
Abstract
Objective
To evaluate the smallest oblique sagittal area of the neural foramen in detecting cervical spondylotic radiculopathy (CSR) and to determine its potential significance for treatment decisions.
Methods
The subjects of the study were patients with CSR who visited the spine surgery from 2016 to 2019. All patients were compared according to the minimum oblique sagittal area and the cut-off point value, and they were divided into positive and negative parameters. The changes in neck disability index (NDI), Japanese Orthopaedic Association score (JOA), and visual analog scale (VAS) during the two treatment groups from baseline to at least 24 months of follow-up were compared.
Results
In the surgery group, there was no significant difference in symptom improvement between patients with positive and negative parameters. In the non-surgical group, for patients with positive parameters, NDI decreased by 2.35, JOA increased by 0.88, and neck VAS score improved by 0.42. For patients with negative parameters, NDI decreased by 10.32, JOA increased by 2.86 on average, and neck VAS score improved by 2.46 points on average (both p<0.01 on t test).
Conclusions
Patients with both positive and negative parameters showed significant improvement in their symptoms after surgery, and the smallest oblique sagittal area of the neural foramen seems to be unable to predict the outcome of the surgery. However, in non-surgical patients, symptomatic improvement was more limited in patients with positive parameters than in those with negative parameters. This suggests that patients with positive parameters may be more suitable for surgery and those with negative parameters are more suitable for conservative treatment.
Introduction
Cervical spondylotic radiculopathy (CSR) is the most common type of cervical spondylosis. 1 In recent years, many studies have evaluated the clinical, imaging and other diagnostic criteria of CSR for better diagnosis and treatment.2-4 However, a major problem is that the imaging results are not always consistent with clinical symptoms. In the treatment of CSR, there is a lack of high-quality evidence for the efficacy of conservative treatment and surgical treatment, 5 the scientific evidence for surgical indications is limited.6-8 Guidance to clinicians is also inconsistent and inadequate.
In addition, the debate about which diagnostic criteria could help decide whether to adopt conservative treatment or surgical treatment and the choice of specific surgical procedures has been ongoing.9-11 There are many randomized controlled trials comparing the efficacy between surgery and conservative treatment of CSR.12,13 Some studies have reported the effectiveness of surgery in relieving symptoms (pain relief, satisfaction, muscle weakness improvement) has been shown to be between 80% and 95%.14-17 However, some systematic reviews have found no clear benefits of surgery over non-surgical treatments.18,19 The evidence that can be drawn from these studies is considered to be limited. Results suggest that selection criteria, observer bias, the natural course and placebo mechanisms play an important role in the reported high success rates after surgery. Although the evidences for the benefits of decompression surgery is growing, the uncertainty around the indication for surgery remains. It is not clear which patients benefit most from each strategy.
Recently, the study of Hong et al. 20 showed that nerve root compression is mainly related to the decrease in the width and area of the neural foramen. Ozaki 21 measured 1152 cases of cervical neural foramen in the oblique sagittal plane in 2019, and the report pointed out that the best cut-off value of the minimum width of the nerve root canal to diagnose cervical nerve foramen stenosis is 2.7 mm. It has certain reference value for the diagnosis of neural foraminal stenosis. Previous research 22 has shown that the smallest oblique sagittal area of the cervical neural foramen can contribute to diagnose cervical radiculopathy caused by foraminal canal bony stenosis. A cut-off value of 25.95 mm2 showed relatively high sensitivity (74.1%) for detecting bony stenosis of the neural foramen and good specificity (80.9%). The next step of the research is to measure and evaluate the clinical value of the new parameters in a representative patient population to prove whether the smallest oblique sagittal area of the neural foramen can identify patients suspected of CSR, and help determine which patients are suitable for surgery or conservative treatment
There is no recognized diagnostic standard for CSR, 23 when there is no perfect reference standard, the ideal research should be to evaluate the correlation between the measurement result and its success of the operation. 24 We designed a retrospective study of the clinical effectiveness of the smallest oblique sagittal area of the neural foramen. The purpose of this study was to determine whether this parameter can provide valuable clinical information to help formulate a treatment plan (surgery or conservative treatment). We studied the relationship between changes in parameters before and after surgery or non-surgical treatment and changes in patient symptoms.
Material and methods
This study was approved by the local ethics committee (BLY20190712). All patient data were anonymous and confidential. Verbal informed consent was obtained from participants. In brief, we evaluated the ability of this indicator to diagnose patients with suspected CSR by studying the correlation between the smallest oblique sagittal area of the neural foramen and the clinical results.
The eligibility assessment of patients who referred to our spine department was conducted between January 2016 and December 2019. Based on medical history and physical examination, including patients suspected of having CSR. The exclusion criteria are as follows: (1) Cervical neural foramen stenosis is caused by soft tissue, such as a herniated disc or ligament, rather than bone structure; (2) cervical spine instability; (3) cervical spine surgery history; (4) history of any neurological disease; (5) tumor/malignant tumor; (6) cause of trauma; (7) congenital or other skeletal dysplasia.
The imaging data used for the measurements were conventional cervical spine CTs (slice thickness: 1.000 mm, slice increment: 0.500 mm, model: Optima, manufacturer: USA), as shown in Figure 1. First, a model of the cervical spine and neural foramen is reconstructed by three-dimensional digital simulation using Mimics software (version 20.0, Materialise, Belgium), as shown in Figure 2. The second step is to select the image at the level of the neural foramen of the target segment. The plane of the intervertebral space is taken parallel to the endplate position and adjusted to the plane of the intervertebral space where the neural foramen is largest. Following this, the midline of the target vertebra is made on this plane, and a straight line is made through the neural foramen at 45° to the midline (Figure 3(a)), which is the neural foramen’s center line. In the third step, the created model and center line are copied into 3-matic software, where a series of planes perpendicular to the center line and intersecting the neural foramen are created, each with a spacing of 0.1 mm (Figure 3(b)). The neural foramen intersects these planes to produce a series of cross-sections, and the software is used to calculate the area of these cross-sections. Finally, the cross-section with the smallest area is taken (Figure 4), which is considered the smallest oblique sagittal area of the neural foramen. These procedures take approximately 45 min. CT image of a patient’s neural foramen stenosis. Three-dimensional digital simulation reconstruction model of cervical vertebra and neural foramen. a: The center line of the neural foramen. b: A series of planes perpendicular to the centerline and intersecting neural foramina model. The section interval was 0.1 mm. The smallest plane: The figure shows the measured value of the smallest oblique sagittal area of the neural foramen.



All patients were compared according to the smallest oblique sagittal area of the neural foramen and the value of the critical point (25.95mm2), and then divided into the parameter positive and negative. In other words: if the patient’s smallest oblique sagittal area of the neural foramen was less than 25.95 mm2, the parameter was positive, and if the smallest oblique sagittal area of the neural foramen was greater than 25.95 mm2, the parameter was negative.
Researchers collect patient clinical information from the medical record system, including patient medical history and self-assessment (Neck Disability Index (NDI), 25 Japanese Orthopaedic Association Scores (JOA),visual analog scale (VAS) for neck and arm pain), physical examination, and imaging (CT, MRI), and treatment programs (surgery or non-surgical treatment). And the researchers also collected the patient’s clinical follow-up information. Two other investigators independently reconstructed all imaging data retrospectively and measured all neural foramen sizes on 3-matic in the absence of clinical or surgical information. All surgeons received one-on-one guidance to ensure that they were familiar with the software program and that the measurements were consistent. They were not treating physicians of study patients and were blinded to all other clinical information. Before further analyses, discordant initial the measured results (the difference is more than 3 mm2) of the two investigators were resolved in a consensus meeting. Take the average of two measurements as the final calculated value. All data were entered into SPSS software to blind investigators to other study information.
The main outcome indicators were the changes in NDI, JOA and pain VAS between baseline and follow-up examinations. The changes in these efficacy indicators were compared between surgery group and non-surgery group. In the surgery group, patients who had no planned surgery initially but who underwent delayed decompression surgery during the follow-up period were evaluated. Secondary results include statistics on the rate of delayed surgery, as well as an evaluation of the consistency of the measurement results of the two investigators.
All data were statistically analyzed using SPSS 20.0 (PASW Statistics, IBM). In the two treatment groups, we tested for a difference in the mean within-patient change in NDI, JOA and VAS between the stenosis and non-stenosis groups using Student t test. The Kappa value was calculated to assess the inter-ethnic consistency between the measurement results of the two researchers. The statistical significance level used was 5%.
Results
Patients
Baseline patient characteristics in patients planned for surgery and no surgery.

VAS, visual analog scale; JOA, Japanese Orthopaedic Association Scores.
After the baseline assessment, 85 patients (53%) underwent surgery. The median time from baseline assessment to surgery was 1.6 months. Of the remaining 74 patients, no surgical treatment was chosen. Their treatment generally included physical therapy and oral pain medication (nonsteroidal analgesic and neurotrophic drug).
26
Of the 74 patients who did not initially choose surgery, 13 of them were revised during the follow-up period. These patients received surgery, and the median time interval between delayed surgery and baseline assessment was 8.3 months (Figure 5). Participants’ research profile.
All procedures were performed by the same team of physicians, with anterior cervical discectomy and fusion. Table 1 lists the baseline characteristics of the included patients.
Outcomes
VAS, JOA, and neck disability index measures according to sedimentation sign result, stratified by treatment group.

VAS, visual analog scale; JOA, Japanese Orthopaedic Association Scores; NDI, Neck Disabilitv Index.

Change of neck disability index in treatment groups.

Change of visual analog scale arm pain in treatment groups.

Change of visual analog scale neck pain in treatment groups.

Change of Japanese Orthopaedic Association score in treatment groups.
Among the 13 patients with delayed surgery, 5 patients were positive parameters and 8 patients were negative parameters. The median baseline NDI was 45.28, and the JOA was 7.92. Overall, the average NDI improved after delayed surgery was 25.77, JOA improved by 6.33 after delayed surgery, neck pain improved by 3.91, and arm pain improved by 4.88. There was no statistically significant difference between these changes between positive and negative parameters.
Among 61 patients in the non-surgical group, 26 patients were positive parameters and 35 were negative parameters. For patients with positive parameters, NDI decreased by 2.35 on average, JOA increased by 0.88 on average, and neck VAS score improved by 0.42 on average. For patients with negative parameters, NDI decreased by 10.32, JOA increased by 2.86 on average, and neck VAS score improved by 2.46 points on average (Table 2).
Comparison of sedimentation sign results with other diagnostic tests at baseline.
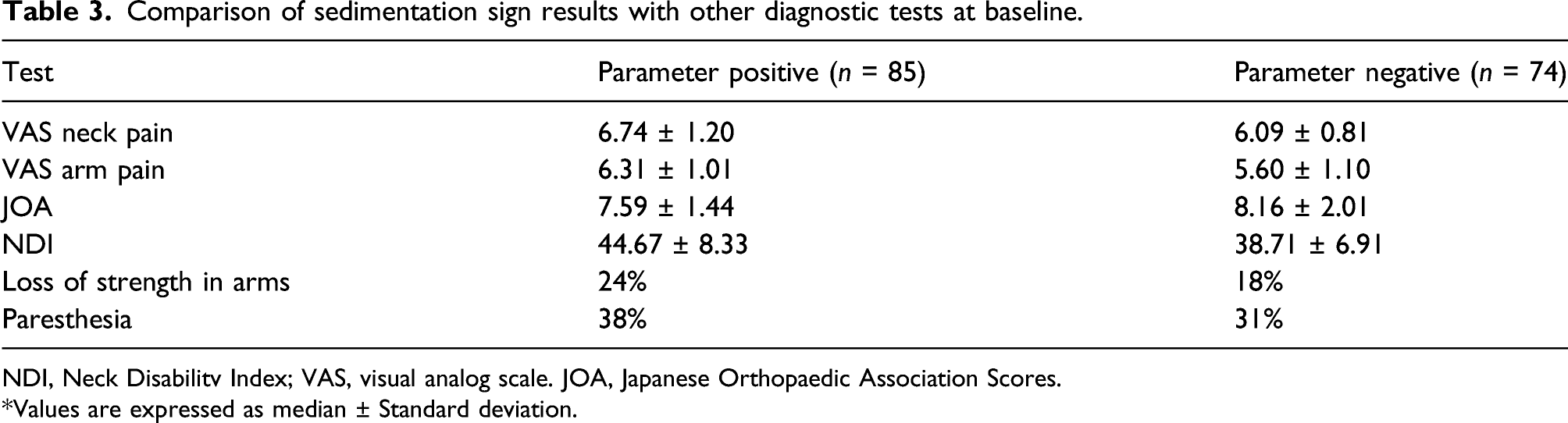
NDI, Neck Disabilitv Index; VAS, visual analog scale. JOA, Japanese Orthopaedic Association Scores.
*Values are expressed as median ± Standard deviation.
The two spine surgeons who used CT data to reconstruct the neural foramen and measure the minimum cross-sectional area agreed in 149 (93.7%). Both considered 79 patients as parameter-positive and 70 patients as parameter-negative. The resulting kappa coefficient was 0.874 ± 0.039.
Discussion
This study evaluated the clinical significance of the smallest oblique sagittal area of the neural foramen in detecting CSR. After the initial report of the parameter, which demonstrated its ability to detect CSR under ideal circumstances, 22 this study takes another step forward in the evaluation of parameters by evaluating the clinical significance of the smallest oblique sagittal area of the neural foramen in a wider group of patients. Among patients undergoing decompression surgery or non-surgical treatment, the changes in NDI, JOA, and pain between the patients with positive and negative parameters from baseline to 24 months follow-up were compared. Regardless of the parameters, the prognosis of patients in the surgery group was similar. In contrast, in the non-surgical treatment cohort, patients with positive parameters improved less than those with negative parameters. The Kappa values of the measurement data of the two researchers showed excellent agreement.
The most interesting result of this study was that there were differences in symptom improvement between patients with negative and positive parameters after receiving conservative treatment, patients with negative parameters had better symptomatic improvement after conservative treatment than those with positive parameters, but there was no similar difference between patients undergoing surgery. This suggests that patients with negative parameters are more suitable for conservative treatment and patients with positive parameters may be more suitable for surgical treatment. In addition, patients with positive parameters had higher baseline NDI, lower JOA scores, and higher levels of neck and arm pain, indicating that CSR was more severe than patients with negative parameters.
In this study, the delayed operation rate was not related to the value of the smallest oblique sagittal area of the neural foramen. In addition to the clinical severity of CSR, other factors (such as the patient’s economic level) may also play an important role in the initial surgical decision. In addition, other surgical indications, such as progressive neurological impairment, associated manifestations of cervical spondylotic myelopathy, segmental instability, and kyphosis, were the reasons for the subsequent decision of some of these patients to undergo surgery. 27
The results of this study indicate that the smallest oblique sagittal area of the neural foramen provides useful information for the diagnosis of CSR and helps identify patients who may benefit from surgery. Since almost all patients suspected of having CSR have undergone a CT examination, the measurement of this parameter does not cost extra, and its use is very simple and fast. In addition, in clinical practice, this parameter can clearly and visually convey the stenosis of the neural foramen to the patient. It is an absolute measure of neural foramen. We believe that this parameter can improve the clinical diagnosis of CSR.
Our study has some limitations. First, our study adopted a retrospective design. Second, it was a single-center study. This may limit the generalizability of our results. Multi-center prospective studies are needed to replicate and verify our results. Third, the time for follow-up examinations cannot be controlled. We accepted a follow-up interval of 22–31 months. A follow-up that is too short may not provide enough time to prove the benefits of the operation, while a follow-up that is too long may compromise the prognosis due to the degeneration of adjacent segments. Between 12 and 21 months after the baseline examination, we followed up most patients. In addition, after the initial postoperative improvement, the effect of the surgery did not seem to change over time, and a multivariate analysis of our data showed that changes in the follow-up interval did not have a significant effect on the results. Fourth, because this is a preliminary study, we did not classify patients by surgical segment. Finally, a small proportion of patients with clinically suspected CSR do not have CT examinations, which may indeed cause selection bias, and as this is a preliminary study, more detailed studies need to be designed in the future.
Further studies on the parameters of the smallest oblique sagittal area need to evaluate the applicability of our findings in different clinical settings. It is necessary to provide clinicians with more practical guidance, detailing how to interpret parameters in more complex situations (such as multi-level CSR). The clinical value of this indicator should also be evaluated in randomized controlled trials.
Conclusion
In patients who usually undergo decompression surgery, the smallest oblique sagittal area of the neural foramen does not seem to predict the outcome of the surgery. However, in conservatively treated patients, symptomatic improvement was more limited in patients with positive parameters than in those with negative parameters. This suggests that patients with positive parameters may be more suitable for surgery and those with negative parameters are more suitable for conservative treatment, but this needs to be investigated in prospective randomized trials.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.