
Abstract
Introduction:
The presence of existing osteoporotic vertebral fracture (OVF) increases the mortality risk. However, the influence of the characteristics of OVF is unclear. This study aimed to investigate the influence of new OVF on patients’ long-term prognosis using our past cohort study.
Method:
This is an extension study of our cohort study carried out between 2005 and 2007. In the present extension study, of 420 patients, 197 whose contact information was available at the 6-month follow-up were included in the telephone survey in 2018. Five patients refused to participate in the survey, and 82 could not be contacted. Eventually, 110 patients were enrolled. Of the Demographic data, radiological findings, medical history, and clinical outcome were investigated at injury onset and at the 6-month follow-up. A proportional hazard model was used to investigate the risk factors for mortality.
Results:
Among 110 patients, 33 died. Male sex and low body mass index (BMI <18.5 kg/m2) were significant risk factors for mortality [hazard ratio (HR) = 6.40, 1.01–40.50; 5.24, 1.44–19.04, respectively]. The history of stroke and liver disease increased the risk of mortality (HR = 13.37, 1.93–92.7; 6.62, 1.15–38.14, respectively). As regards radiological findings, local kyphosis progression per 1° or ≥7° were significant risk factors of mortality (HR = 1.20, 1.06–1.36; 5.38, 1.81–16.03, respectively).
Conclusions:
A telephone survey at 12 years after the occurrence of OVF analyzed risk factors for mortality and showed that a progression of local kyphosis in fractures between injury onset and 6 months after injury was a risk factor of poor prognosis.
Introduction
Osteoporotic vertebral fractures (OVF), as the most common fractures among osteoporotic fractures, are shown to occur in approximately 40% of women aged 80s. 1 The number of patients with OVF is expected to increase with the increasingly aging population. As clinically apparent OVFs account for only one-third of all OVFs, it is unclear to what extent the predictive findings can be generalized to individuals with asymptomatic vertebral deformities. 2 While healthy life expectancy is considered important, the quality-adjusted life year (QALY) is shown to decrease by 0.1 when OVF occurs. 3 In addition, they found no significant QALY differences between clinical and asymptomatic OVFs. Therefore, the influence of OVF on the quality of life (QOL) in older people should not be ignored. Large-scale 10-year randomized controlled trials of antiosteoporotic agents have proved the long-term effectiveness of bisphosphonate 4 and denosumab 5 for the prevention of fractures. However, according to long-term cohort studies on community-dwelling older population, 6,7 the presence of existing OVF increases the mortality risk. This high mortality rate after a clinically diagnosed OVF appears to increase progressively over time since the fracture event 6,7 . This is in contrast with the increased mortality rate after a hip fracture, where the increased risk is predominantly within the first year after the fracture. 8 Although the cause of death in OVF patients might be different from those with hip fractures, the reason is not yet elucidated. Especially, the OVF morphology, fracture healing process, and the effect of treatment on injury or immediately after injury on the mortality have not been shown. Thus, this study aimed to investigate the influence of new OVF on patients’ long-term prognosis using our past cohort study. 9 –11
Methods
This is an extension study of our previous cohort study carried out between 2005 and 2007 10 (Figure 1). In the primary cohort study, 485 patients were enrolled and 420 patients with new OVF (aged ≥65) were followed for 6 months at 25 facilities to investigate the predictors of nonunion by magnetic resonance imaging (MRI), 10 factors that influence patients’ QOL, 9 and effects of conservative treatment. 11 On the initial visit to the respective institutes, a new OVF was diagnosed if the following were present: acute back pain, a deformed vertebral body on radiographs, and an abnormal intensity within vertebral bodies on MRI.

The primary cohort study enrolled 485 patients with osteoporotic vertebral fractures and 420 patients with new OVF were followed for 6 months. Of those patients, 197 patients whose contact information was available at the 6-month follow-up were included into the present extension study. Eventually, 110 patients were investigated. Of the 87 patients who could not be followed in 2018, five patients declined participation in the survey and 82 patients could not be contacted because the telephone number was changed in 61 patients and multiple calls did not connect to the other 21 patients. Among 110 patients, 33 died.
In the present extension study, of the 420 patients, 197 patients whose contact information was available at the 6-month follow-up were included in the telephone survey in 2018. Verbal informed consent was obtained from the patients or their family by a physician. After obtaining informed consent, the caller was asked whether the patient was alive or not. If the patient had died, the time and reason of death were recorded. Eventually, 110 patients were investigated. Of the 87 patients who could not be followed in 2018, five refused participation in the survey and 82 could not be contacted because the telephone number was changed in 61 patients and multiple calls did not connect to the other 21 patients.
As baseline data between 2005 and 2007, we collected the following information: sex, age, bone density (ultrasound heel bone measurement device), back pain, mini-mental state examination (MMSE) result, medical history (presence/absence of stroke, heart disease, respiratory disease, liver disease, kidney disease, and gastrointestinal disease, and diabetes mellitus). At 6 months after injury, pain, MMSE, Short-Form 36, rate of vertebral compression, and degree of local kyphosis were assessed. With regard to treatment, the presence/absence of a brace for OVF as well as antiosteoporotic agents was investigated. Pain severity was assessed subjectively by patients using a visual analog scale (VAS, 0-100). To evaluate patients’ performance of activities of daily living (ADL), we used the criteria proposed by the long-term care insurance system of the Japanese Health and Welfare Ministry for evaluation of the degree of independence of older individuals with disability. 12 ADL classifications were ranked as follows: rank J, although some disability is present, daily life was almost independent and patients can go outdoors without assistance from other individuals; rank A, patients lived independently indoors but required assistance to go outdoors; rank B, patients required some assistance living indoors and spent most of the day in bed but were able to sit up; and rank C, patients spent all day in bed and required assistance with urination/defecation, getting dressed, and meals. A structured self-administered questionnaire was used to collect data regarding medical history.
At the time of injury and at 6-month follow-up, patients were examined using plain radiography of the spine. The ratio of vertebral compression, degree of fractured vertebral kyphosis, and previous vertebral fractures were investigated. The percentage height of the anterior wall was calculated using the following formula as compression ratio: [2 × affected vertebral height/(lower vertebral height plus upper vertebral height)] × 100. If the adjacent vertebral body, either cranial or caudal, was deformed because of an old fracture, the vertical height of the anterior wall of the fractured vertebral body was divided by the vertical height of the anterior wall of the adjacent non-deformed vertebral body. Whether a fracture was in the acute phase was judged by MRI.
The study design was approved by the ethics committees for clinical research at each institute. Informed consent was obtained from all individual participants included in the study.
Statistical analysis
T-test was used for continuous variables and a χ2 test or Fisher’s exact test for categorical variables. Since there was an association of the difference of local kyphosis progression of the fractured vertebrae between injury onset and at 6 months after injury, the receiver operating characteristic (ROC) curve was used to investigate the area under curve (AUC). A proportional hazard model was used to investigate risk factors of mortality. The adjusted hazard ratio (HR) was adjusted for variables with p < 0.05 including age, sex, BMI, stroke, liver disease, smoking status, and change in local kyphosis per 1° or >7°. Statistical test results were considered significant at p < 0.05. All p-values were two-sided. All analyses were performed using the SAS software package, version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Among 110 patients, 33 had died. The mortality rate was 30%. Of the 33 deaths, the causes were cancer (n = 4), cardiovascular disease (n = 6), stroke (n = 4), pulmonary disease (n = 2), others (n = 6), and unknown (n = 11). Baseline differences are shown in Table 1. The study showed that the mean age was higher (77.7 vs. 74.5, p = 0.021) and BMI was lower (20.6 vs. 22.3, p = 0.02) in deceased group than in the living group. Male patients were more likely to die than female patients (death rate 66.7%, 12/18 patients vs. 22.8%, 21/92 patients, p < 0.001). A history of stroke and liver disease was significantly more predominant in the deceased group than in the living group (18.2% vs. 2.6%, p = 0.009; 18.2% vs. 3.9%, p = 0.020, respectively). The number of never smokers was low in the deceased group than in the living group (54.6% vs. 75.3%, p = 0.040). Table 2 shows the assessments of images at injury onset and at 6 months after injury. Vertebral kyphotic deformity greatly progressed in the deceased group (8.7° vs. 5.5°, p = 0.004). As regards clinical data, at 6 months after injury, no difference was found in the clinical scores including pain, MMSE, and SF-36. However, ADL status tended to be worse in the deceased group at injury and 6-month follow-up (Table 3).
Comparison of demographic data and comorbidities between the deceased group and living group.

Comparison of radiological findings between the deceased group and living group.

Comparison of clinical outcome between the deceased group and living group.

Hazard ratios (HR) are shown in Table 4. Being male and having a low BMI (<18.5 kg/m2) were significant risk factors for mortality (HR = 6.40, 1.01–40.50; 5.24, 1.44–19.04, respectively). The history of stroke and liver disease were also identified to increase the risk of mortality (HR = 13.37, 1.93–92.7; 6.62, 1.15–38.14, respectively). The cutoff value of the degree of kyphotic deformity progression was 7° in the ROC curve. The distance from the top-left corner of the ROC curve was used to determine the cutoff value of local kyphosis progression for death, with an AUC of 0.662. Both HRs of local kyphosis progression per 1° and ≥7° were calculated because the AUC was less than 0.7. Local kyphosis progression per 1° or ≥7° were significant risk factors for mortality (HR = 1.20, 1.06–1.36; 5.38, 1.81–16.03, respectively).
Risk factors for death at the final follow-up.
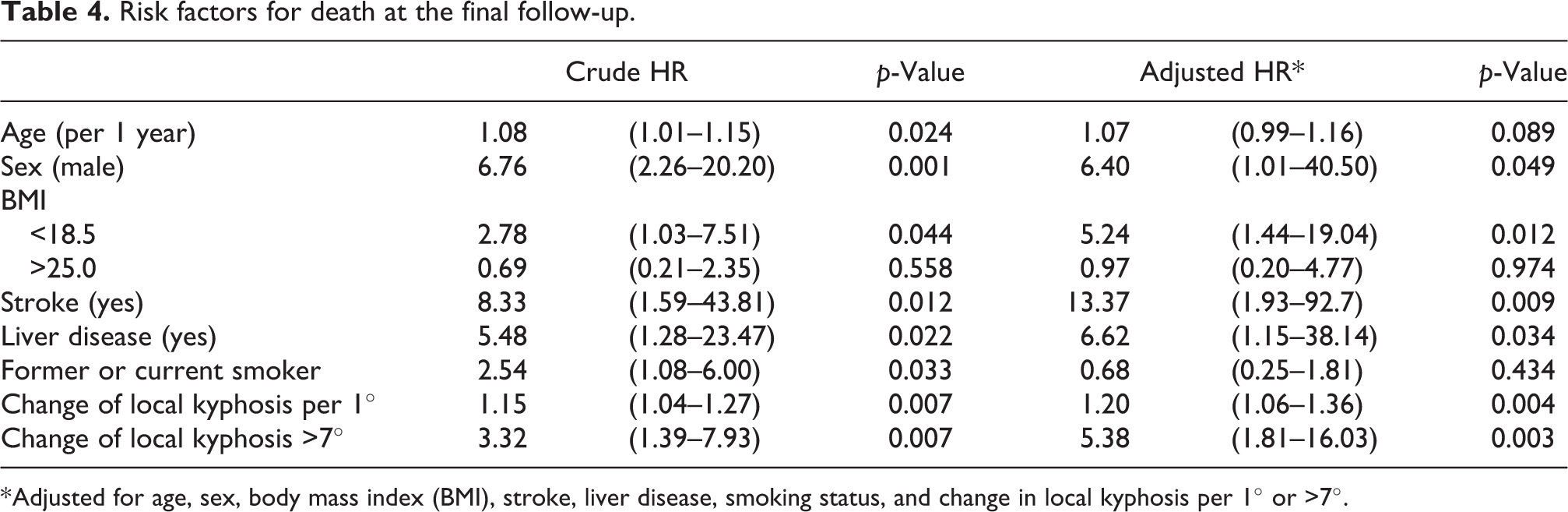
* Adjusted for age, sex, body mass index (BMI), stroke, liver disease, smoking status, and change in local kyphosis per 1° or >7°.
Discussion
This study demonstrated that 33 patients (30%) had died in more than 10 years follow-up after the onset of OVFs even though 87 patients among 197 were lost. Previous studies have reported that OVF increases the mortality rate 8 and that the greater number of OVFs is associated with increased mortality rate of patients. 13 Although the present study could not compare the mortality rate with subjects without OVFs of, factors that influence death were analyzed. Progression of the local kyphosis was shown to be an independent risk factor. The progression of vertebral kyphosis is considered to reflect repeated stress due to nonunion or bone fragility. In these patients, malalignment due to advanced kyphosis or nonunion which is associated with residual pain 14 may cause limitations in physical activity and increase the mortality rate. Although the reason is unclear, careful follow-ups for at least 6 months and appropriate intervention are needed in patients with fragile bones. A report 15 based on the US Medicare data demonstrated that balloon kyphoplasty reduced the mortality rate, which may indicate that balloon kyphoplasty reduces the progression of kyphosis or prevent nonunion.
The reason of the increased mortality has been reported in several studies. Kado et al. 13 investigated the reason of the increased mortality in a prospective cohort study including 1915 female patients with 8.3 years of follow-up. They demonstrated that the risk of cancer and pulmonary disease was higher in patients with OVFs and mentioned that severe kyphosis was strongly predictive of pulmonary deaths because those with underlying lung disease and decreased respiratory reserves may not tolerate restrictive changes in thoracic anatomy resulting from vertebral fractures. Meanwhile, Hasserius et al. 6 demonstrated that the mortality in cancer and in cardiovascular diseases was significantly increased among female vertebral fracture patients. On the contrary, Trone et al. 16 demonstrated that female patients with any prevalent vertebral fractures also had increased mortality risk from ‘‘other’’ causes (adjusted HR=1.59) but not cardiovascular disease or cancer. Calcium supplements (not co-administered with vitamin D) are associated with an increased risk of myocardial infarction. 17 Another study also demonstrated that increasing calcium intake from diet might not confer significant cardiovascular benefits, while calcium supplements, which might raise MI risk, should be taken with caution. 18 Four-monthly supplementation with 100 000 IU of oral vitamin D may prevent fractures without adverse effects among community-dwelling in men and women. 19 Although the main cause of an increase in the mortality rate following OVF remains unclear, the results were obtained while various confounding factors were taken into account in all these studies; thus, OVF may independently have an influence on prognosis.
In our study, stroke and liver disease were risk factors for poor prognosis. Stroke and chronic liver disease, including hepatitis B and C infection and alcoholic hepatitis, are well-known risk factors of poor prognosis. 20,21 Osteoporosis is a known consequence of stroke, associated with an increased incidence of fractures, mainly of the hip, leading to further disability. 22 In addition, patients with chronic liver diseases have malabsorption of calcium and phosphate, reduced concentration of 25-hydroxyvitamin D, an increase in parathyroid hormone level, and reduction in the number and activity of osteoblasts. 23 Therefore, these conditions might exert additional effects on mortality risk and osteoporosis should be appropriately treated because OVF is an independent risk factor of death.
Although obesity is an important public health problem in Western countries, it has been reported that being underweight remains an important public health problem too, especially in males.24,25 The increased mortality in underweight males has been mainly attributed to lung cancer among smokers. 25 The impact of obesity on mortality is small primarily due to the low prevalence of obesity in the Japanese population as a whole. 24 In our study, while only 2 patients (2%) were obese (BMI ≥30), 22 patients (20%) were underweight. A large study 26 conducted in Japan showed that a low BMI in elderly people was associated with an increased risk of all-cause mortality. The authors mentioned that thin older adults might be high risk for infections and preexisting diseases, which may be linked to both thinness and an increased risk of death.
This study has several limitations. First, selection bias might have occurred because the follow-up ratio was low. Of the 197 patients whose contact information was available, 87 patients (44%) dropped out. A comparison of the follow-up group with the lost group showed that average age was 75.4 ± 6.7 vs. 77.9± 7.3 years (p = 0.014) and average BMI was 21.8 ± 3.6 vs. 23.0 ± 3.4 kg/m2 (p = 0.024), respectively. Other variables including clinical and radiological factors at enrollment and at 6-month follow-up were not different. The higher average age in the lost group might indicate that these patients included those who dropped out presumably because of favorable progress and or because of admission to a nursing home, death, or other reasons. Therefore, more fragile patients might be lost, which implies the risk of type II error. Second, the reason of death was unclear in 33% of the patients who died because this study was carried out based on a telephone survey. However, visiting hospital for survey was very costly and was often difficult for elderly people. A previous study 22 demonstrated that comparison of the interview transcripts revealed no significant differences between telephone and face-to-face interview. Third, detailed data obtained at the 6-month follow-up and telephone survey was not obtained. Therefore, other OVFs and other risk factors for death were not evaluated between the time period. Finally, the association between mortality and the radiograph findings at the 6-month follow-up was evaluated. Six-months of follow-up might be too short to predict future death.
Conclusions
A telephone survey at 12 years after the occurrence of OVF was conducted to analyze risk factors for death. This study showed that a progression of local kyphosis in fractures between injury onset and at 6 months after injury was a risk factor for a poor prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.