
Abstract
Background:
Hip fractures are a common condition associated with high morbidity and mortality. In this study, we assess (1) yearly incidences, (2) demographic factors, (3) postoperative outcomes, (4) primary diagnoses, and (5) primary procedures.
Materials and Methods:
The National Inpatient Sample was queried for patients admitted with hip fractures from 2009 to 2016 (n = 2 761 850). Variables analyzed were age, sex, race, obesity status, Charlson Comorbidity Index, smoking status, osteoporosis status, lengths of stay (LOS), discharge dispositions, charges, costs, mortalities, inpatient complications, primary and secondary diagnoses, and primary procedures.
Results:
From 2009 to 2016, the overall gross number of hip fractures decreased (P < .001). At the conclusion of the study, more patients were male, obese, and smokers, while fewer had a diagnosis of osteoporosis (P < .001 for all). Mean LOS significantly decreased (P < .001), while charges and costs increased (P < .001 for both). Both mortality and the overall complication rate decreased (P < .001 for both). Specifically, complications that decreased included myocardial infarctions, deep vein thromboses, pulmonary emboli, pneumoniae, hematomas/seromas, urinary tract infections, and transfusions (P < .001 for all). Complications that increased included cardiac arrests, respiratory failures, mechanical complications, and sepsis (P < .001 for all). The most common diagnosis was “closed fracture of intertrochanteric section of neck of femur.” The procedure performed most often was “open reduction of fracture with internal fixation, femur.”
Conclusion:
An increasing number of males and smokers have sustained hip fractures, although fewer patients with osteoporosis experienced these injuries. A decreasing overall complication rate may indicate improving perioperative courses for hip fracture patients. However, several shortcomings still exist and can be improved to further decrease negative outcomes.
Background
Hip fractures are common orthopedic injuries that require substantial hospital resources, costing an estimated US$9.2 billion dollars annually in the United States. 1 This figure is expected to grow, as the annual incidence of hip fractures in the United States is projected to exponentially increase over the next several years. 2 These anticipated trends are worrisome, as this injury possesses some of the poorest outcomes in orthopedic surgery. Currently, studies estimate that 2% to 14% of patients die during the same hospital admission and 14% to 36% die within a year of their index surgery. 3 -6 Of those that survive, 58% continue to have difficulty ambulating without an assistive device at 1 year after their surgery. 7 As a consequence, the high incidence of hip fractures, coupled with the high morbidity and mortality rates, has caused this condition to become a major public health concern. In an effort to mitigate rising costs and suboptimal outcomes, studies have investigated various elements of this injury.
Risk factors have been heavily scrutinized in an attempt to implement fracture prevention strategies. As such, studies have demonstrated poor nutritional status, tobacco use, low body mass index (BMI), and the presence of osteoporosis to significantly increase fracture risk. 8 -12 Thus, providers have focused on modifiable risk factors, such as the treatment of osteoporosis and smoking cessation, as methods to reduce risk. Although helpful, these approaches have been met with limited success as the risk of fracture remains elevated despite intervention. 13,14 Studies have also reported on the importance of perioperative timing, such as the time-to-surgical-intervention and time-to-rehabilitation. If patients experience a delay in surgery beyond 48 hours, their risk of postoperative complications and death significantly increases. 15 Additionally, if patients delay postoperative ambulation past 48 hours, they experience lower survival rates, higher mortality rates, and higher postoperative complication rates. 16,17 Other studies have examined the institutional changes in how hospitals care for hip fracture patients. Hospitals are beginning to integrate medicine services to provide more global care, as many of these patients have preexisting conditions and functional deficits. 18 As a result, studies have found this approach to facilitate shorter length of stays and fewer negative outcomes. 19,20 The diversity of the aforementioned studies exemplifies the complex nature of hip fractures and illustrates the multifaceted care required to improve outcomes.
There have been a bevy of previous reports providing valuable information pertaining to hip fracture management. However, studies documenting recent national trends as a reflection of management changes have been sparse. Therefore, this study investigated the current trends in hip fractures throughout the United States. Specifically, this study utilized a large national database assessing (1) yearly incidences, (2) demographic factors, (3) post-fracture outcomes, (4) primary diagnoses, and (5) primary procedures for hip fracture patients between 2009 and 2016.
Materials and Methods
Database Selection
The utilized database, the National Inpatient Sample (NIS), is one of several publicly available databases collected by the Agency for Healthcare Research and Quality and distributed by the Health Care Utilization Project (HCUP). This database contains 20% of all inpatient hospital stays throughout the United States, representing over 7 million annual hospitalizations. 21 Once weighted, this database estimates more than 35 million hospitalizations. As a result of this database being deidentified, this study was exempt from institutional review board approval.
Patient Selection
We queried the NIS for patients who were admitted with hip fractures from January 1, 2009, to December 31, 2016. Hip fracture patients were identified by International Classification of Disease, Ninth and Tenth Revisions (ICD-9 and ICD-10) diagnosis codes. Patients included in this study possessed ICD-9 or ICD-10 codes involving fractures of the femoral head, neck, intertrochanteric, and subtrochanteric regions, yielding 2 761 850 patients. Exclusion criteria included patients sustaining isolated acetabular fractures, pelvic fractures, and femoral shaft fractures.
Study Variables
Patient demographics included age, sex, race, obesity status, Charlson Comorbidity Index (CCI) rank, smoking status, and osteoporosis status. Race was categorized into Caucasian, African American, Hispanic, Asian or Pacific Islander, Native American, or other. Patients were considered obese if they possessed the proper diagnosis codes pertaining to obesity status, while any entry without a code was considered nonobese. As the NIS does not provide BMI status, obese patients were obtained by querying the database with the respective ICD-9 (278.00, 278.01) and ICD-10 (E66.0, E66.01, E66.9) diagnosis codes. The CCI is a weighted index meant to predict risk of death within 1 year of hospitalization in patients with 19 specific comorbid conditions. 22 Each patient had their CCI calculated utilizing diagnosis codes within the NIS and were subsequently categorized into CCI scores of 0, 1, 2, or 3+.
Postoperative outcomes included lengths of stay (LOS), discharge dispositions, charges, costs, mortalities, and inpatient complications. Additionally, primary diagnoses, secondary diagnoses, and primary procedures were recorded. Discharge dispositions included home discharges, discharges to short-term hospitals (critical access hospitals, cancer centers, and federal health care facilities), discharges to other facilities (skilled nursing, intermediate care, inpatient rehabilitation, long-term care hospitals, and hospice), discharges home with home health care, and discharges against medical advice. Cost was defined as the dollar amount accrued by the hospital for the duration of the patient’s hospital stay and were estimated using the supplemental “Cost-to-Charge Ratio” files provided by the HCUP. Charges were defined as the dollar amount billed by the hospital to the primary payer. The data regarding total charges is available within the NIS database, as it is a data element gathered by the HCUP. Obtained charges and costs were adjusted using the January 1, 2019, consumer price index. Inpatient complications included myocardial infarctions (MIs), cardiac arrests, deep vein thromboses (DVTs), pulmonary emboli (PEs), respiratory failures, pneumoniae, hematomas/seromas, mechanical complications, sepsis, urinary tract infections (UTIs), and blood transfusions. Mechanical complications consisted of any fracture, loosening, dislocation, or mechanical breakdown of implants.
Statistical Analysis
Chi-squares were utilized for categorical variables, while student t tests and 1-way analyses of variance and were utilized for continuous variables. All data were examined using the 25th version of the SPSS (IBM Corporation). Statistical significance was set to a P value of less than .05.
Results
Patient Demographic
The gross number of hip fractures fluctuated over the study period, although an overall decrease was observed, with 339 786 patients having hip fractures in 2009 and 335 860 in 2016 (P < .001; Table 1). The mean age of patients decreased throughout the study (78-77 years), and the proportion of males significantly increased (+2.2%; P < .001 for both). Caucasians were the most common race having hip fractures, consistently comprising greater than 85% of all hip fractures. Furthermore, there were increases in the proportion of African Americans (+0.7%) and Hispanics (+0.2%) and decreases in Native Americans (−0.2%) and other races (−0.5%; P < .001). The proportion of obese patients significantly increased (+1.7%; P < .001). The most common CCI, 3+, comprised over 90% of hip fracture patients and increased (+0.1%; P < .001). Significantly more patients were smokers (+3.2%) and less patients had a diagnosis of osteoporosis (−4.0%; P < .001 for both).
Demographics of Patients Sustaining Hip Fractures From 2009 to 2016.

Postoperative Outcomes
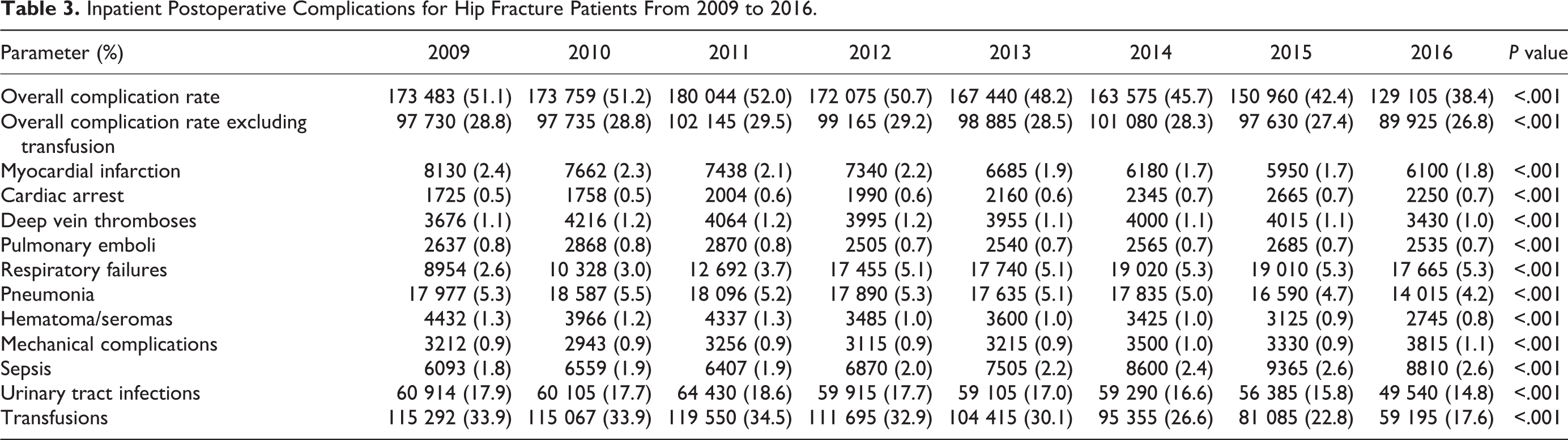
From 2009 to 2016, mean LOS decreased from 6.30 to 5.64 days (P < .001). Charges increased by US$17 984.93 (P < .001) and costs increased by US$1027.32 (P < .001), while mortality decreased (−0.5%; P < .001; Table 2). Discharges to other facilities, the most common disposition, increased (+0.5%), as did home health care (+0.9%), while home discharges (−0.4%) and discharges to short-term hospitals (−0.6%) decreased (P < .001). The overall complication rate significantly decreased by 12.8% (P < .001; Table 3). Complications that significantly decreased included MIs (−0.6%; P < .001), DVTs (−0.l%; P < .001), PEs (−0.1%; P < .001), pneumonia (−1.1%; P < .001), hematomas/seromas (−0.5%; P < .001), UTIs (−3.1%; P < .001), and transfusions (−16.3%; P < .001). Complications that significantly increased included cardiac arrests (+0.2%; P < .001), respiratory failures (+2.7%; P < .001), mechanical complications (+0.2%; P < .001), and sepsis (+0.8%; P < .001).
Postoperative Outcomes in Hip Fracture Patients From 2009 to 2016.

a Short-term Hospitals include critical access hospitals, cancer centers, and federal health care facilities.
b Other facilities include skilled nursing, intermediate care, inpatient rehabilitation, long-term care hospitals, and hospice
Inpatient Postoperative Complications for Hip Fracture Patients From 2009 to 2016.
Diagnoses and Procedures
The most common ICD-9 and ICD-10 fracture diagnoses were “closed fracture of intertrochanteric section of neck of femur” (n = 863 154) and “displaced intertrochanteric fracture of left femur, initial encounter for closed fracture” (n = 76 365), respectively (Table 4). The most common ICD-9 and ICD-10 secondary diagnosis was “acute hemorrhagic anemia” (ICD-9: n = 277 656; ICD-10: n = 47 540; Table 5). The most common ICD-9 and ICD-10 primary procedures performed were “open reduction of fracture with internal fixation, femur” (n = 617 506) and “reposition left upper femur with internal fixation device, open approach” (n = 33 145), respectively (Table 6).
Primary Diagnosis of Hip Fracture Patients.

Abbreviations: ICD-9, International Classification of Disease, Ninth Edition; ICD-10, International Classification of Disease, Tenth Edition; N, number.
Secondary Diagnosis of Hip Fracture Patients.
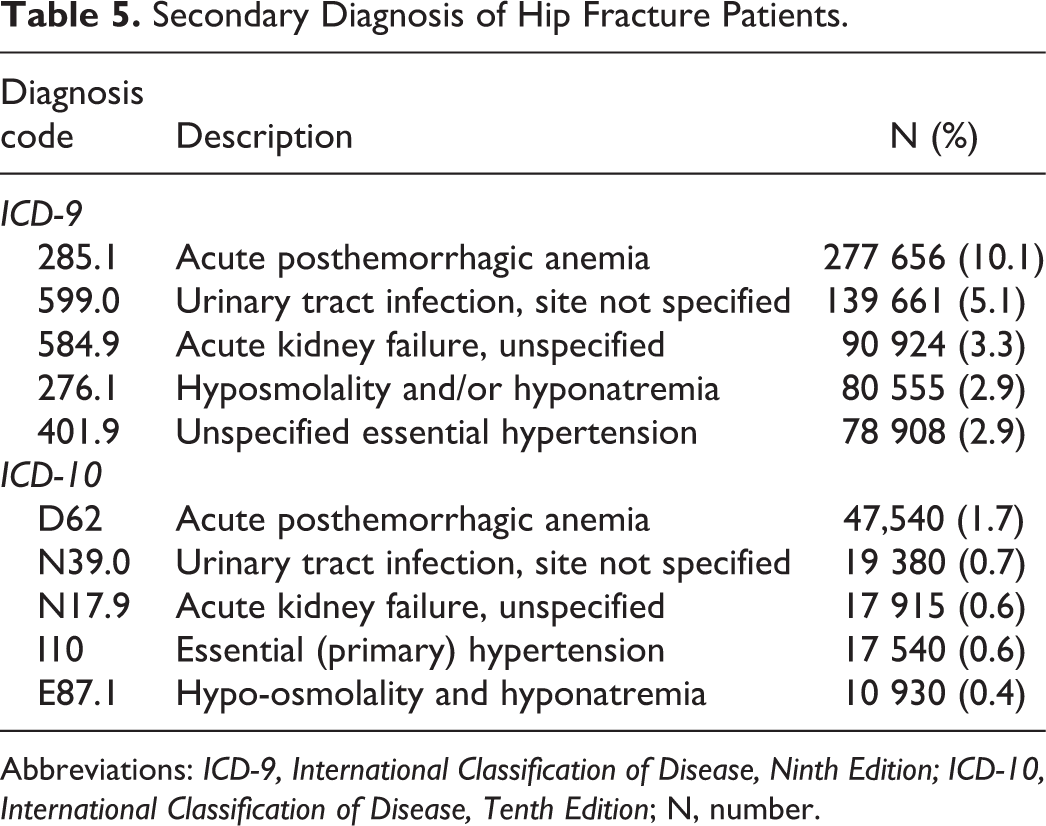
Abbreviations: ICD-9, International Classification of Disease, Ninth Edition; ICD-10, International Classification of Disease, Tenth Edition; N, number.
Primary Procedure of Hip Fracture Patients.

Abbreviations: ICD-9, International Classification of Disease, Ninth Edition; ICD-10, International Classification of Disease, Tenth Edition; N, number.
Discussion
Hip fractures continue to pose problems for elderly populations in the form of poor outcomes. The current study utilized the NIS to assess incidence, demographics, postoperative outcomes, and the most common diagnoses and procedures. Hip fracture incidence fluctuated throughout the study but ended up grossly decreasing from 2009 to 2016, which contrasts with previous studies projecting increases in hip fracture incidence in the United States. An increasing number of males, smokers, and obese individuals experienced hip fractures. Additionally, the mortality and overall complication rate of hip fractures decreased. Specifically, rates of MIs, DVTs, and transfusions decreased, while rates of cardiac arrests, mechanical complications, and sepsis increased. The most common primary diagnosis overall was “closed fracture of intertrochanteric section of neck of femur” and the most common primary procedure was “open reduction of fracture with internal fixation, femur.” Several trends observed in this study support the notion of improved perioperative management. Although these results cannot be directly linked to any particular intervention, the large number of previous hip fracture studies has likely influenced these trends.
This study is not without limitations. Our data set is highly dependent upon ICD diagnoses and procedures, and as the study period contains the transition between ICD-9 and ICD-10 coding systems, discrepancies may exist. Furthermore, some procedure codes, such as “open reduction of fracture with internal fixation, femur” are somewhat ambiguous and subject to interpretation based on physician preference. Accordingly, physicians may consider cephalomedullary nail placement open reduction internal fixation whereas another provider may not. Additionally, with the utilization of the NIS database, we were subjected to the inpatient stay only and unable to track patient data post-discharge. Despite these limitations, this study was able to provide valuable inpatient trends regarding hip fracture management.
Low velocity hip fractures are regarded as an osteoporosis-related or fragility fracture, as risk for this type of fracture dramatically increases with each decrease in standard deviation of bone mineral density. 23 In the present study, the proportion of individuals sustaining hip fractures with a diagnosis of osteoporosis decreased by a rate of 19.5% from 2009 to 2016 (20.5%-16.5%). This decline may be a reflection of updated screening recommendations from the U.S. Preventive Services Task Force in 2011 pertaining to postmenopausal females. 24 However, the group did not provide recommendations for males as there was insufficient evidence demonstrating its efficacy. These recommendations, or lack thereof, may explain the decreasing number of osteoporotic hip fracture patients and increasing number of males sustaining hip fractures. The latter trend should not be taken lightly, as males have demonstrated increased mortality rates at 1 year with comparison to females. 25,26 Instead of improved hip fracture screening and prevention as the reason for decreasing osteoporotic fractures, this downward trend may be a representation of worsening osteoporosis detection. In a trend study performed by King and Fiorentino, 27 the authors analyzed Medicare claims for dual-energy X-ray absorptiometry (DEXA) scans from 2002 to 2010. The authors noted a downward trend in utilization from 2007 to 2010, attributing the decrease to a 56% reduction in Medicare reimbursement for DEXA scans that occurred from 2006 to 2010. As a result, an estimated 800 000 fewer scans were performed, which would have prevented a projected 12 000 fragility fractures. Furthermore, in a study performed by Amarnath et al, 28 the authors investigated osteoporosis screening from 2006 to 2012, concluding that over 40% of women aged 65 to 74 and nearly 60% of women greater than age 75 fail to receive proper osteoporosis screening. Moreover, in an institutional study performed by Antonelli et al, 29 the authors examined how frequently patients underwent osteoporosis workup following a hip fracture, determining only 10.3% of patients received proper screening and 19% of patients received treatment for their presumed osteoporosis. These conclusions are noteworthy, as studies have demonstrated a higher than 2-fold increase in risk of subsequent fracture after the initial fragility fracture. 30 The shortcomings in the detection of osteoporosis may be the reason fewer individuals diagnosed with osteoporosis are sustaining hip fractures. Therefore, osteoporosis detection may be a focus for improvement to continue decreasing hip fracture incidence.
Over the course of the study, the proportion of hip fracture patients that smoked increased from 9.1% in 2009 to 12.3% in 2016. Although meta-analyses have clearly demonstrated smokers to be at heightened risk of hip fractures, this trend is somewhat surprising, particularly as the proportion of smokers in the United States has been decreasing since 2005. 31 -34 This trend should not be overlooked, as Solbakken et al 35 demonstrated hip fracture patients who smoked have a greater than 3-fold increase in mortality risk. As the 45 to 64 age-group in the United States constitutes the largest proportion of current smokers, the number of smokers sustaining hip fractures may continue to rise as these individuals grow older and the amalgamation of risk increases. 9,36 Thus, heightened efforts must be taken to encourage smoking cessation in this age group to minimize not only the risk of fracture but also the risk of mortality.
The current study reported a decreasing mortality rate from 2.9% in 2009 to 2.4% in 2016. Although a number of reports have investigated mortality rates in hip fracture patients, very few have analyzed inpatient mortality in a temporal manner like the present study. In a 2007 HCUP Report, 37 inpatient mortality rates of femoral neck fractures were estimated at 2.81%. In a database study, Kiriakopoulos et al 38 investigated mortality rates in individuals having intertrochanteric fractures and noted the overall inpatient mortality rate to be 1.7% from 2005 to 2010, with males possessing significantly higher mortality rates than females (2.56% vs 1.39%; P < .0002). It should be noted that these investigations report different mortality rates as they examine patients with different anatomical fractures. Accordingly, studies reporting hip fracture mortality should be perceived with caution as a large number of factors, such as anatomical location, sex, time-to-operation, or the presence of certain comorbidities contribute to the variability seen with this rate. 39,40 The present study reports on patients with femoral neck and intertrochanteric fractures, in addition to femoral head and subtrochanteric fractures, and our mortality rates align similarly with the previous reports. As such, the decreasing rate may be a result of improving patient optimization and/or perioperative course.
Beyond patient specific factors, institutions have implemented programs that care specifically for hip fracture patients. One such program that has been investigated, called the “Fracture Liaison Service” (FLS), focuses on providing fracture prevention services, such as osteoporosis workup or education on tobacco use, in order to minimize risk of negative outcomes. 41 In a systematic review and meta-analysis performed by Wu et al, 42 the authors analyzed 74 studies comparing FLS with the usual standard of care (SOC). The authors noted significant increases in DEXA scans (FLS: 48.0% vs SOC: 23.5%) and subsequent treatment initiation (38.0% vs. 17.2%), as well as decreases in subsequent fractures (6.4% vs 13.4%) and overall mortality (10.4% vs 15.8%) in patients cared for under the FLS. Another similar version, the Ortho-Geriatric Care approach, is comprised of 3 models (routine geriatric consultation, geriatric ward, and shared care models) that involve varying levels of comanagement between orthopedic surgeons and geriatricians. 18 -20 In a systematic review and meta-analysis performed by Grigoryan et al 18 , the authors analyzed 18 studies comparing Ortho-Geriatric Care models to the usual SOC. The authors noted significant reductions in inpatient (relative risk [RR]: 0.60; 95% CI: 0.43-0.84) and long-term mortality (RR: 0.83; 95% CI: 0.74-0.94), while a decrease in mean LOS (−0.25; 95% CI: −0.44 to −0.05) was also observed. Interventions emphasizing better coordination and communication, such as the previously mentioned models, may be the future standard of hip fracture care in the United States, as represented by the decreased mortality and overall complication rates in the present study.
Looking past institutional changes, studies have explored health care payment models and their effects on hip fracture patients. One such approach that has been gaining attention is the bundled payment model. This initiative involves expanding the episode of care up to 90 days posthospital-discharge to improve care quality by increasing the coordination of care between providers. 43 In a Taiwanese database study performed by Tung et al, 44 the authors investigated bundled payments within the confines of a single-payer health care model and assessed the impact it had on hip fracture patients. After bundled payment implementation in 2010, the authors noted a decrease in all-cause 30-day unplanned readmission rates (14.0%-12.9%) and mean LOS (9.0-8.1 days). However, no decrease was observed with regard to mortality. The health care systems between Taiwan and the United States differ, yet an increasing number of states are adopting bundled payment models in order to reduce cost and improve outcomes. Although the Centers for Medicare and Medicaid has recently withdrawn a program mandating bundled payments for hip fractures, revisions to make the program voluntary, shorten the episode of care, or appropriately define the bundled payments to address unexpected costs may make this model a viable option for hip fractures in the future.
Conclusion
Hip fractures continue to demand a large portion of orthopedic resources in the United States. The present study demonstrated an overall decrease in the number of hip fractures, as well as shorter length of stays. Furthermore, patients experienced a decrease in mortality and overall complication rates. These results contrast with previous studies projecting exponential increases in hip fractures throughout the United States and may be an indication of improving perioperative courses for patients. However, this article also identified several areas in the prevention and management of hip fractures that can be improved to further reduce negative outcomes. As such, future investigations should examine which patient-specific factors pose the greatest risk of postoperative morbidity and mortality, and whether the utilization of programs, such as the FLS, mitigates postoperative risk of these certain populations. This will allow providers to tailor postoperative care specific to patients, thereby increasing the likelihood for successful outcomes following this devastating injury.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.