
Abstract
Introduction
Malignant soft tissue tumors are rare tumors representing <1% of all malignancies. As these tumors are rare, it is not uncommon that malignant soft tissue tumor excision is performed without the required preoperative imaging, staging, or wide resection margins for sarcomas. The purpose of this study was to investigate the characteristics of patients with undergoing unplanned excisions. Risk factors for tumor recurrence and mortality in patients treated with unplanned excisions were also analyzed.
Methods
Forty-nine patients who underwent unplanned excision at other hospitals and additional wide excision at our hospital between January 2002 and December 2018 were identified. Among them, 42 patients with follow-up for more than 1 year were included in this retrospective study. The relationships between sex, age, tumor depth, histological grade, location, size, surgical margin at additional wide excision, residual tumor, reconstruction, kind of hospital where the primary excision was done (sarcoma vs non-sarcoma center), preoperative examination, chemotherapy, radiation therapy, and oncological outcomes were statistically analyzed.
Results
Mean patient age was 57.3 years (15–85 years) and the mean observation period was 72.5 months (14–181 months). This analysis showed 53.8% tumors that underwent unplanned excisions were small (<5 cm) and 70.7% tumors were superficial. Multivariate analysis revealed that a positive margin during additional wide excision was significantly associated with a lower 5-year LRFS (p < 0.01).
Conclusion
Most of the tumors underwent unplanned excisions were small (<5 cm) and superficial. Surgeons should be aware that a positive margin during additional wide excision is an independent risk factor for local recurrence.
Introduction
Malignant soft tissue tumors are rare tumors accounting for <1% of all malignancies. 1 Owing to the rarity, it is not uncommon that malignant soft tissue tumor excisions are performed without the required preoperative imaging, staging, or wide resection margins for sarcomas. 2 “Unplanned excision” was first described by Giuliano and Eilber, 3 who raised caution regarding the presence of gross residual tumor tissue after unplanned excision. Later, Noria et al. 4 modified the definition of “unplanned excision” to include any tumor surgically manipulated without preoperative imaging or regard for the necessity to resect the tumor with a margin of normal tissue. Because malignant soft tissue tumors are rare and unsuspected, inadequate or inappropriate evaluation and treatment by plastic, general, and orthopedic surgeons are common. 5 In general, unplanned excisions are performed for superficial tumors; however, sometimes, it is also performed for deep tumors such as tumors in the muscles or bones. Patients with larger, deeper tumors tend to be referred to specialized tumor centers while those with smaller, more superficial tumors are more likely to undergo an unplanned excision. However, there are only a small number of studies investigating characteristics of the tumors which were treated by unplanned excisions.2–4 Furthermore, there are only small numbers of studies investigating risk factors for clinical outcomes.5–7 The purpose of this study was to investigate the characteristics of patients with undergoing unplanned excisions. Risk factors for tumor recurrence and mortality in patients treated with unplanned excisions were also analyzed.
Materials and methods
A non-controlled retrospective analysis was conducted based on data obtained from medical records. The authors did not and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article. This study was approved by ethics committee of our hospital. Informed consent was obtained from the patients.
Flow diagram chart with clear inclusion and exclusion criteria.

All statistical analyses were conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). Survival curves were generated using the Kaplan–Meier method and compared using the log-rank test. For each survival outcome (LFRS, DMFS, or OS), Cox regression analysis was used for multivariate analysis and was built using a selection of four of the lowest p-values. Results with p-values <0.05 were considered to indicate statistical significance.
Results
Characteristics of patients with undergoing unplanned excisions
Mean patient age was 57.3 years (15–85 years) and the mean observation period was 72.5 months (14–181 months). Sixty-nine percent (29 in 42) of the tumors were located in the subcutaneous tissue. There were 38 high-grade tumors and four low-grade tumors. Six tumors were located in the upper extremities, 24 in the lower extremities, and 12 in the trunk. Mean tumor size was 5.3 cm (0.8–20 cm, Figure 1). Histology of the tumors included undifferentiated pleomorphic sarcoma (UPS) or malignant fibrous histiocytoma (MFH) in 12, liposarcoma in nine, myxofibrosarcoma in seven, leiomyosarcoma in three, synovial sarcoma in three, fibrosarcoma in two, and others in six. Surgical margin after additional wide excision was positive in 10 cases and negative in 32 cases. Pathological examination of the specimens showed that 34 of the 42 cases (80.9%) had residual tumor after primary tumor excision. Fourteen patients (33.3%) required reconstruction including that using skin grafts (n = 11), free flaps (n = 5), pedicled flaps (n = 3), and other procedures (n = 3). Of the 42 patients, 10 had undergone preoperative MRI. Among these patients, only one underwent contrast-enhanced MRI. No patients had a preoperative biopsy. Ten patients received chemotherapy, while no patient received radiotherapy during follow-up (Table 2). The unplanned excisions were performed by orthopedic surgeons in 18 cases, by general surgeons in eight, plastic surgeons in seven, dermatology surgeons in two, a urology surgeon in one, and a vascular surgeon in one (Figure 2). Four of the primary surgeries (9.5%) were performed at a sarcoma center (Figure 3). Histologically, residual tumors were observed in 84.2%, and positive margins after additional wide excision were found in 36.8% of the patients with UPS/MFH and myxofibrosarcoma (Table 3). Fourteen tumors (53.8%) that underwent unplanned excisions were small (<5 cm). Patients characteristics+. UPS; Undifferentiated pleomorphic sarcoma, MFH; Malignant fibrous histiocytoma. Our data showed that unplanned excisions were performed most frequently at the general orthopedic department, followed by the general surgery department and the plastic surgery department. Thirty-seven of the unplanned excisions (88.1%) were performed in general, non-sarcoma centers. The relationship between histology, residual tumor, and positive margin at additional wide excision. UPS; Undifferentiated pleomorphic sarcoma, MFH; Malignant fibrous histiocytoma.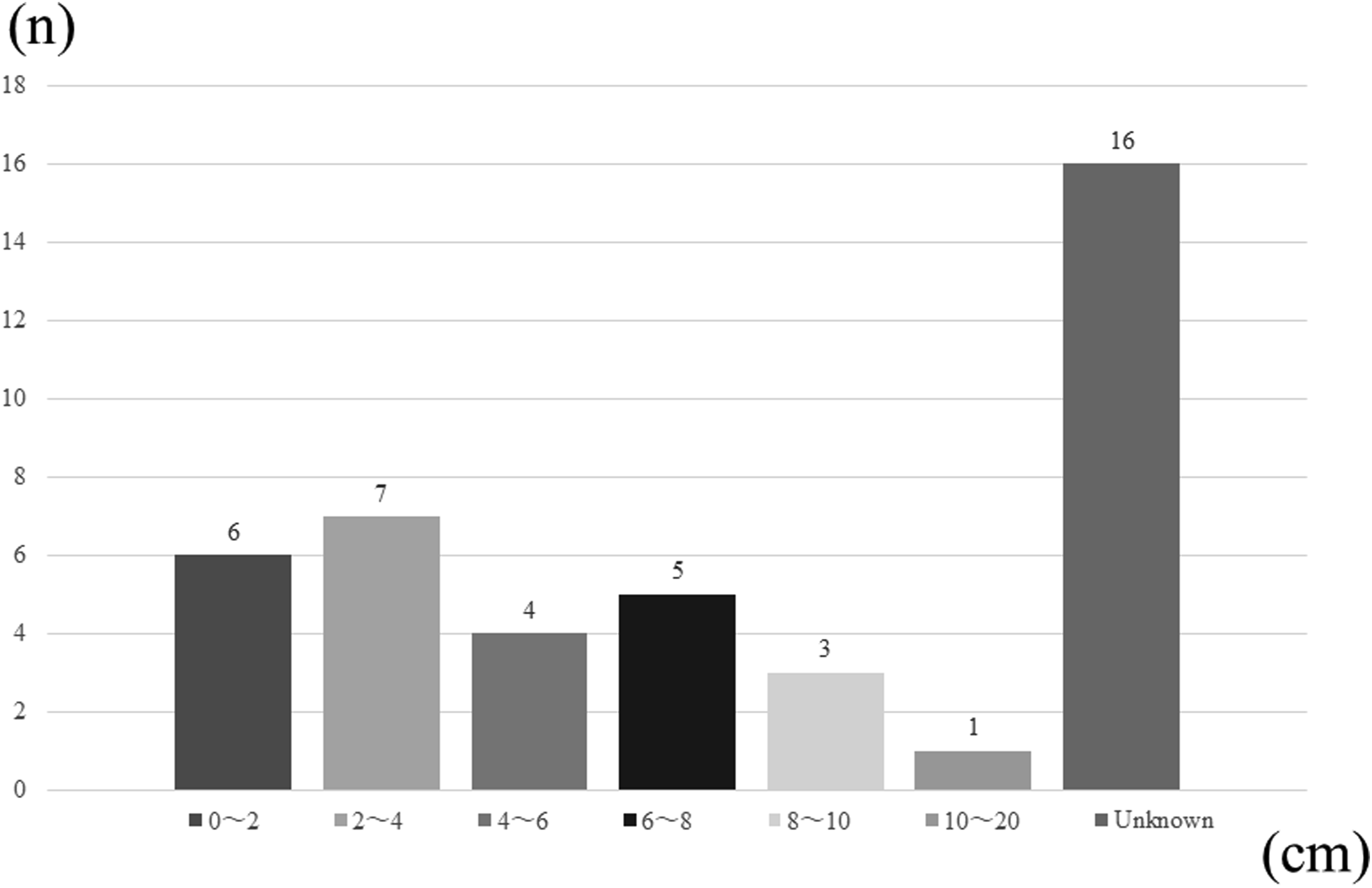




Recurrence and survival
Local recurrences were encountered in 21 patients (50%). Distant metastases were developed in 12 patients (28.6%). The 5-year LRFS, DMFS, and OS rates were 53.7%, 71.7%, and 90.3%, respectively.
Risk factors for tumor recurrence and mortality in patients treated with unplanned excisions
Oncological outcomes of the patients in the unplanned excision for locoregional recurrence-free survival (LRFS).
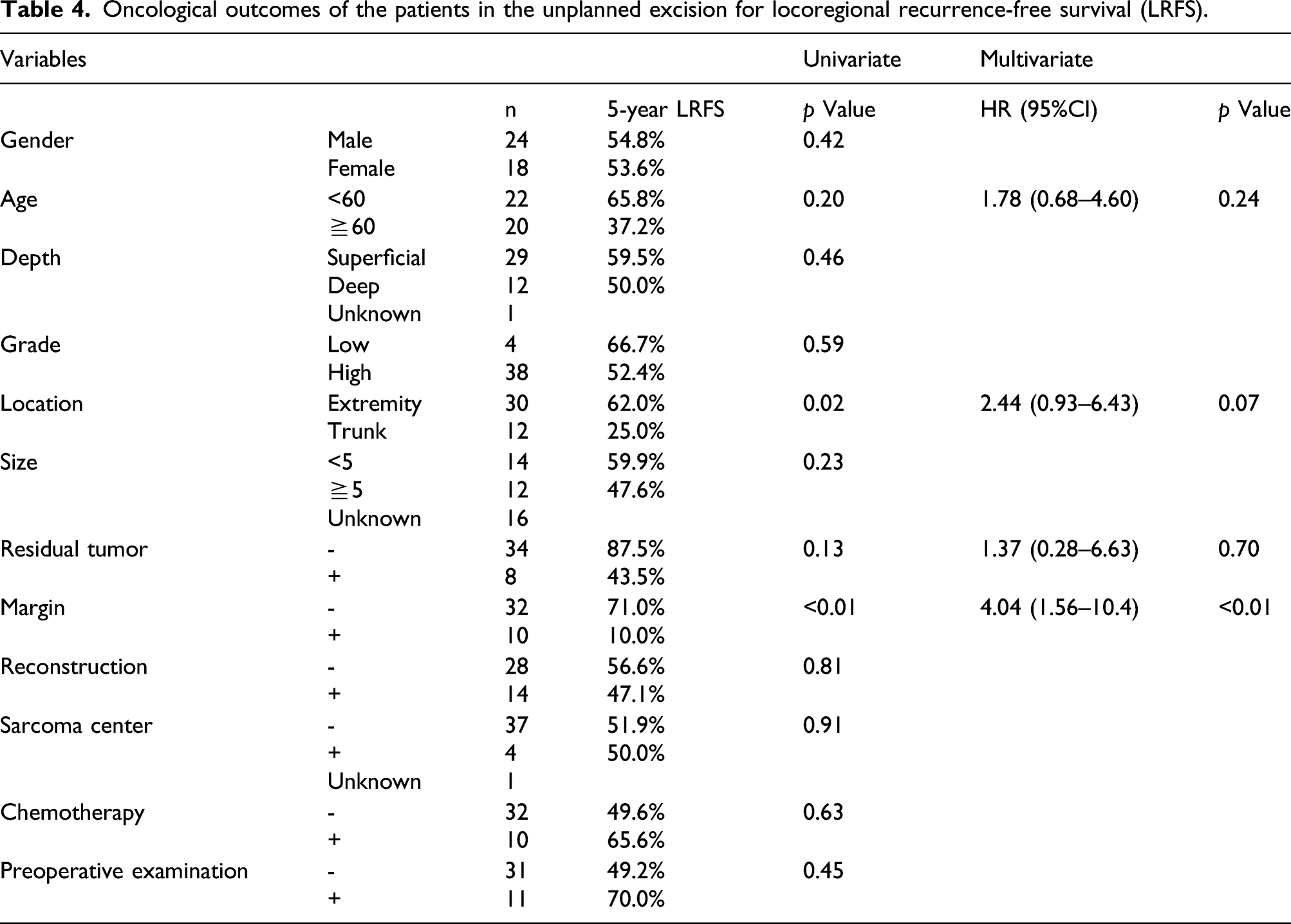
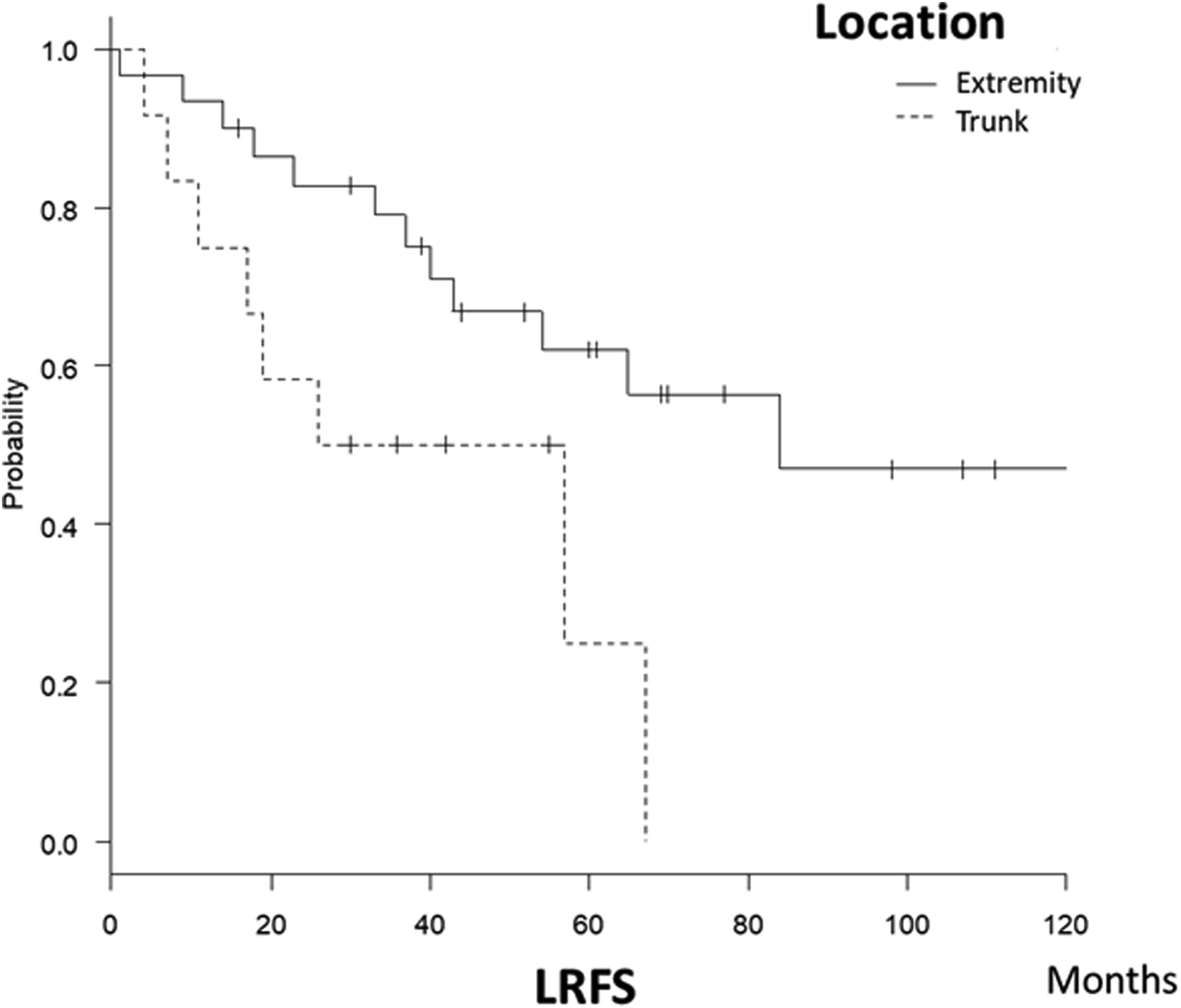
Trunk tumors (p=0.02) were significantly more likely to cause recurrence (5-year LRFS) in univariate analysis.
Oncological outcomes of the patients in the unplanned excision for distant metastasis-free survival (DMFS).

NA; Not available.

The group that needed reconstruction was significantly more likely to have distant metastasis (p=0.01) in univariate analysis.
Oncological outcomes of the patients in the unplanned excision for overall survival (OS).
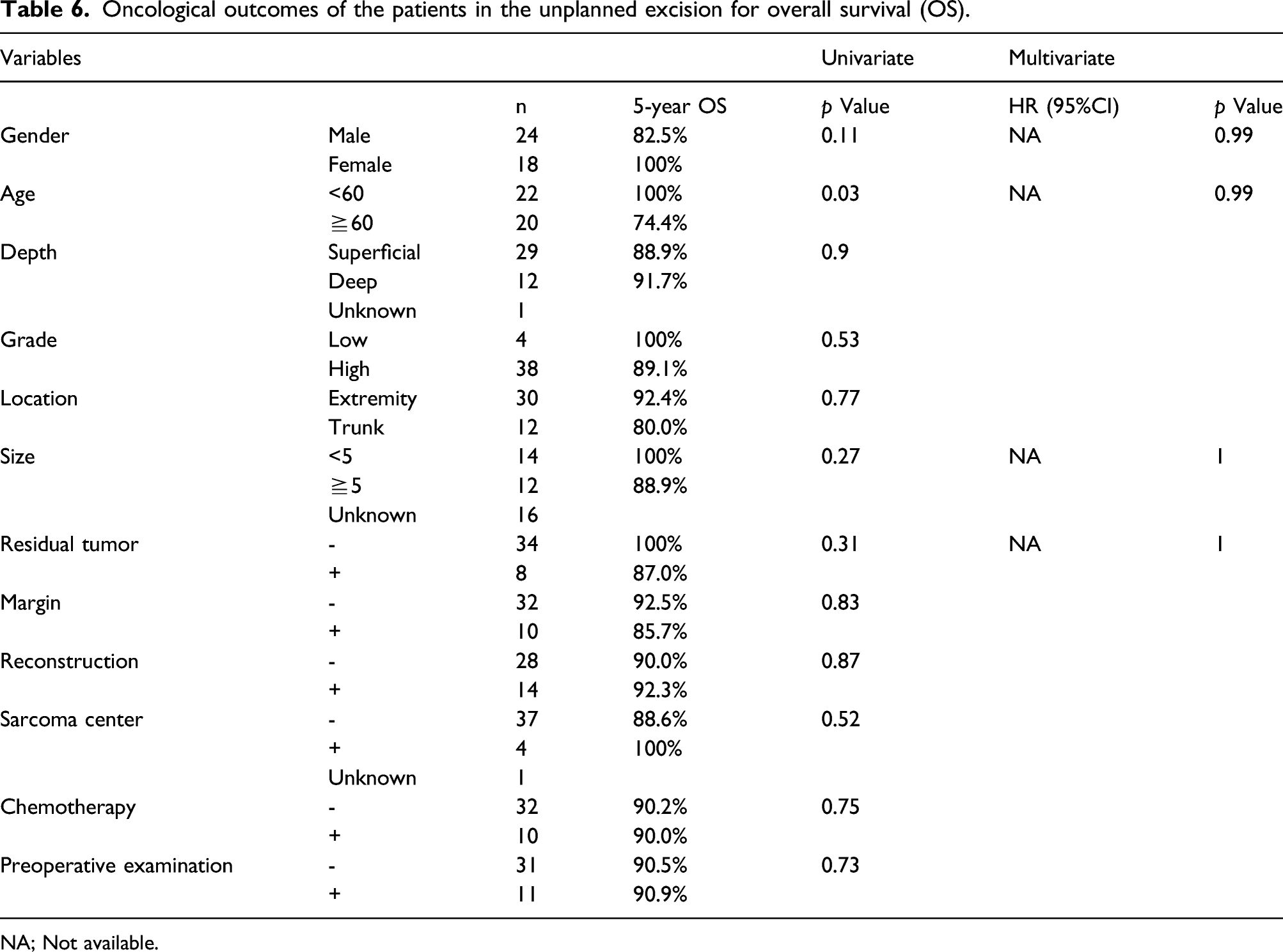
NA; Not available.

Multivariate analysis revealed that a positive surgical margin (hazard ratio 4.04, 95% confidence interval 1.57–10.4, p<0.01) was significantly associated with a lower 5-year recurrence-free survival.
Discussion
Previous studies have reported that the incidence of unplanned excision ranges from 33% to 53%.5,10–12 Unplanned excisions are performed frequently, and it is important to inform surgeons about the risks associated with such procedures. Some authors described that a positive surgical margin was an independent risk factor for recurrence.13,14 Similarly, our study observed a significant association between a positive surgical margin and lower recurrence-free survival.
Several reports suggest that a soft tissue mass should be suspected as being malignant if large (>5 cm), increasing in size or located deep to the facia.15,16 Hung et al. 17 performed an ultrasound study of 714 superficial soft tissue masses which included 247 mases with a histological diagnosis, of which 11 (4.5%) were malignant. However, previous studies have reported that most of the unplanned excisions are performed for small and superficial tumors.18,19 This analysis also showed that 53.8% tumors that underwent unplanned excisions were small (<5 cm) and 70.7% tumors were superficial. Thus, to reduce the number of cases of unplanned excision, surgeons should understand that small, subcutaneous tumors may be malignant.
Previous studies have reported that reconstruction after planned wide excision was required for 5–47% of cases; however, reconstruction after additional wide excisions was required for 30–71% of cases.11,20 In our study, 14 patients (33.3%) required reconstruction after unplanned excisions. Unplanned excisions performed in the other hospital caused tumor contamination, which created the need for a wider re-excision area to obtain a negative surgical margin.11,21,22 Moreover, univariate analysis of this study showed that the group that needed reconstruction was significantly more likely to have distant metastasis. Some authors reported that larger tumor size was a poor prognostic factor for distant metastasis.23,24 In our analysis, reconstruction may be needed for larger tumors.
As other authors described that patients had unplanned excisions in non-sarcoma centers and were referred to sarcoma centers,9,25 in this study, almost all unplanned excisions (88.1%) were performed in general, non-sarcoma centers. Although Alamanda et al. 25 reported that the incidence of an unplanned excision of soft tissue sarcoma is not influenced by patient distance from a sarcoma center, Mankin et al. 26 reported that the rate of errors, complications, and adverse patient outcomes were 2–12 times greater (p <0.001) for biopsies performed at community facilities than for those performed at sarcoma centers. Unplanned biopsy or excision can lead to significant adverse effects. Therefore, if soft tissue sarcoma is suspected, referral to a specialized facility is recommended before invasive procedures such as biopsies are performed. Further, previous studies have reported that unplanned excisions were performed most frequently by the general orthopedic department, followed by the plastic and general surgery departments.19,22,27 Similarly, our data showed that unplanned excisions were performed most frequently at the general orthopedic department, followed by the general surgery department and the plastic surgery department. Noria et al. 4 compared the outcomes between planned and unplanned excisions. They found that local recurrence was considerably higher in the unplanned excision group because of the increased difficulty in obtaining wide surgical margins during re-excisions secondary to extensive tumor contamination of the primary surgical bed. Qureshi et al. 28 reported that patients who underwent unplanned excision had worse LRFS than those who underwent planned excision. Saeed et al. 29 also reported that patients who received unplanned excision had worse LRFS and progression-free survival than those who received planned excision. Moreover, several reports suggest worse oncological outcomes in terms of local recurrence and metastasis for unplanned excisions.3,5,12,13,20,30,31 Morii et al. 22 reported that unplanned excisions should be avoided for several reasons: the definite risk of microscopic residual tumors in unplanned excision cases resulting in worse prognosis and oncological outcomes; difficulty in defining the margins during additional wide resections 4 ; and inconvenience for patients having to undergo more operations, and incurring further expenses. 25 Hence, surgeons in different specialties, including orthopedic surgeons, should be aware of the risks associated with unplanned excisions.
Another problem with unplanned excision is that there are many cases where MRI or biopsy is not performed before surgery. Hoshi et al. 32 reported that only 21% of patients who received unplanned excision had an MRI performed before primary surgery. Our study revealed that MRI before unplanned excision was performed only in 23.8% of the cases. Without an MRI before primary tumor excision, accurate spread of the tumor cannot be determined and a proper wide resection cannot be performed. Gadolinium enhancement has been reported to improve diagnostic accuracy 33 and is especially helpful in assessing masses located deep into the fascia. 18 In our analysis, contrast-enhanced MRI was performed in only 2.4% of the cases.
An infiltrative growth pattern has been reported in both UPS/MFH and myxofibrosarcoma.34,35 Nakamura et al. 36 reported that more than 70% patients with myxofibrosarcoma and UPS/MFH have residual tumors. In our study, residual tumors were observed in 84.2% and positive margins after additional wide excision in 36.8% of the patients with UPS/MFH and myxofibrosarcoma. These results reflect the invasive nature of UPS/MFH and myxofibrosarcoma, and surgeons should be careful about these tumors during primary excision and additional wide excision. Our data showed that positive surgical margins after additional wide excision were significantly related to high recurrence rates. This might be due to the failure to recognize the nature and extent of the tumor without contrast-enhanced MRI and biopsy before the primary surgery.
Our study had some limitations. First, the study design was retrospective. Prospective studies of unplanned excisions were ethically impossible. Second, the study had a small sample size because most of the surgeries for malignant soft tissue tumors are planned surgery. Third, information about the tumors could not be obtained from hospitals where the primary excision was performed. Lastly, an analysis of a planned excision group was not conducted. It is difficult to compare outcomes between planned excision group and unplanned excision group because factors such as mean tumor size or depth are so different. In our group, propensity score matching will be planned to compare them.
In summary, this study analyzed the clinical characteristics of unplanned excisions. This analysis showed that 53.8% tumors that underwent unplanned excisions were small (<5 cm) and 70.7% tumors were superficial. Risk factors for tumor recurrence and mortality were also analyzed. Surgeons should be aware that a positive margin during additional wide excision is an independent risk factor for local recurrence.
Footnotes
Author’s contributions
SM, SM, NY, KH, AT, KI, KT, M-B L, HY, YA, YA and HT designed the study. SM and SM collected the data. SM, SM and NY analyzed the data and developed the methodology. SM was a major contributor in writing the manuscript. SM and SM analyzed and interpreted the patient data. HT oversaw the study. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability statement
All data generated or analyzed during this study are included in this article.
Informed consent
Written consent to publish was obtained from the study participant, and a copy is available to the journal. All the authors read the final manuscript and approved for publication. Participate outcomes were collected independently from the participant with written informed consent.
Ethics approval
This study was approved by Medical Ethics Committee of Kanazawa University.