
Abstract
Objective
To compare analgesic and mobility effects of different ropivacaine concentrations in femoral–sciatic nerve block, for postoperative analgesia in knee arthroscopy.
Methods
Outpatients (American Society of Anesthesiologists physical classification status of I or II), scheduled for elective knee arthroscopy, were randomly allocated to one of seven groups, prospectively investigating different concentrations of ropivacaine (0.12%; 0.14%; 0.16%; 0.18%; 0.20%; 0.22% or 0.50%), for ultrasound-guided femoral–sciatic nerve block procedures for postoperative analgesia. Visual analogue scale (VAS) pain scores and motor block evaluation scales were observed at 4, 8, 16 and 24 h postsurgery.
Results
In total, 105 patients were enrolled; results were analysed for 103. VAS scores for the 0.12%, 0.14% and 0.16% groups were significantly different from the 0.50% group. There were no significant differences between the 0.18%, 0.20%, 0.22% and 0.50% groups: half maximal effective concentrations and 95% maximal effective concentrations of ropivacaine were 0.158 (95% confidence intervals [CI] 0.149, 0.167) and 0.198 (95% CI 0.186, 0.221), respectively. Rates of motor blockade (Bromage score or hip motor function scale > 0) were significantly different between the 0.50% group and all other ropivacaine doses.
Conclusion
The 0.20% ropivacaine dose for femoral–sciatic nerve block in knee arthroscopy provided satisfactory postoperative analgesia, while preserving ability of motion.
Introduction
Knee arthroscopy is one of the most commonly performed orthopaedic procedures for the diagnosis and treatment of knee disease. Different anaesthetic techniques (including local, regional and general anaesthesia) have been used successfully for this surgical procedure.1,2 More recently, peripheral nerve block techniques (such as femoral, lateral femoral cutaneous and obturator block, with or without sciatic nerve block) have been used, 3 and when combined with general anaesthesia, provide satisfactory pain relief in knee arthroscopy.
Recent growth in outpatient surgery presents new challenges in the field of postoperative pain management, with ongoing research seeking to find the ideal analgesic technique that is site specific, long lasting, easily administered and offers a high therapeutic safety index.
In knee arthroscopy, peripheral nerve block provides the potential advantages of reductions in postoperative pain, nausea, emesis and urinary retention, (together with earlier hospital discharge), when compared with spinal or general anesthaesia.4,5 Combined femoral–sciatic nerve block has been shown to have similar clinical characteristics to low-dose spinal anaesthesia, and to provide satisfactory anaesthesia in outpatient arthroscopic knee surgery. 3 In addition to satisfactory analgesia, the ability of early postoperative motion should be preserved. When using ropivacaine at a concentration of 0.50%, however, prolonged motor blockade of the lower extremities has been observed. 6 Decreasing the concentration of the local anaesthetic is an effective way to preserve the ability of motion, when using epidural analgesia.6,7
The present study evaluated different concentrations of ropivacaine to identify the appropriate level that provides satisfactory postoperative analgesia, while preserving the ability of early postoperative motion.
Patients and methods
Study population
This prospective, randomized study was carried out at the Day Surgery Unit, The Sixth People’s Hospital Affiliated to Shanghai Jiaotong University, Shanghai, China, between November 2011 and May 2012. Outpatients who had an American Society of Anesthesiologists (ASA) physical status classification of I or II (http://www.asahq.org/Home/For-Members/Clinical-Information/ASA-Physical-Status-Classification-System), who were scheduled to receive elective knee arthroscopy, were enrolled. The following were exclusion criteria for patients: any contraindications to the use of regional anaesthesia; severe cardiovascular or respiratory disease; severe liver or kidney insufficiency; severe psychiatric disorder; diabetes and peripheral or central neuropathy; difficulty in comprehending visual analogue scale (VAS) pain scores; difficulty in using an intravenous patient-controlled analgesic device; pregnancy or lactation.
Ethical approval was provided by the Ethical Review Board of The Sixth People’s Hospital Affiliated to Shanghai Jiaotong University. Written informed consent was obtained from all participants.
Study design
Patients were randomized using a computer-generated sequence of random numbers, then allocated to one of seven groups using a sequential sealed-envelope technique. All patients were randomly assigned to receive combined femoral–sciatic nerve block using ropivacaine at concentrations of 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, 0.22% or 0.50%. The volume of medication used was the same (20 ml) for all treatment groups.
Patients were visited on the day before surgery for preoperative assessment and explanation of the study protocols, including the VAS and modified Bromage scale score. 8
Anaesthesia and analgesia procedures
Following insertion of an 18-gauge intravenous (i.v.) cannula into the forearm, patients were premedicated with 2 mg midazolam, i.v., 45 min before starting the surgical procedure. Standard monitoring was used throughout the study, including continuous electrocardiography (lead II), heart rate, noninvasive arterial blood pressure (measured every 5 min) and oxygen saturation via continuous pulse oximetry.
Following premedication with midazolam, ultrasound-guided femoral block and sciatic block were performed by the same two investigators (Z.Z., J.Y.), who had substantial expertise in ultrasound-guided peripheral nerve block and who were blinded to the group assignments. Each patient was placed in the supine position, with the inguinal region exposed on the side of the body where the surgery was to take place. After positioning the target neural structures to the middle of the ultrasound screen, a 22-gauge needle was placed just lateral to the lateral aspect of the ultrasound probe and advanced in plane toward the target neural structures. Using dynamic ultrasound to perform the injection resulted in an even perineural spread of the local anaesthetic. Then, the patient was placed in the lateral decubitus position with a slight forward tilt, hips flexed, with the operative side uppermost. When the hyperechoic, oval to lip-shaped structure of the sciatic nerve was observed by ultrasound, an 18-gauge needle was placed lateral to the lateral aspect of the ultrasound probe and advanced in plane toward the target neural structures. Ropivacaine, of varying concentrations (depending on the study group), was injected with even distribution, deep into the gluteus maximus, the subgluteal space and around the sciatic nerve. Sensory block was evaluated using the pinprick test (22-gauge hypodermic needle), and was judged to be effective if there was a different pinprick sensation in the femoral and sciatic nerve distribution, compared with the other leg, in each patient.
After successful femoral–sciatic block was confirmed, general anaesthesia was induced using 1 µg/kg fentanyl with 2 – 2.5 mg/kg propofol by i.v. injection. Then, a laryngeal mask airway was inserted to keep the airway safe. General anaesthesia was maintained with 1 minimum alveolar concentration of sevoflurane. Patients were allowed to breathe spontaneously via the laryngeal mask airway for the duration of the procedure. End-tidal carbon dioxide was monitored following induction of general anaesthesia. A standard thigh tourniquet, inflated up to 200 mmHg pressure, was used during the surgical procedure.
Assessments were performed by an independent observer (Z.H.J.) who was blinded to the group assignments and to the concentration of ropivacaine. Pain scores at rest and on movement (the knee was bent passively) were assessed with a 100-mm VAS score (where 0 indicated no pain and 100 indicated maximal pain).
The pain-management protocol included rescue analgesia of 400 mg oral ibuprofen every 8 h if requested by the patient. Ibuprofen consumption and incidence of nausea and vomiting were recorded at 4, 8, 12, 16, and 24 h following surgery. Satisfactory postoperative analgesia was defined as a VAS score ≤ 30 at all times throughout the 24-h postoperative period.

Blinding
The research assistant (Z.H.J.) who questioned patients to obtain the main outcome data (VAS and motor block scale scores), the patients and the investigators who performed the surgical procedures were all blinded to the treatment groups.
Statistical analyses
Statistical analyses were performed using SPSS® software, version 13.0 (Abacus Conc–US; SPSS Inc., Chicago, IL, USA) for Windows. Distribution of data was evaluated using the Kolmogorov–Smirnov test. Continuous variables were analysed using either the Student’s t-test or the Mann–Whitney U-test, depending on the distribution of data. Categorical variables were assessed using contingency table analysis and the χ2-test or Fisher’s exact test, as appropriate. Pain scores for consecutive postoperative time points (4, 8, 12 and 24 h) and for other grouping variables were assessed by multivariate analysis of variance for repeated measures. The probit regression model was used to evaluate the effective concentration (95% confidence interval [CI]) of ropivacaine. A P-value ≤ 0.05 was considered statistically significant.
Results
Demographic and clinical data for 103 patients who underwent elective knee arthroscopy with single-shot ropivacaine femoral–sciatic nerve block for postoperative analgesia, delivered at concentrations of 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, 0.22% or 0.50%.
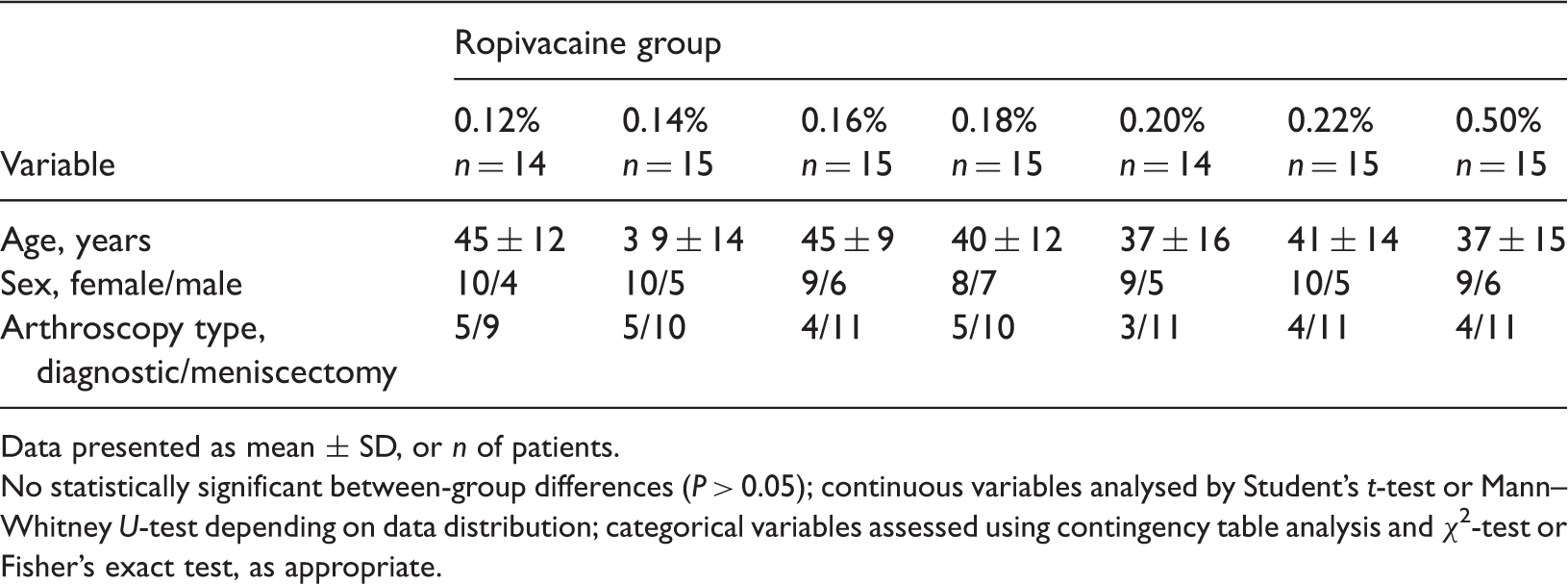
Data presented as mean ± SD, or n of patients.
No statistically significant between-group differences (P > 0.05); continuous variables analysed by Student’s t-test or Mann–Whitney U-test depending on data distribution; categorical variables assessed using contingency table analysis and χ2-test or Fisher’s exact test, as appropriate.
Postoperative pain VAS scores for the 0.12%, 0.14% and 0.16% ropivacaine groups were significantly different compared with the 0.50% group (P = 0.001, P = 0.008 and P = 0.025, respectively), but there were no significant differences between the 0.18%, 0.20%, 0.22% and 0.50% groups (Figure 1). Postoperative pain VAS scores were also significantly different across the time points (4, 8, 16 and 24 h) for all individual ropivacaine doses (P < 0.01). The result was unchanged after removing the nonsignificant ‘group by time’ interaction (i.e. the difference in change over time between groups). When only patients who were regarded as having received effective postoperative analgesia (VAS ≤ 30) were analysed, the relative effective postoperative analgesia ratios were significantly higher in the 0.50% ropivacaine group compared with the 0.12%, 0.14% and 0.16% groups (P < 0.001, P < 0.001 and P = 0.042, respectively), but there were no significant differences between the 0.18%, 0.20%, 0.22% and 0.50% groups (data not shown).
Visual analogue scale (VAS) scores for postoperative pain at 4, 8, 12 and 24 h following surgery in 103 patients who underwent elective knee arthroscopy. Postoperative pain relief was delivered as a single-shot femoral–sciatic nerve block using ropivacaine at concentrations of 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, 0.22% or 0.50%. Data presented as mean ± SD. The 0.12%, 0.14% and 0.16% concentrations were significantly different from the 0.50% concentration (P = 0.001, P = 0.008 and P = 0.025, respectively). There were no significant differences between ropivacaine at concentrations of 0.18% 0.20%, 0.22% and 0.50%; Student’s t-test or Mann–Whitney U-tes, depending on data distribution. There was a statistically significantly difference across time points (4, 8, 16 and 24 h) for all individual ropivacaine doses (P < 0.01); multivariate analysis of variance.
When data from only those patients who were regarded as having received effective postoperative analgesia (VAS ≤ 30) were analysed, the half maximal effective concentrations (EC50) and 95% maximal effective concentrations (EC95) 95% CI for ropivacaine were 0.158 (95% CI 0.149, 0.167), and 0.198 (95% CI 0.186, 0.221), respectively (Figure 2).
Effective rates of different concentrations of ropivacaine (0.12%, 0.14%, 0.16%, 0.18%, 0.20%, 0.22% or 0.50%), in single-shot femoral–sciatic nerve block for postoperative analgesia following knee arthroscopy (n = 103). The 50% effective concentration (EC50) (95% confidence interval [CI]) was 0.158 (0.149, 0.167). The 95% effective concentration (EC95), 95% CI of ropivacaine was 0.198 (0.186, 0.221); probit regression analysis.
Rates of oral ibuprofen consumption over 24 h in the 0.12%, 0.14% and 0.16% ropivacaine groups were significantly different from the 0.50% group (P = 0.002, P = 0.017 and P = 0.041, respectively). There were no significant differences between the 0.18%, 0.20%, 0.22% and 0.50% groups (data not shown).
The rates of motor blockade (Bromage score > 0 and hip motor function scale > 0) were significantly different between the 0.50% ropivacaine group and all other doses (P < 0.01). There were no significant differences between the 0.12%, 0.14%, 0.16%, 0.18%, 0.20% and 0.22% groups (Figure 3).
Rates of motor block scores > 0 using either the Bromage scale or hip motor function scale for ropivacaine in single-shot femoral–sciatic nerve block for postoperative analgesia following knee arthroscopy (n = 103). Ropivacaine was used at concentrations of 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, 0.22% or 0.50%. *P < 0.01 compared with 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, and 0.22% ropivacaine concentrations; there were no significant differences between the 0.12%, 0.14%, 0.16%, 0.18%, 0.20%, and 0.22% groups; Pearson’s χ2-test.
There were no cases of local anaesthetic toxicity or complications relating to application of the peripheral nerve block.
Discussion
The present study compared different concentrations of ropivacaine in single-shot femoral–sciatic nerve block analgesia for outpatient knee arthroscopy. The relative rate of satisfactory postoperative analgesia was significantly higher in the 0.50% group than in the 0.12%, 0.14% and 0.16% ropivacaine groups, but there were no significant differences compared with the 0.18%, 0.20% and 0.22% ropivacaine groups. Maximum VAS scores were observed 8 h following surgery in each group. The EC95 for ropivacaine ∼0.20%, and rates of motor blockade, were significantly different compared with the 0.50% group. Thus, the combined effective analgesia and motor blockade results indicated that 0.20% ropivacaine was the optimal concentration for femoral–sciatic nerve block, for postoperative analgesia in knee arthroscopy.
There are several types of postoperative analgesia for knee arthroscopy. Peripheral nerve blocks frequently continue into the postoperative period following hospital discharge, in order to optimize pain relief. 10 Due to a loss of proprioception and the protective reflex of pain, physicians are often concerned about discharging patients from hospital if they have received a long-acting peripheral nerve block of the lower extremity. 11 The present study was inspired by cases of discharged patients who were injured after falling down at home (unpublished information). One large study showed, however, that the practice of prolonging peripheral nerve blocks into the postoperative period (following hospital discharge) may be done effectively, with favourable safety findings and a high degree of patient satisfaction. 12 Based on the present study, by using an optimal concentration of ropivacaine, nerve blocks may not necessarily be a contraindication to hospital discharge. Ropivacaine, at concentrations of 0.25% and 0.50%, has been reported to provide adequate for pain relief following outpatient hernia repair, whereas 0.125% was shown to be no more effective than saline. 13 For this reason, 0.12% ropivacaine was selected as the lowest concentration, in the present study.
Several studies have used ‘up-and-down’ methods to determine the effective dose in 50% of patients (EC50), 14 as this provides a simple sequential design to determine the dose at the 50th percentile, and reduces the total number of participants needed to determine the ED50. Anaesthesiologists are interested in the ED95, which is often calculated using the isotonic regression estimator, with the CIs derived by bootstrapping. Although isotonic regression provides favourable back-up analysis for obtaining the ED50, with a smaller bias and tighter CIs compared with standard probit regression (which is likely to produce biased estimators), the extrapolation of the ED95 from small study number ‘up-and-down’ data can be imprecise. 14 Thus, groups assigned to receive different concentrations of ropivacaine in the present study were analysed using standard probit regression.
The value of sciatic nerve block combined with femoral nerve block for postoperative analgesia has been demonstrated by an improvement of postoperative analgesia following knee arthroscopy. 15 A single injection or continuous sciatic nerve block, in addition to a femoral nerve block, reduces severe pain on the day of surgery, whereas a continuous sciatic nerve block reduces moderate pain during mobilization over the first two postoperative days. 16 Another study suggested that there were no clinically important analgesic advantages for sciatic nerve block beyond 24 h postoperatively. 17 As there is inconclusive published evidence defining the effect of adding sciatic nerve block to femoral nerve block on acute pain (and related outcomes), compared with femoral nerve block alone for total knee arthroplasty or knee arthroscopy, the present study used combined femoral–sciatic nerve block to reduce bias.
Lumbar-plexus and sciatic-nerve blocks are commonly combined for lower-extremity anaesthesia, and require large doses of ropivacaine. Plasma ropivacaine concentrations increase more rapidly when a sciatic-nerve block is added to a lumbar-plexus block, but the maximum concentration remains below the toxicity threshold. 18 No local anaesthetic toxicity was observed in the present study.
Unlike physiological localization of neurostimulation techniques, ultrasound techniques use an anatomic image to determine the relative position of a nerve and a catheter. Ultrasound can provide reliable blockade, and the expansion and volume of local anaesthetics can be clearly seen. For the sake of better blinding, the present study used the optimal concentration of ropivacaine rather than the optimal effective volume of local anaesthetic or optimal dose of ropivacaine; the volume of medication used was the same for all groups.
There were some limitations to the present study. The effects of continuous nerve block in postoperative analgesia were not studied because the single-shot nerve block is convenient for daily surgery. The use of continuous nerve block should be evaluated in further investigations.
In conclusion, the EC50 and EC95 for ropivacaine in femoral–sciatic nerve block for postoperative analgesia in knee arthroscopy were 0.158 (95% CI 0.149, 0.167) and 0.198 (95% CI 0.186, 0.221), respectively, with rates of motor blockade being significantly different between the 0.20% and 0.50% doses. Ropivacaine at 0.20% used in femoral–sciatic nerve block for postoperative analgesia in knee arthroscopy may provide satisfactory postoperative analgesia and better preserve the ability of motion.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.