
Abstract
Tension pneumocephalus (TP) can be a life-threatening postoperative complication, but there are limited data owing to its exceedingly low frequency. A 48-year-old man that suffered a head injury survived the acute phase and cranioplasty was performed using a titanium plate. Progressive deterioration of consciousness occurred the day after the cranioplasty. Computed tomography showed the presence of expanded air in the left epidural cavity and a midline shift to the right side. Emergency skin flap reopening was performed. Tension of the scalp decreased when the skin suture was cut and the wound reopened. Lucidity and improved right hemiparesis were obtained within a few hours after drain insertion. Pooled air in the left epidural cavity gradually dissipated postoperatively and the epidural drain was removed 2 days after insertion. The patient was discharged 27 days after cranioplasty, with a modified Rankin scale score of 2. The mechanism that caused TP was considered. Specifically, the skin flap acted as a one-way valve and trapped air. Then the trapped air expanded as the patient’s body temperature warmed. TP should be considered a differential diagnosis after craniotomy. Emergency skin flap reopening and drain insertion may be an effective treatment for TP in the epidural space.
Introduction
Tension pneumocephalus (TP) can be a life-threatening postoperative complication, but there is a paucity of data owing to its exceedingly low frequency.1–3 TP sometimes occurs in low cerebrospinal fluid (CSF) pressure situations, such as with CSF leakage owing to trauma or ventriculoperitoneal (VP) shunts.4–9 A previous study reported TP following cranioplasty in a shunted patient. 2 This current case report describes a patient with TP following cranioplasty without a cause of low CSF pressure.
Case report
In August 2020, 48-year-old man fell off a stepladder and suffered a right skull fracture, right epidural haematoma, left subdural hematoma and left frontal lobe contusion (Figures 1a and 1b). Left decompressive craniectomy was performed the same day in the Department of Neurosurgery, Osaka University Hospital, Osaka, Japan. The patient survived the acute phase (Figures 1c and 1d) and cranioplasty was performed using a custom-made titanium plate (Craniofit-Ti; HOYA Technosurgical Corporation, Tokyo, Japan) in the Department of Neurosurgery, National Hospital Organization Osaka National Hospital, Osaka, Japan 50 days after the injury. No drains were placed at the end of the cranioplasty operation. The day after the cranioplasty, progressive deterioration of consciousness (the Glasgow coma scale score deteriorated from 15 to 13) and right hemiparesis appeared with elevated body temperature ranging from the upper 37s °C to 39.0 °C. Tension of the scalp over the titanium plate was high. Computed Tomography (CT) showed the presence of expanded air in the left epidural cavity and midline shift to the right side (Figures 2a and 2b). Emergency skin flap reopening and epidural drain insertion from the space between the custom-made titanium plate and the skull edge was performed (Figure 2c). The tension of the scalp was decreased when skin suture was cut and the wound reopened. Lucidity and improved right hemiparesis were obtained within a few hours after drain insertion. The pooled air in the left epidural cavity gradually dissipated postoperatively and the epidural drain was removed 2 days after insertion (Figures 2d and 2e). The patient was discharged 27 days after the cranioplasty, with a modified Rankin scale score of 2 (Figure 2f).

Computed tomography (CT) images before cranioplasty in a 48-year-old man that fell off a stepladder and suffered a right skull fracture, right epidural haematoma, left subdural hematoma and left frontal lobe contusion: (a) CT in the emergency room (ER) showing a right epidural haematoma, left subdural haematoma and left frontal lobe contusion; (b) three-dimensional CT image in the ER showing a right temporal bone fracture (arrow); (c, d) CT images just before cranioplasty.
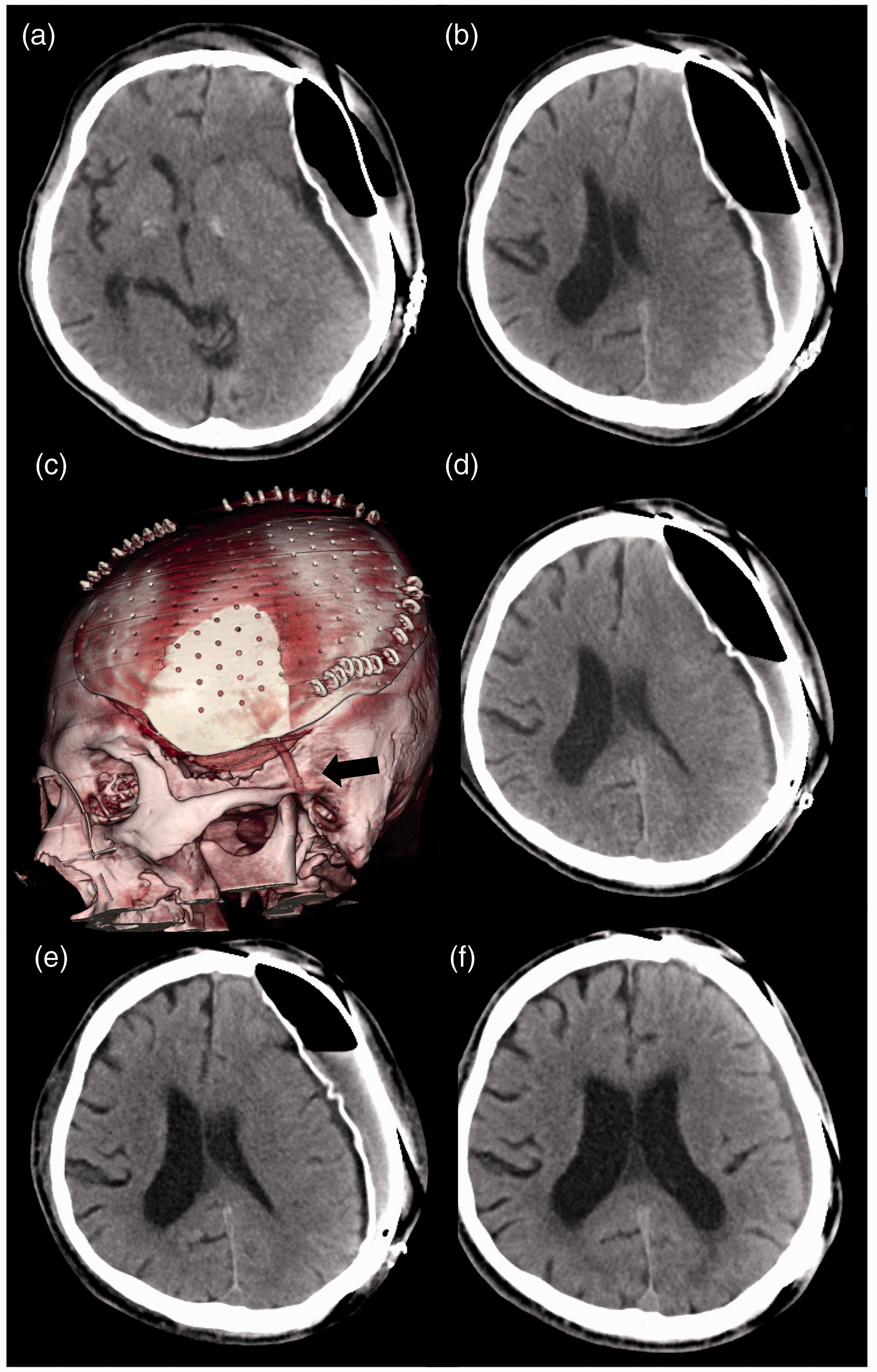
Time-course of the computed tomography (CT) images after cranioplasty in a 48-year-old man that fell off a stepladder and suffered a right skull fracture, right epidural haematoma, left subdural hematoma and left frontal lobe contusion: (a, b) CT images the day after the cranioplasty showing distended air in the subgaleal and epidural spaces displacing the brain to the right side; (c) three-dimensional CT image after emergency epidural drain insertion (the arrow indicates the epidural drain); (d) CT image the day after emergency epidural drain insertion; (e) CT image 2 days after emergency epidural drain insertion; (f) CT image at discharge. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
This current case report describes a rare patient with TP in the epidural space following cranioplasty with a custom-made titanium plate that was resolved after emergency skin flap re-opening and epidural drain insertion.
Retention of air in the cranial cavity, pneumocephalus, is common after intracranial surgery. Usually, the air is absorbed and causes no neurological symptoms, but fairly infrequently, the air is trapped and causes increased intracranial pressure (TP).1,2,10 Several mechanisms explaining TP have been proposed.11–14 The first mechanism is the presence of a promoting factor drawing air into the intracranial space by decreasing the CSF pressure, such as a VP shunt or CSF leakage.4–9 The second mechanism is a one-way valve mechanism that permits air to enter but not to exit to the extracranial space.1,10,12A previous study reported that a dural defect could be a one-way valve after craniotomy. 12 A frontal sinus breach in decompressive craniectomy could act as a one-way valve and cause TP. 10 The present case did not undergo previous shunt insertion, had no CSF leakage and a one-way valve was not detected. A dural defect was excluded as the cause of the TP because the trapped air existed in the epidural space. A one-way valve in the frontal sinus was also excluded owing to the lack of an opening in the frontal sinus. Skin flaps could have acted as a one-way valve, but the probability was very small because no such defect drawing air into the epidural space was noticed perioperatively in the scar. However, a previous study reported that expanded air collected in the subgaleal and subdural space after cranioplasty. 2 Although no such injury was noticed, the authors presumed that a one-way valve existed in the scar tissue. 2 The third mechanism explaining TP is the theory that trapped air expansion occurs with warming of the patient’s body temperature.11,15 In a previous study, it was presumed that elevated body temperature caused dilatation of postoperative air in the aqueduct and resulted in neurological deterioration. 11 According to this theory, lowering the body temperature might be effective in the event of a slight worsening of neurological status due to pneumocephalus.
The treatment methods used for pneumocephalus vary according to the mechanism and location.6,12,13,16 The mainstay of conservative treatment is augmented oxygen delivery.16–19 By breathing 100% oxygen, nitrogen washout from the lungs hastens, facilitating the diffusion of the nitrogen in the intracranial bubble into the circulating blood following its gradient. 16 In most cases of TP, invasive treatment may be necessary. Emergency air decompression with needle aspiration or drain insertion may be effective in cases of TP in the epidural or subgaleal space. 2 In cases with shunts, shunt removal or adjusting the shunt to a high pressure setting may be required. 2 Epidural and/or subgaleal drain insertion at the end of the cranioplasty may be one of the effective techniques to prevent postoperative TP.
In conclusion, the present case report described a patient with TP in the epidural space following cranioplasty with a custom-made titanium plate. TP has the potential to become a life-threatening postoperative complication even without CSF leakage or shunts and should be considered a differential diagnosis after craniotomy. Emergency skin flap reopening and drain insertion may be an effective treatment for TP in the epidural space.
Footnotes
Acknowledgement
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant-in-Aid for Early-Career Scientists from the Japan Society for the Promotion of Science to Tomohiko Ozaki (no. 18K16582).