
Abstract
Aims and Objectives:
The high esthetic demands led to the promotion of various esthetic appliances like lingual orthodontics. This study aimed to review clinical outcome and potential complications of lingual orthodontics to achieve an evidence-based decision for orthodontic therapies.
Materials and Methods:
A comprehensive electronic search was conducted from January 1975 to March 2019 which was limited to English language and administrations of lingual orthodontics treatment which evaluated its efficacy and potential complications. Data extraction was performed according to the PRISMA statement.
Results:
49 studies were selected and analyzed in this systematic review. The pain of lingual appliances starts a little earlier and lasts longer, and patients with lingual appliances experience more tongue discomfort and less cheek and lip pain and greater eating difficulties especially after placement and take a longer time to adapt to appliances. Lingual appliances generally cause more plaque accumulation and gingivitis especially in lingual anterior teeth; however, labial appliances are associated with high frequency in posterior maxillary teeth.
Conclusion:
This systematic review shows that despite the drawbacks of these appliances such as pain and eating difficulties, they can accomplish treatment goals with the same outcomes in comparison with conventional approaches, within the same duration and even lesser anchorage loss.
Introduction
Malocclusion has important effects on smile, appearance, esthetic, socio-psychological aspects, and generally on the quality of life.1,2 In recent years, the demographics of ortho-dontic patients changed from children to adults, and the number of adults who want the orthodontic therapy increased significantly.3,4 Many adults who require orthodontic treatment refuse it due to conventional appliance appearance problems.5,6 This high esthetic demand of patients 7 led to the promotion of various esthetic appliances such as esthetic brackets, clear aligners, and lingual orthodontics. 8 Since the advent of lingual orthodontic in the 1970s, 9 the promotion has been seen in many aspects such as design manufacturing and mechanotherapy. Different studies have stated different advantages and disadvantages including lower noticeability, need for lighter forces due to smaller interbrackets distance, and better anchorage control as advantages,7,10-12 and more difficulties in the insertion and handling, longer chair times for patients and orthodontist, and higher laboratory costs as disadvantages. 8 By increasing the number of patients who want lingual treatment, orthodontists have a tendency toward lingual orthodontics. During the years, several case reports, reviews, and clinical research papers have discussed various aspects of lingual orthodontic treatment. However, a thorough systematic evaluation of clinical studies related to clinical outcomes of lingual orthodontic treatment is lacking from the literature.
Such a review will allow gathering the supporting evidence on this expanding treatment approach, will help clinicians to provide evidence-based treatment, and will provide recommendations for targeted future research in the field. The current study aimed to review clinical outcome and potential complications of lingual orthodontic in most recent evidence during the last 7 years.
Materials and Methods
Eligibility Criteria
We followed PRISMA guidelines 13 for systematic reviews. All in vitro studies and in vivo analysis, which administrated orthodontic treatments in ex vivo or in vivo investigations, were excluded. Clinical trials, case controls, abstracts, reviews, letters, and theses were included.
Any type of animal models (such as rats and primates) was excluded. Studied on female animals (nonovariectomized) and/or animals with other systemic variables (such as diabetic rats) were excluded. Only clinical investigations on human being were included.
Types of Interventions
Studies investigated that lingual orthodontic treatment on human were included. Studies which did not investigate the lingual approach or not related to this therapeutic modality were excluded.
Types of Outcome Measures
Complications must be reported by the experienced orthodontist or patients in questionnaire-based studies. Clinical parameters must be reported as the outcome of the intervention.
Information Sources
The MEDLINE (NCBI PubMed and PMC), Embase, EBSCO, Scopus, and Google scholar were the information sources. Moreover, a hand-search was done specifically in the following journals: Journal of Orthodontics, The Angle Orthodontist, British Dental Journal, American Journal of Orthodontics, and Dentofacial Orthopedics.
Search Strategy
An electronic search was conducted in PubMed from January 1975 to March 2019 limited to English language publications. Published papers on orthodontic treatment via lingual approach were found using the following keywords alone or ensemble: (“Orthodontics” [Mesh] OR “Orthodontic Appliances” [Mesh] OR “Dental Braces” [Mesh] OR “Orthodontic Wire” [Mesh]) AND (“Lingual”). In addition, manual search of the selected articles/bibliographies was done.
Study Selection and Data Extraction
Two independent reviewers retrieved studies according to the defined keywords. They also performed initial screening on titles and abstracts of the selected articles according to the pre-defined eligibility criteria. Disagreement between reviewers was resolved by discussion, and if it still remained, a third person’s consultation was referred to. After all, we reviewed all full texts in which all the authors were selected and confirmed. Data extraction was performed according to PRISMA statement.
Data Items
Data were summarized according to the following: (a) author and year of publication, (b) type of study, (c) method of assessment, (d) duration of follow-ups, (e) reported complication, and (F) outcomes of assessments.
Results
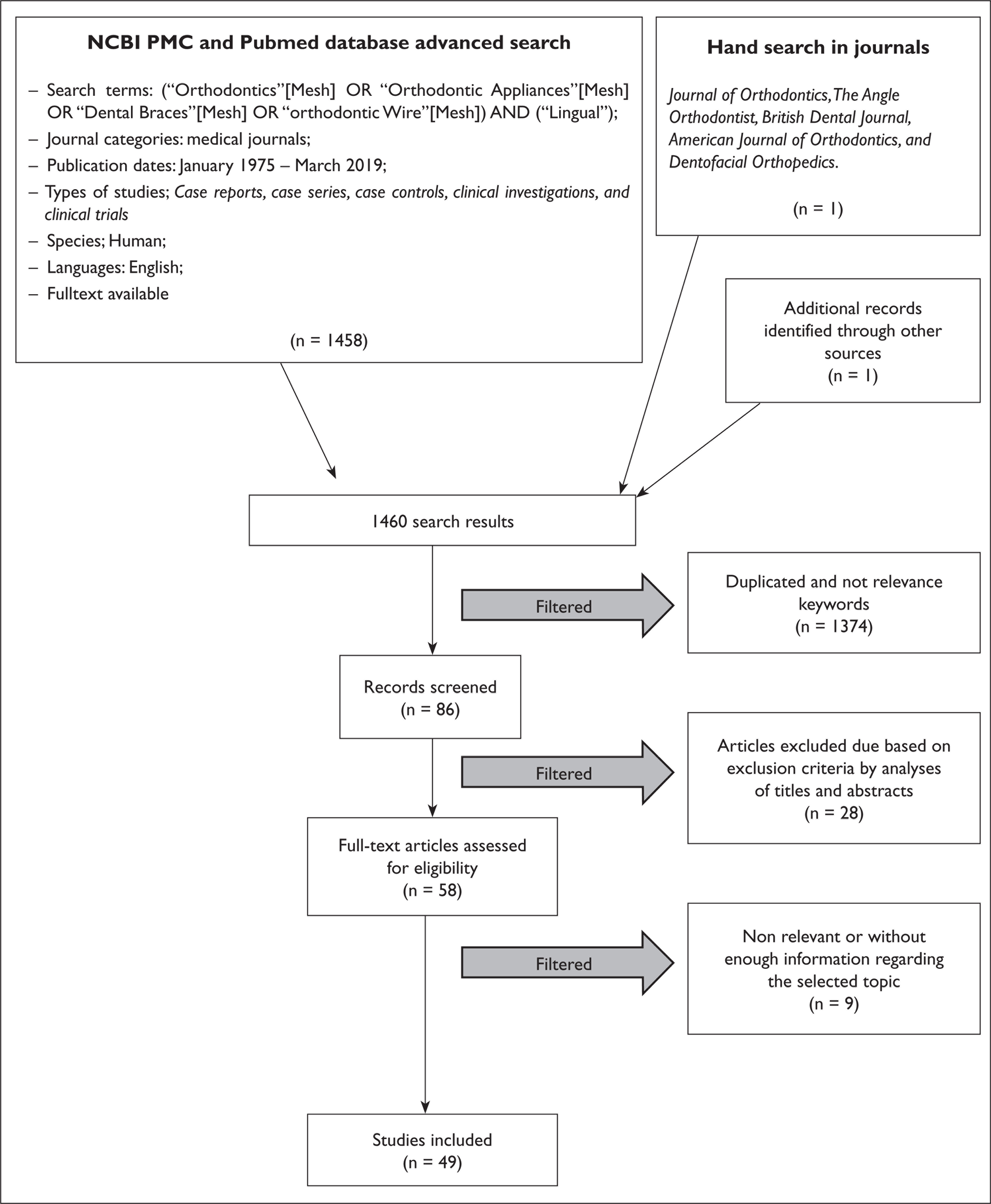
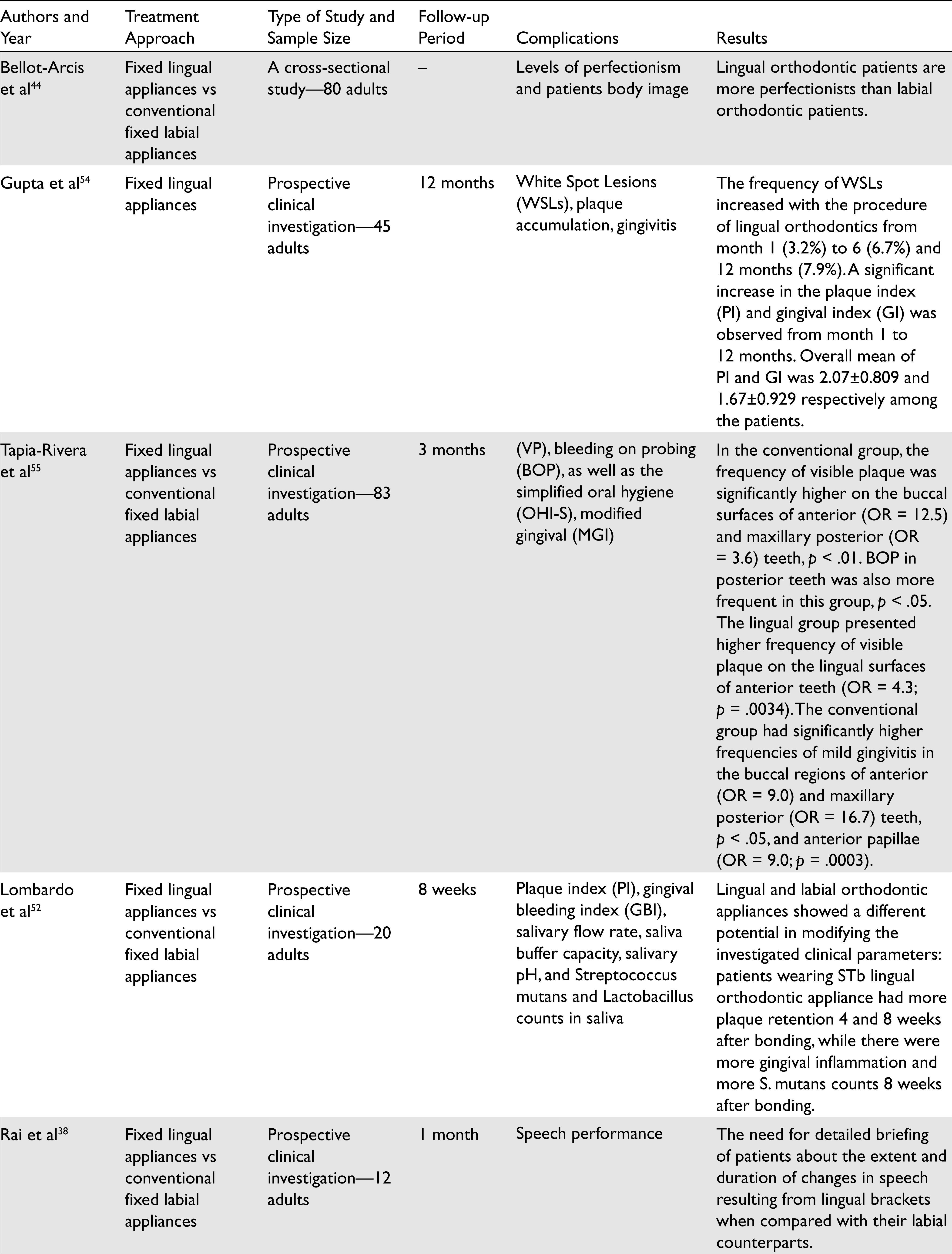
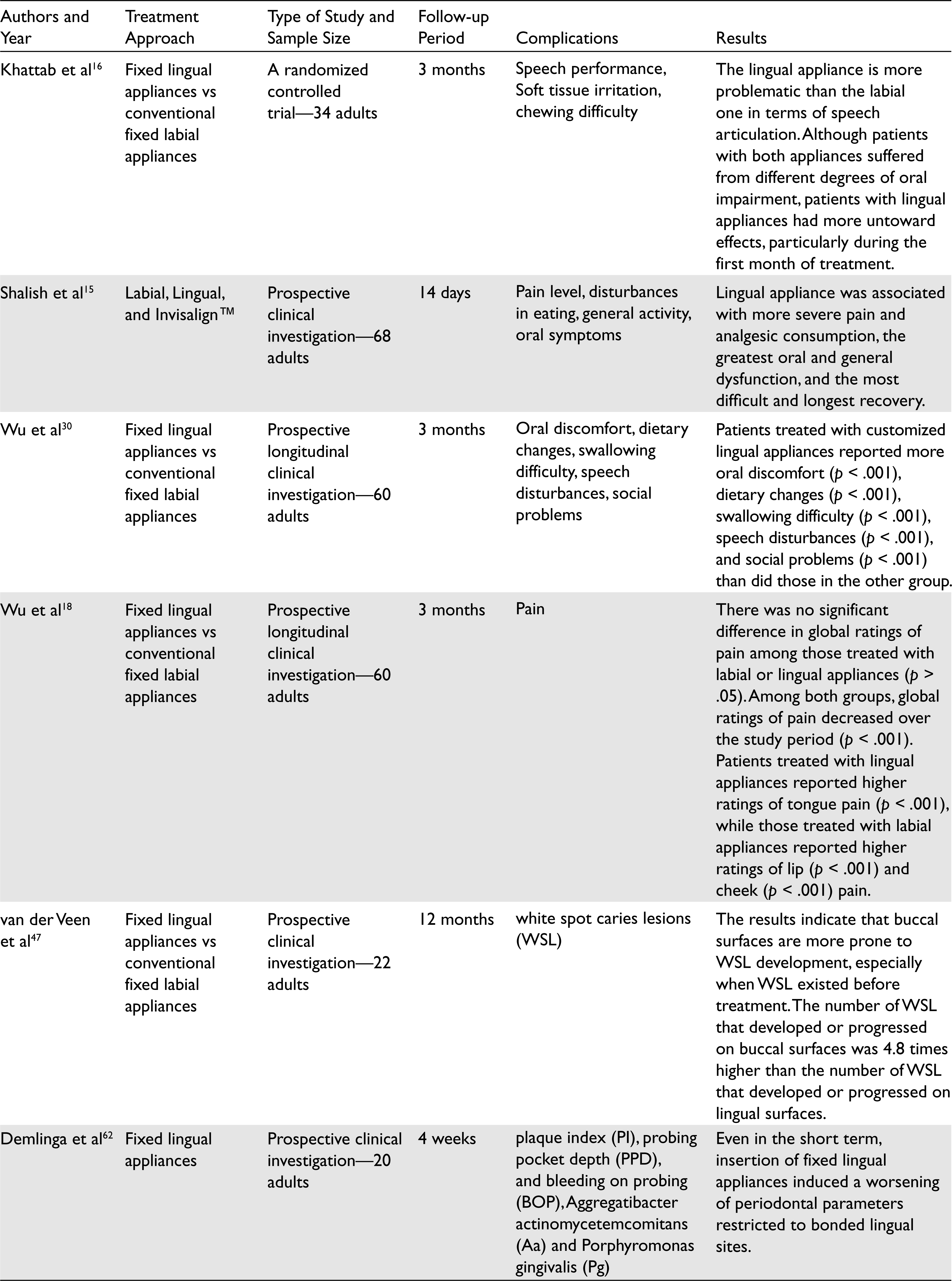
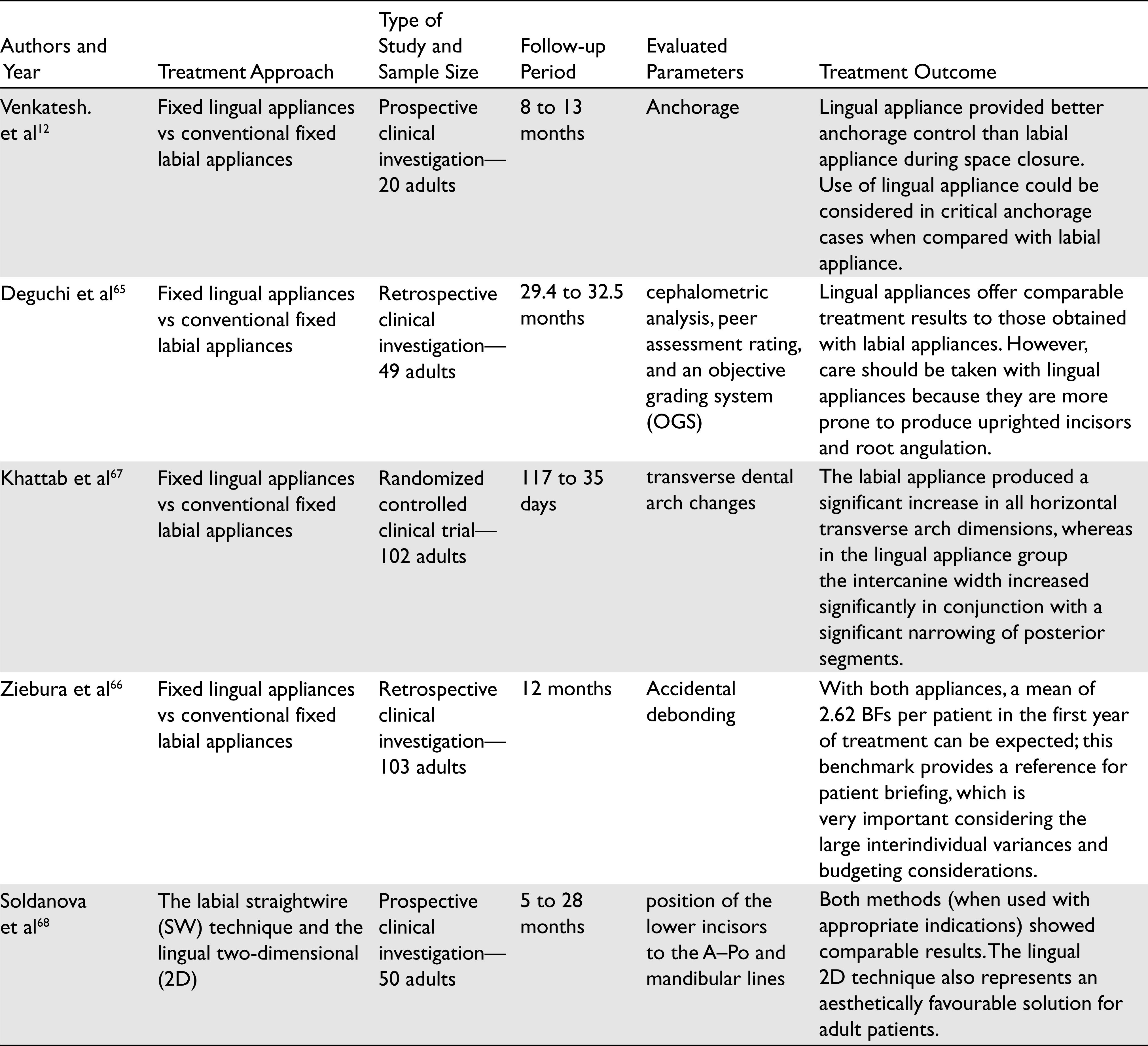
Figure 1 illustrated the PRISMA flow diagram of the search strategy used in this study. 1,458 articles were retrieved from the NCBI, PMC, and PubMed databases, and one article from other sources and one studies from hand-search. A total of 1,460 articles were initially screened by 2 independent reviewers and 1,374 studies were excluded due to duplication and unrelated keywords according to our study design. After exclusion of non-relevant articles, the full texts of 49 studies were included. 11 articles that published after January 2010 and investigated complications related to the lingual treatments are listed in Table 1. Table 2 represents treatment outcome in 5 articles during the same period.
Complications Related to the Lingual Orthodontic Treatment in the Most Recent Articles
Treatment Outcome of the Lingual Orthodontic Treatment in the Most Recent Articles
Discussion
Complications
Pain and Discomfort
Pain is a nonrecognized phenomenon that depends on many factors. There are different results regarding overall pain. Some studies show that lingual appliances have greater overall pain,8,14-16 while others state no significant difference.9,17,18 We must be reminded that pain is associated with many factors such as age, sex, personal value,19,20 malocclusion and skeletal characteristics, and arch shape and size. 4 The pain of lingual appliances starts a little earlier 21 and lasts longer. 14 Sites of pain are different and researches show that patients with lingual appliances experience more tongue pain and soreness14,17,18,22 and less cheek and lip pain.8,14,18,23,24 This may be attributed to the restriction of tongue space by lingual appliances that are supported by Thomas Stamm, 25 but another study shows that the use of low-profile brackets does not change the results. 15 In both types of appliances, by the time pain experience is diminished,14,18,26-29 it is unclear if it affects the stages of treatment or adaptation. During treatment, maximum use of analgesics is required in the initial stage of treatment, 18 but there is no significant difference between the amount used in labial and in lingual.14,18
Eating Difficulties
With any type of fixed orthodontic appliance, there will be problems during eating, because it is an external device in an oral environment especially with firm food.14,30 Researches have shown greater eating difficulties in patients with lingual appliance14,16,22,30 especially after the placement of the appliance. 16 The majority of pain is felt in the first month 31 and it takes a longer time to recover and adapt to appliances. 32 After 3 months of placement, results are not significant and they are the same.14,16,30 Among lingual appliances, lower eating difficulties are reported with customized brackets. 33
Speech Difficulty and Tongue Discomfort
Many people state that speech difficulties are one of the most important problems of lingual appliances 14 and the others may include eating difficulties 16 or tongue discomfort. 34 Researches have shown that dental appliances “such as orthodontic appliances” can cause articulation problems35-37 at the beginning and decrease thereafter. Both labial and lingual appliances have speech problem at the beginning of treatment, but lingual has more difficulty14,16,30,38,39 due to more changes in the articulation zone. Speech disorder in patients with labial appliance disappears after 1 month, but in patients with lingual appliances, it may persist up to 3 months or more in some patients.23,24,34,40 Speech problems are very important for patients and may have some impact on the quality of life;15,41 therefore, it is an important part of the informed consent process.
Adaptation
In recent years, aesthetic orthodontic appliances have a good promotion to increase the acceptability of patients who are concerned about their appearance, 42 although today the number of adults who are willing to have an orthodontic treatment is growing and they are seeking for esthetics during treatment; therefore, esthetic orthodontic treatment becomes popular. In the application of labial orthodontic appliances, it is more recognizable by the other people, whereas labial orthodontic appliances are really hard to notice. 14 Females under 40 are more likely to choose lingual appliances due to esthetics, 41 while patients with somatization symptoms‚ obsessive-compulsive traits‚ and/or a narcissistic type of personality traits are the first applicants of lingual appliance due to their anxiety. 43 Researchers have found that patients who choose lingual appliances are more perfectionists. 44 The adaptation period for many persons is approximately the same with both labial and lingual between 30 days, 14 while some patients with lingual appliances never adapt fully. Fortunately, it has been shown that satisfaction between patients treated with labial or lingual appliances are the same and both of them are ready to recommend it to others. It seems custom lingual appliances and labial appliances have an equal acceptability. 30 Therefore, assessing personality expectation of patients is more necessary to answer which type of appliance can perceive treatment goals and patients’ expectations.
Caries and Demineralization
Achievement of good oral hygiene is necessary for the prevention of caries during orthodontic treatment. 45 However, all patients experience impact on oral hygiene and there appears to be a need for oral hygiene instruction and motivation of patients during treatment. 30 Therefore, it seems difficult to clean lingual brackets due to smaller interbrackets distance. 46 The main reason for caries is plaque accumulation especially around the brackets, underneath the arch-wire and between gingiva and brackets. Researches show that the risk of demineralization in the lingual surface of the tooth under brackets is less than that in the buccal, and it is less prone to caries. van der Veen et al investigated this in their study and revealed that the number of white spot lesions that developed or progressed during treatment on the buccal surfaces was 4.8 times higher than those on the lingual surfaces, and that the extension of the lesion was 10.6 times higher. Although many of the white spots that appear after treatment existed before treatment, there is a need for more sensitive detection and prevention methods. 47 The most common method used to identify the risk of caries is Lactobacillus and Streptococcus mutans.48-51 Although studies have shown that lingual appliances cause an increase in S. mutans, no differences were found in Lactobacillus count, salivary flow rate, and salivary buffer capacity. 52
Periodontal Indices
Orthodontic appliances cause plaque-induced gingivitis, gingival enlargement, and increase in periodontal depth (PD) and bleeding on probing (BOP). 5 When patients are treated with a lingual appliance, it is very difficult to clean lingual surfaces23,25,32,53 and studies have shown more plaque accumulation and gingivitis in person with lingual appliance.14,25,54 However, the occurrence of a white lesion is lower in lingual appliances. 54 Also, it has been shown that patients with a labial appliance experience significantly higher frequency of gingivitis in posterior maxillary teeth, but patients with lingual appliances experience it more often in lingual anterior teeth. 55 Regarding the bleeding on probing (BOP) and PD, some studies have shown the significant increase of PD and BOP,56-58 and the others have stated no significant differences.56,58-61 Therefore, further studies are required to prove the effects of lingual appliances on these parameters. In addition, change in periodontal microflora was reported after bonding of lingual appliances with a higher prevalence of pathogens such as Aggregatibacter actinomycetemcomitans. 62
Treatment Outcome
A high standard of outcomes is necessary for successful orthodontic treatment. Results showed that lingual appliances can achieve a significant extent of treatment goals. 63 Also, treatment outcomes are the same with labial and lingual appliances43,64 and treatment duration in labial and lingual appliances are the same.64,65 In this manner, the number of lost brackets during the first year of treatment 66 and root resorption during treatment are similar. 65 In some studies, it was stated that lingual appliances lead to an increase in intercanine width and decrease in intermolar width.67,68 A possible explanation for these is prominent offset with the small interbrackets distance in anterior part that may cause more intercanine width. Also, lingual appliances cause tongue discomfort and move it to an anterior and inferior position that changes the force on posterior teeth and may cause lesser intermolar width, 67 although more research is required to prove this. Evidences show that lingual appliances provide better anchorage control than labial appliances, and that lingual appliances are associated with less anchorage loss.10,12 A possible explanation is that there is smaller arch perimeter leading to better anchorage control 69 and that the lingual brackets are close to the resistance center of the teeth which causes an increase in the anchorage value. 11
Conclusion
From the beginning of lingual orthodontics, this concept has varied over the time for solving problems. Early researches in this area were limited to outcomes and advantages or disadvantages in comparison with labial orthodontics. In recent years, lingual orthodontics has been promoted continuously and now there are several systems and options for orthodontists to achieve their inspections. In this article, we attempted to gather some evidence about lingual orthodontic which can change opinions about it. Also, there are wide choices in lingual orthodontics for research and promotion. Our article concluded the following:
The pain of lingual appliances starts a little earlier and lasts longer, and patients with lingual appliances experience more tongue pain and soreness and less cheek and lip pain. Patients with lingual appliances have greater eating difficulties, especially after the placement of appliances, and take longer time to adapt to appliances. Lingual appliances have more speech difficulty due to major changes in the articulation zone and take longer time to disappear. The adaptation period time for many persons is approximately the same with both labial and lingual between 30 days, while some patients with lingual appliance never adapt fully. It seems difficult to clean lingual brackets due to smaller interbrackets distance, but the risk of demineralization in lingual surface of the tooth under brackets is less than buccal and it is less prone to caries. Lingual appliances generally cause more plaque accumulation and gingivitis, especially in lingual anterior teeth; however, labial appliances are associated with high frequency in posterior maxillary teeth. Lingual appliances can achieve a significant extent of treatment goals with the same outcomes, duration, lost brackets, root resorption, and lesser anchorage loss.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.