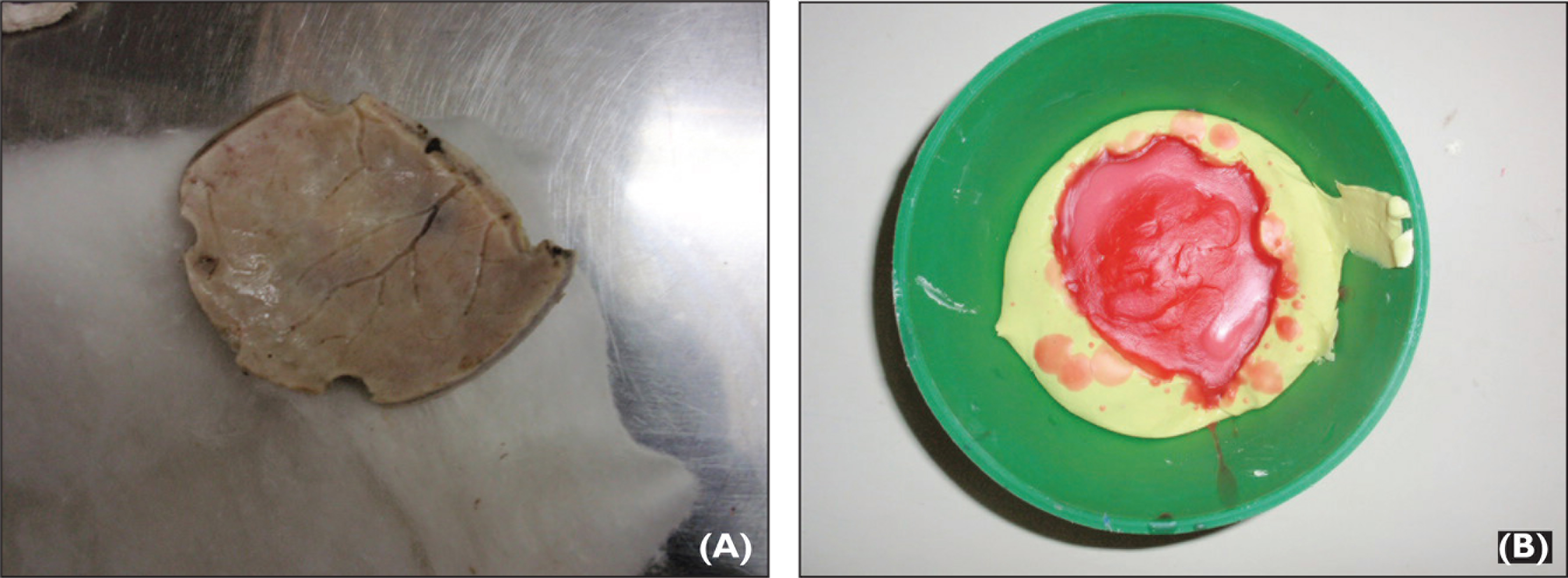
A 24-year-old female patient presented with a chief complaint of swelling in the right back region of the head since 5 years. According to the patient the swelling was asymptomatic and gradually increased to the present size. On inspection, swelling was found to be oval in shape, approximately 3.5 × 4 cm in diameter, and located in the parieto-temporal region (Figure 1A). On palpation it was hard in consistency and fixed to the underlying structures. Computed tomography scan of the brain-plain study revealed expansile intramedullary lesion with sclerotic and lucent areas (ground glass appearance) in parietal bone, suggestive of calvarial bone fibrous dysplasia (Figure 1B). Surgical excision of a lesion affecting the right parietal cranial bone was performed without any complications followed by immediate postoperative period cranioplasty prosthesis using clear heat-polymerized poly (methyl methacrylate). Soon after the surgery, performed by a neurosurgeon, a leaf-shaped sectioned bone of dimensions around 8 × 6 cm (Figure 2A) was sent to us for fabrication of cranioplasty prosthesis.
(A) Swelling in the Right Parietal Region of the Head and (B) Computed Tomographic Images Reveling Expansile Intramedullary Lesion With Sclerotic and Lucent Areas in Right Parietal Region.
(A) Resected Bone and (B) Molten Wax Poured in the Impression of Resected Bone.
Procedure for Fabrication of Cranioplasty Prosthesis
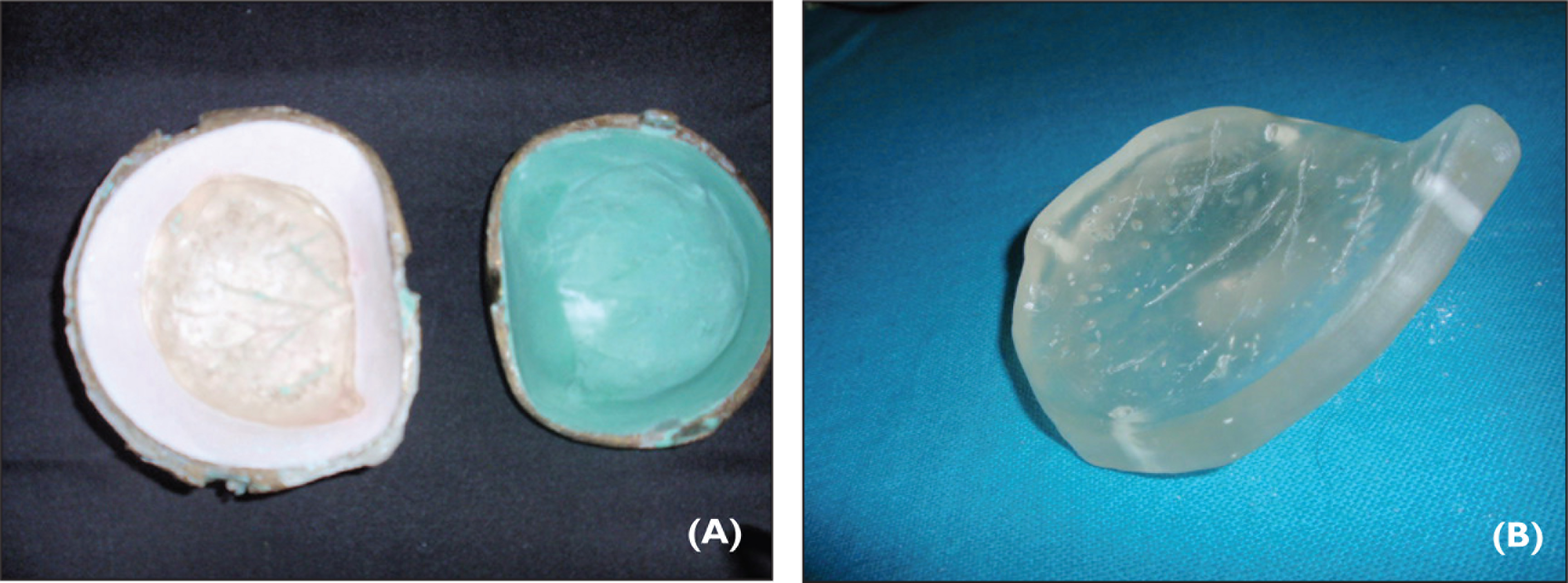
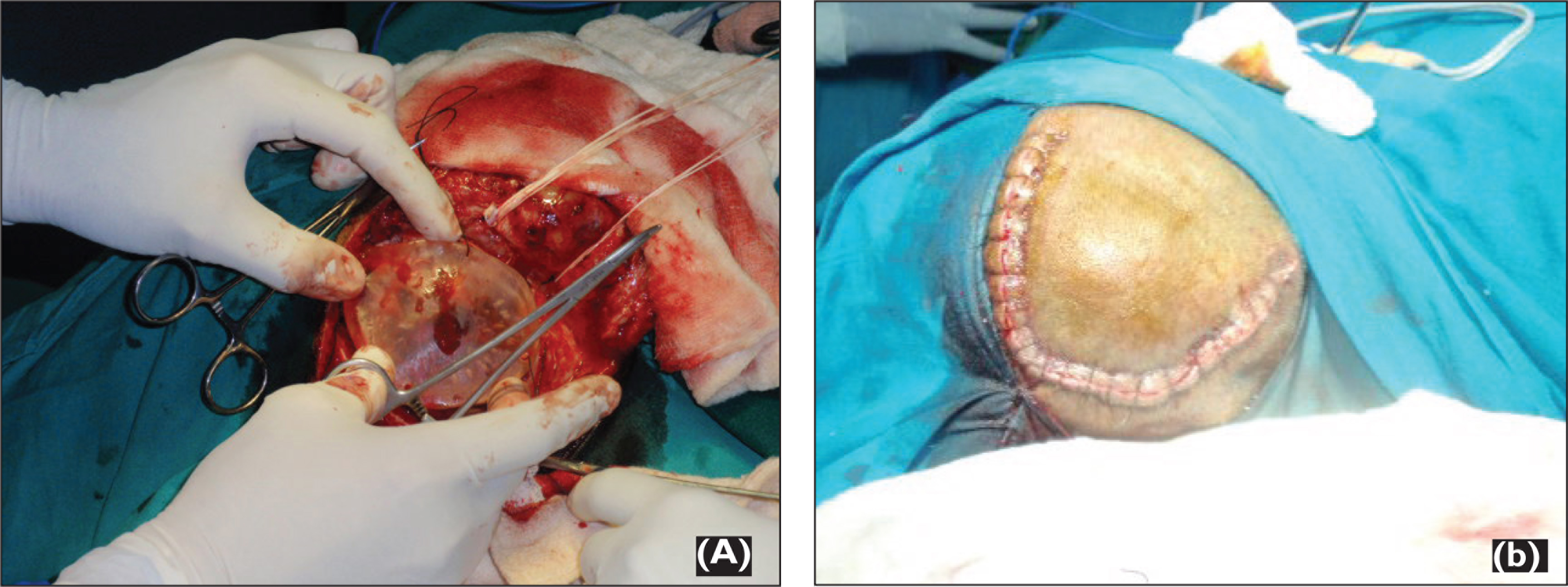
As the contour of the inner surface of the sectioned bone was undisturbed by the disease, it was duplicated using irreversible hydrocolloid impression material. The imp-ression was immersed in Korsolex Rapid (Raman & Well Pvt. Ltd, Bombay, India) for 10 minutes for sterilization. Modeling wax was melted and poured into the impression to make a positive replica of the bone (Figure 2B). Immediately after taking impression, the sectioned bone was sent for histopathological investigation. The trephine holes in the wax pattern were then filled with wax and contoured. The outer surface of the wax pattern was properly contoured maintaining the thickness of the walls and to restore the normal anatomy and appearance. Wax pattern was then invested in a conventional manner and processed using clear heat-polymerized poly (methyl methacrylate) resin at 168 F for 12 hours (Figure 3A). A long curing cycle was selected to reduce the residual monomer content of the cured prosthesis. After curing cycle, the prosthesis was boiled for 30 minutes to ensure the elimination of all free monomers. The prosthesis was deflasked after bench cooling and polished. Four holes of 2 mm diameter were then made at the edge of the prosthesis to position it (Figure 3B). Sterilization of the prosthesis was performed, and after 48 hours of the surgery sutures were cut at the surgical site and prosthesis was placed into the resected site and inspected. Adjustments were made to fit the prosthesis as closely as possible. Fixation to the skull was accomplished by aligning the corresponding holes at the edge of the prosthesis with the borders of the surrounding bones at four points, and it was secured using sutures (Figures 4A and B). Histopathology investigations confirmed the calvarial bone fibrous dysplasia. Post-operative healing was uneventful and follow-up did not record any clinical signs suspicious of foreign body reaction to PMMA material. In terms of functional and esthetic results the case was successfully treated.
(A) Acrylized Cranioplasty Prosthesis in the Dental Flask and (B) Finished Prosthesis With 2 mm Diameter Holes to Secure It into Position.
(A) Securing Cranioplasty Prosthesis to Final Position Using Sutures and (B) Final Countour After Skin Suture.
Discussion
Cranioplasty is a commonly performed operation in the field of neurosurgery. It is the surgical involvement to repair cranial defects in both cosmetic and functional ways. 3 Methods of cranioplasty have developed from using autogenous materials to alloplastic materials; the most widely used is PMMA or a combination of PMMA with titanium or wire mesh. 4 In the present study, we used PMMA but did not use titanium or wire mesh to reduce infection and cost. Autogenous bone grafts are not commonly indicated because of complications such as absorption and loss of contour.3-5 Alloplastic implants are considered imperative as they are readily available, simple to handle, and display minimal resorption after following the cranioplasty procedure. 6 Alloplastic implant materials used for cranial prosthesis are metals, self-polymerizing and heat-polymerizing methacrylate, silicone, and poly-ethylene. Metals such as tantalum, titanium, austenite stainless steel, and vitallium display the benefit of being hard, malleable, and easily available, but their high thermal conductivity may precipitate headaches and other neurological symptoms. 7 Silicones and polyethylene are tissue compatible but their flexibility compromises pro-tection in cranial defects. 5 Self-polymerizing acrylic resin is less inert, strong, and has poor thermal and electrical conductivity. One major disadvantage of using self-cure PMMA includes increased heat generation during a polymerizing reaction which could cause harm to the underlying tissues and release bits of residual monomers that have been reported to be carcinogenic. 8
Heat-polymerizing acrylic resins overcome the disadvantages of self-polymerizing acrylic resins and are stronger, rigid, more inert with good reproduction of contours. 9 This is the reason we had selected heat-polymerizing PMMM as a material of choice for the present case. Release of residual monomer content in the heat-polymerized resin could be decreased by the use of long curing cycle, water bath, and microwave post-polymerization.10-11 In the current case, the disadvantage of residual monomers in heat-cured PMMA was addressed by long curing cycle and preparation before implantation.
Although newer techniques such as computer-aided design and computer-aided manufacturing (CAD CAM) generated cranial prostheses or titanium plates and 3-dimensional printing prosthesis can give anticipated result, however, the high cost of these prostheses makes their use rare in the patients. In the present case, we had explained all possible treatment plans to the patient, but she refused CAD CAM generated cranial prostheses or other recent techniques due to economic reasons. The main purpose of immediate postoperative fabrication of cranioplasty is to achieve good cosmetic results as well as to provide aid to psychological hitches. Usually the waiting period between initial surgery and the cranioplasty procedure ranges from 2 to 3 months, but in conditions of trauma, aneurysms, and certain tumors, the waiting time is as much as 1 year following an infective process. 12 The advantages of immediate postoperative period cranioplasty procedure are to provide adequate time for fabrication of a reasonably precise, and well-fitting prosthesis that can be properly shaped, polymerized, perforated, and polished. The major advantage of immediate postoperative period cranioplasty is to limit morbidity for the patient. The prosthesis was placed after opening the sutures on second postoperative day before any healing process could began and wound was resutured at the same time. The fabrication of cranioplasty prosthesis during the surgery by using autopolymerizing resin can be done, but it has disadvantages of exothermic reaction and excess of monomer leach out. To avoid these problems heat-polymerizing resin was used in the current case. After surgical reconstruction of the cranial defect, the patient was called for regular follow-up visits. The cosmetic result of surgical reconstruction with clear heat-polymerized poly (methyl methacrylate) was satisfactory.
Conclusion
Fabrication of cranial prosthesis immediately after the postoperative period with PMMA is an excellent option to enhance the cosmetic effect. It also restores the cranial defect and gives advantages of psychological and social performance. Also, immediate postoperative loading of cranial prosthesis reduces the morbidity rate for the patient. The use of impression materials to duplicate the patient’s excised bone is a cheap and safe way to rebuild the cranium if time and budget are important limitations. Infection, being the most feared complication of allograft implants, has a very low rate with the procedure explained in the present article. The advantages of cranioplasty on neurologic function have also been proved by many researches in the literature. This technique has proven to be harmless and has produced excellent results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.