
Abstract
Objective:
The present study was conducted to evaluate the effectiveness of treatment outcome using American Board of Orthodontics (ABO) scoring and total treatment time between labial and lingual appliance and also to assess patients’ perception of the lingual appliance system.
Materials and Methods:
Twenty patients requiring first premolar extraction were selected; 10 patients were treated with a lingual and 10 with a labial appliance. The treatment duration and ABO scores were recorded from the posttreatment dental casts and orthopantomogram (OPG). A questionnaire was used to evaluate the perception of patients on lingual treatment using a visual analogue scale (VAS).
Results:
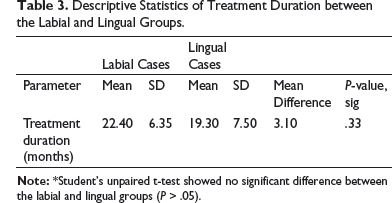
The total ABO scores of the 2 groups were not statistically significant. The lingual- and labial-appliance treatments were completed in 19.30 ± 7.50 and 22.40 ± 6.35 months, respectively. The VAS showed that lingual-appliance patients experienced a moderate amount of pain and discomfort to the tongue and soft tissues. Patients did not have considerable difficulty with speech and in maintaining oral hygiene.
Conclusion:
Lingual appliance cases finished with a comparable quality of orthodontic treatment precision well within the normal treatment time frame. These patients had moderate difficulties with speech, tongue irritation, and pain. They did not have difficulty in maintaining their oral hygiene and were satisfied with their smile and treatment outcome.
Keywords
Introduction
Adult orthodontics is increasing in its popularity, and the advent of “invisible braces” has given options to patients who previously refused labial appliance. In an attempt to provide patient comfort, mechanical efficiency, and precise tooth positioning, various designs of lingual brackets have been used and frequently modified over the past 10 years. 1
The most commonly used alternative to the labial appliance is the lingual appliance, but it results in different clinical outcomes and a short interbracket distance, which is considered to be problematic, especially during detailing. 2 Clinical outcomes of the lingual appliance have been evaluated in previous studies,1, 3 mainly using cephalometric analysis, but the Objective Grading System (OGS) can also be used to evaluate the lingual appliance. Few clinical studies1, 3, 4 have compared the clinical outcome of the lingual appliance with that of the labial appliance.
Thus, the purpose of this study is to compare the final treatment outcomes (effectiveness) of the patients treated with labial and lingual fixed appliances and also to assess patients’ perception of the lingual appliance system.
Methodology
In this prospective clinical study, the patients were selected from the Department of Orthodontics and Dentofacial Orthopedics, College of Dental Sciences (CODS), Davangere. Ethical clearance was obtained from the Institutional Ethical Committee before the commencement of the study (Ref: CODS/2427/2018-19).
This prospective study used data from the first 10 consecutive cases that met the inclusion criteria for lingual cases and compared these cases with 10 matched labial cases. All eligible patients who met the inclusion criteria and provided informed consent for their participation were randomly allocated in the analysis. The case selection criteria were as follows:
Patients requiring therapeutic extraction of first premolars; Angle Class II malocclusion patients; Patients with aesthetic concerns; Patients with no history of previous orthodontic treatment; and Patients who will not undergo any lateral expansion of dental arches.
The labial group consisted of 8 women and 2 men, whereas the lingual group consisted of 10 women, with average (± standard deviation [SD]) ages of 16.20 ± 2.1 years and 19.60 ± 1.8 years, respectively.
Ten patients were treated with a lingual appliance, and the other 10 with a labial fixed appliance. Slot brackets of 0.018 inch were used in the treatment of all the patients. STb lingual brackets (Ormco, Orange, CA) were used to treat the lingual cases. Sequencing of wires in the labial cases was initially with 0.014-inch or 0.016-inch nickel-titanium (Ni-Ti) and later with 0.016 inch × 0.022 inch Ni-Ti and 0.016 inch × 0.022 inch stainless steel (SS), and then stabilizing 0.017 inch × 0.022 inch SS wires were placed. The sequence of wires in the lingual cases was initially 0.014-inch or 0.016-inch Ni-Ti, then 0.018-inch titanium molybdenum alloy (TMA) or 0.016-inch SS, followed by 0.017 inch × 0.022 inch copper (Co)-Ni-Ti, 0.0175 inch × 0.0175 inch TMA, or 0.016 inch × 0.016 inch SS. Finally, 0.016 inch × 0.022 inch SS or 0.017 inch × 0.022 inch SS was placed. In all the cases, anteriors were retracted by sliding mechanics using en masse retraction. In either group, a Nance appliance or transpalatal arch was placed. An overcorrection was incorporated into the lingual setup as recommended by Scuzzo and Takemoto. 2
American Board of Orthodontics Objective Grading System
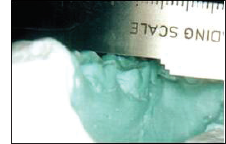
The final outcome of the treatment was assessed based on the ABO grading system using posttreatment dental casts and panoramic radiographs. This system for scoring contains eight criteria: alignment, marginal ridges, buccolingual inclination, occlusal relationships, occlusal contacts, interproximal contacts (Figures 1 to 3), overjet, and root angulation. 5
The principal author was initially trained in the ABO OGS using the ABO Calibration Kit from February 2010, as well as a tutorial using the ABO gauge. Only one investigator evaluated all the cases.
Measuring Buccolingual Inclinations of Maxillary Molar Using ABO Gauge.
Measuring Marginal Ridge Using ABO Gauge.

Measuring Interproximal Contacts Using ABO Gauge.

Questionaire 1 to 4.
Questionaire 5 to 10.
Treatment Duration
The total time taken for completion of the treatment was assessed between the two groups from the beginning of the treatment till the end of the treatment.
Assessment of Patients’ Perception of Lingual Mechanotherapy
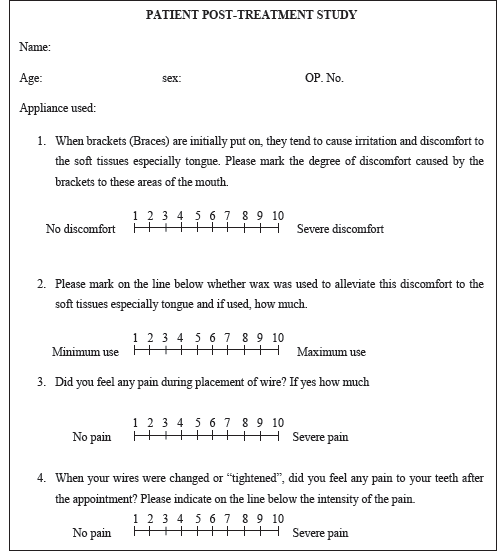
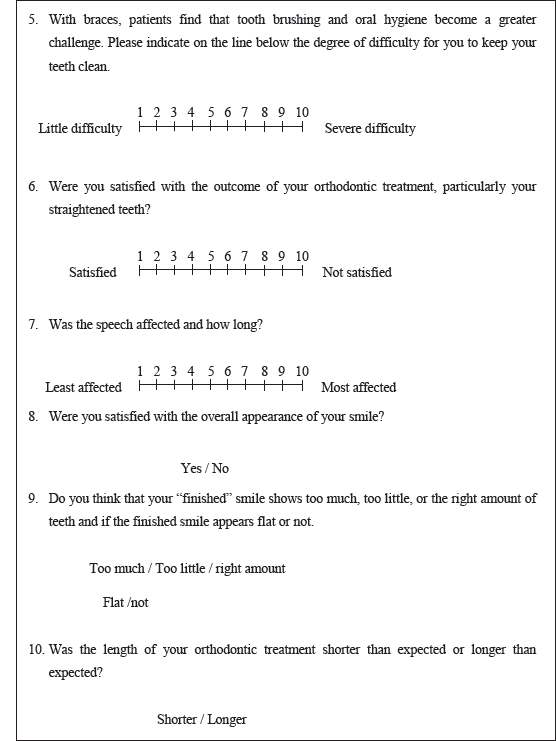
All 10 lingual patients were asked to complete a questionnaire (Figures 4 and 5) that included 10 questions. The perception of the patients on lingual treatment was assessed using a visual analogue scale (VAS).
Patients were given oral instructions, along with an explanation on how to complete the questionnaire. Questions 1 to 7 were evaluated on the VAS, where patients were asked to mark on a scale with scores ranging from 1 to 10, whereas questions 8 to 10 were with options, in which the patient had to mark any one option.
Results
Statistical Analysis
All the data were analyzed with the MINITAB version 13.1 and SPSS software. The results were presented as mean ± SD. To evaluate the repeatability of the intra-examiner, randomly, 8 patients were selected from the main sample to form a subsample. Measurements were repeated at 8 weeks after the first measurements to evaluate the intra-examiner reliability using the intraclass correlation coefficient (ICC). ICC values equal to 0 represented agreements, which are equivalent to that expected by chance, while 1 represented perfect agreement.
Unpaired t-test was used for intergroup comparison of changes between the labial and lingual groups to assess age and treatment duration, and a chi-sqaured test was used for assessing the sex differences between the 2 groups. The nonparametric Mann–Whitney U test was chosen for intergroup comparison of posttreatment ABO scoring between the labial and lingual groups. A P-value of .05 or less was considered for the results to be statistically significant.
The results showed that all ICC values for the lingual and labial group were >.90, showing good repeatability of the measurements (the labial- and lingual-group coefficients of variation were .96 and .92, respectively).
American Board of Orthodontics Scores
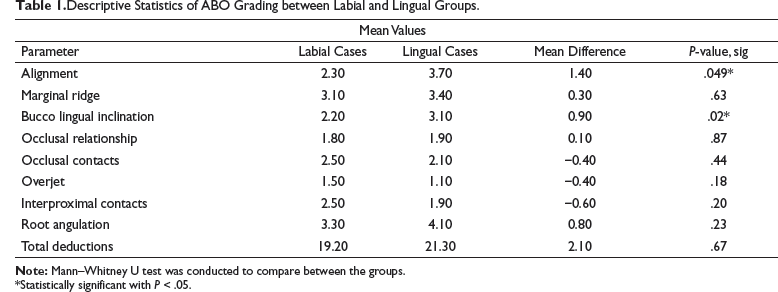
Descriptive Statistics of ABO Grading between Labial and Lingual Groups.
*Statistically significant with P < .05.
95% Confidence Intervals of the Mean Difference of the ABO Scores.
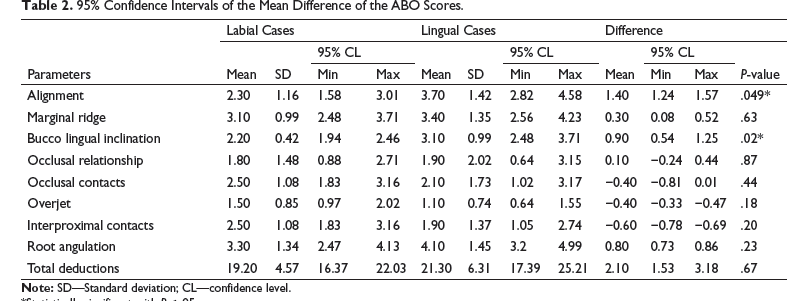
*Statistically significant with P < .05.
Treatment Time (Table 3)
Descriptive Statistics of Treatment Duration between the Labial and Lingual Groups.
Questionnaire Analysis
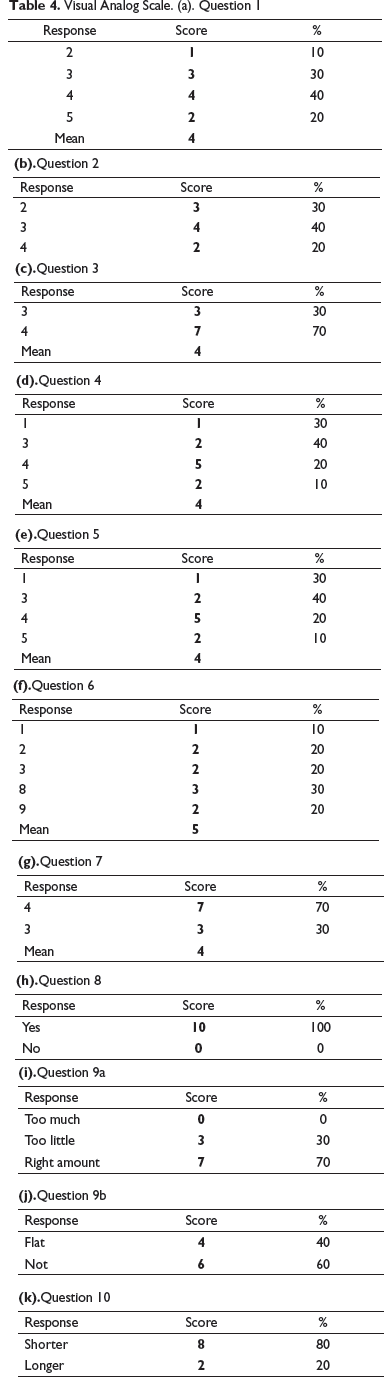
Visual Analog Scale. (a). Question 1
Discussion
A large number of patients, especially adults, are seeking more aesthetic forms of orthodontic treatment. However, at the same time, these patients also demand a high level of comfort, greater treatment efficiency, better aesthetic results, and faster treatment.
The lingual appliance therapy has its own set of unique problems by virtue of the reduced tongue space, and irritation also adds to the patients’ and practitioner’s woes.
Very few studies in the literature have comprehensively mentioned the effectiveness of the lingual appliance system and compared it to the labial appliance system.1, 3, 4, 6Hence, this study was undertaken to analyze mainly the finished occlusion, patient perception, and treatment time.
American Board of Orthodontics Grading System
Lingual-appliance patients are extremely demanding. The majority of them are adult patients with extremely high aesthetic and functional expectations, and hence finishing and detailing in these cases takes a whole new meaning and is very important as far as functional stability is concerned.
Finishing and detailing of a lingual-appliance case is difficult due to the reduced interbracket distance, which makes placement of finishing bends very cumbersome due to the resulting stiffness of the wires. The anatomy of the lingual surface also makes precise repositioning of brackets difficult. 7 Finishing a lingual case perfectly is far more challenging than doing the same with a labial case. Hence, we undertook a detailed posttreatment assessment of the lingual technique compared to the labial one.
One the best ways to assess a finished case is with the use of ABO OGS. 5
The lingual group finished with a total score of 21.30, and the labial group with 19.20. The difference in the mean total ABO scores between the 2 groups was 2.10, which is not statistically significant. This is similar to the finding of Deguchia et al’s study. 4 Of the individual ABO scores compared, only alignment and buccolingual inclination showed a statistically significant score. These findings show that both labial and lingual appliance systems finished with a comparable quality of orthodontic treatment precision.
Treatment Time
Treatment duration is another basic concern, because most patients are adults who cannot commit to long-term treatment, and it is thought that the complexity of lingual appliance mechanics and the difficulty in working with a limited amount of space intraorally and reduced interbracket space tends to increase the treatment time. The differences in treatment time between the 2 groups were not statistically significant.
This study infers that lingual appliance treatment does not require an excessively lengthy treatment time and can be completed well within the normal time frame of regular orthodontic treatment. The reduced treatment time seen with the lingual appliance is very likely the result of rapid tipping of the anteriors into the extraction space due to the tipping movement created during retraction, leading to a very short space closure stage. However, a detailed, stage-wise analysis of the treatment time is required over a much larger sample to support the above finding.
Visual Analogue Scale
Placement of the appliance on the lingual aspect brings to light a new set of problems associated with patient discomfort. With the lingual technique, the area of main concern is the tongue. All the related functions, such as speech, swallowing, and oral hygiene maintenance, are affected. This study investigated how these patients related to the problems and dealt with them. Patient perception was assessed using a set of 10 questions that were aimed at the various problems that are typically faced by lingual-appliance patients.
The answers to questions 1 and 2 suggest that lingual fixed mechanotherapy caused average discomfort to the tongue and soft tissues and wax was not used much to alleviate the discomfort. Fritz et al, 8 Hohoff et al, 9 Cem and Öztürk, 10 and Stamm et al 11 all reported discomfort to the tongue and irritation during the initial period after lingual-appliance placement. Stamm et al 11 recommended the use of small-dimension, custom-made brackets to reduce patient discomfort. In Cem and Öztürk’s 10 study, patients, after wearing the appliance for 4 weeks, did not experience any discomfort. This was similar to the finding in Fujita’s 12 study, and he attributed the reason for tongue discomfort to the reduction in functional space.
Questions 3 and 4 pertained to pain during wire placement and during subsequent appointments. The results show that a moderate amount of pain was experienced during the placement of wire and during subsequent appointments. Wu et al 13 also found that lingual-appliance patients experienced a moderate amount of pain during the initial period which gradually decreased over a period of time, similar to the findings of our study.
Question 5 related to the maintenance of oral hygiene, and the results show that patients experienced average difficulty in maintaining their oral hygiene. Cem and Öztürk 10 also reported difficulty with oral hygiene maintenance in 100% of the patients in the study. Stamm et al 11 recommended the use of smaller-dimension custom-made brackets for better oral hygiene. Oral hygiene maintenance is considered a problem because of the lack of tongue stimulation to the gingival tissues, that is, normal stimulation of the gingival tissues is prevented due to the presence of the appliance on the lingual. This creates problems with self-cleansing mechanisms. 14
Question 6 pertained to the outcome of orthodontic treatment, and the results show that patients were satisfied with the outcome of treatment. Fritz et al 8 also used a questionnaire to assess the motivation and appliance acceptance of lingual-appliance patients, which showed that 99% were content with the treatment outcome, similar to the findings of our study.
The seventh question examined the effect of lingual fixed mechanotherapy on speech, and the results show average difficulty with speech. Seven out of the 10 patients faced difficulties in speech for 1 month, and the 3 other patients had difficulties for only 1 week. Cem and Öztürk 10 in their study stated that in the majority of patients in the lingual group, within 4 weeks after appliance placement, speech problems disappeared. Longer-lasting speech problems (3 months) were seen in few of the patients with lingual brackets. These data are in agreement with the findings of Sinclair et al 15 and Artun. 16
Mariotti and coworkers conducted a study and concluded that lingual appliances do have an effect on speech, most speech distortions being apparent immediately after placement and then diminishing with time. Within a month’s time, patients were well adapted to the appliance, and any distortions in speech at this time were not clinically significant. 1
Stamm et al 11 found that initially with the lingual appliance there was difficulty in speech, which reduced over a period of time, and they suggested that a detailed briefing on the extent and duration of potential impairments to oral comfort and functions be given prior to the insertion of lingual brackets.
Questions 8 and 9 pertained to the overall appearance of the smile—whether the finished smile showed too much, too little, or the right amount of teeth and if the smile was flat or not; the results show that 7 patients felt that the finished smile showed the right amount of teeth, whereas 3 felt that the finished smile showed too little teeth, and 4 out of the 10 patients felt that their finished smile was flat. Hence, the majority of the patients were satisfied with their smile and incisal exposure.
Question 10 asked whether the length of the orthodontic treatment was shorter than expected or longer, and patients were informed regarding the normal duration of treatment. The results show that 8 out of the 10 patients felt their treatment was shorter than expected, whereas 2 felt their treatment was longer than expected.
The VAS evaluation is summarized as follows: Patients experienced a moderate amount of pain and discomfort to the tongue and soft tissues. Speech was impaired only for about a month, and patients did not experience any noticeable difficulty in maintaining their oral hygiene. The majority of the patients were satisfied with their treatment outcome and smile and the treatment duration.
Conclusion
The lingual appliance finished with a comparable quality of orthodontic treatment precision.
Lingual-appliance treatment can be completed well within the normal time frame of regular orthodontic treatment.
Patients had moderate difficulties with speech, tongue irritation, and pain. Speech was impaired only for about a month.
Patients did not have considerable difficulty in maintaining oral hygiene.
The majority of the patients were satisfied with their treatment outcome, smile and treatment duration.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical clearance
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.