
Abstract
Introduction:
Fibromatosis is a benign disease yet prone to recurrence. The best treatment option remains controversial. The purpose of this study was to analyse the management approach in our musculoskeletal tumour centre.
Materials and Methods:
Thirty-four patients with extra-abdominal fibromatosis referred to our centre between 2000 to 2018 were included. Patients’ demographics, tumour location and size, year of diagnosis, treatment modalities, surgical margins, recurrence, and subsequent management were analysed.
Results:
Patients mostly presented in the second and third decade, with female predominance. Twenty-seven patients underwent excision. Other management options included ‘watchful waiting’, pharmacological treatment and radiotherapy. Recurrence rate was 51.9%. There was no statistically significant relationship between marginal status and recurrence.
Conclusion:
We report our experiences on management of fibromatosis, with strategy shifted from early excision to a conservative approach over the years. Surgical excision is still indicated in some situations. Tumour recurrence is not rare but second excision is not always necessary.
Introduction
Fibromatosis is a rare benign disease in which monoclonal fibroblastic proliferations occur in deep soft tissues, characterized by infiltrative growth and tendency towards local recurrence after excision. It arises in different anatomical locations, both abdominal and extra-abdominal. The tumour can cause pain, and functional impairment as a result of joint contracture and compression on major neurovascular bundles in limbs. Although it does not metastasize, it can still be fatal if it compresses on adjacent vital structures. Natural history is highly unpredictable. Treatment modalities include ‘watchful waiting’, non-steroidal anti-inflammatory drugs, anti-oestrogen, chemotherapy, targeted therapy, radiotherapy, surgical excision and combination of the above. However, management remains challenging. There is limited number of publications from orthopaedic perspective on this disease in Hong Kong population. This study aims to review the management of extra-abdominal fibromatosis in one of the three musculoskeletal tumour centres in Hong Kong.
Methodology
This is a retrospective study on patients with biopsy proven extra-abdominal fibromatosis from May 2000 to January 2018 managed in Department of Orthopaedics and Traumatology in our hospital. All cases with diagnosis of ‘fibromatosis’ in the database of Department of Pathology in our hospital were retrieved. There were 43 patients. In cases where pathological diagnosis had been made elsewhere, the slides were reviewed by pathologist in our hospital for confirmation of diagnosis. Exclusion criteria were: 1. fibromatosis in the hands and feet, 2. cases with insufficient information, 3. cases with follow-up duration less than 1 year. There were 34 patients included in analysis. Data were obtained through review of medical records. Patients’ demographics, tumour characteristics (size, location, primary or recurrent) and treatment with outcome were evaluated. Tumour size was determined by greatest dimensions in magnetic resonance images (MRI) or excisional specimen. The excisional margins were classified as either microscopically positive (involved) or negative (clear). Local recurrence was diagnosed by MRI with or without biopsy. Follow-up period ranged from 17 to 179 months (median 85 months).
Results
The patients’ age at diagnosis ranged from 6 months to 77 years old. The peak age at presentation was in the second and third decade. Female (23) to male (11) ratio was 2.1:1. Thirteen cases were fibromatosis of upper limbs and 16 were disease of lower limbs. Five patients had fibromatosis from other extra-abdominal locations, such as neck and back. Sizes of tumours ranged from 3.78 to 3139.5 cm3. Patient and tumour characteristics with excision, marginal status and recurrence are shown in Table 1.
Patient and tumour characteristics with excision, marginal status and recurrence.
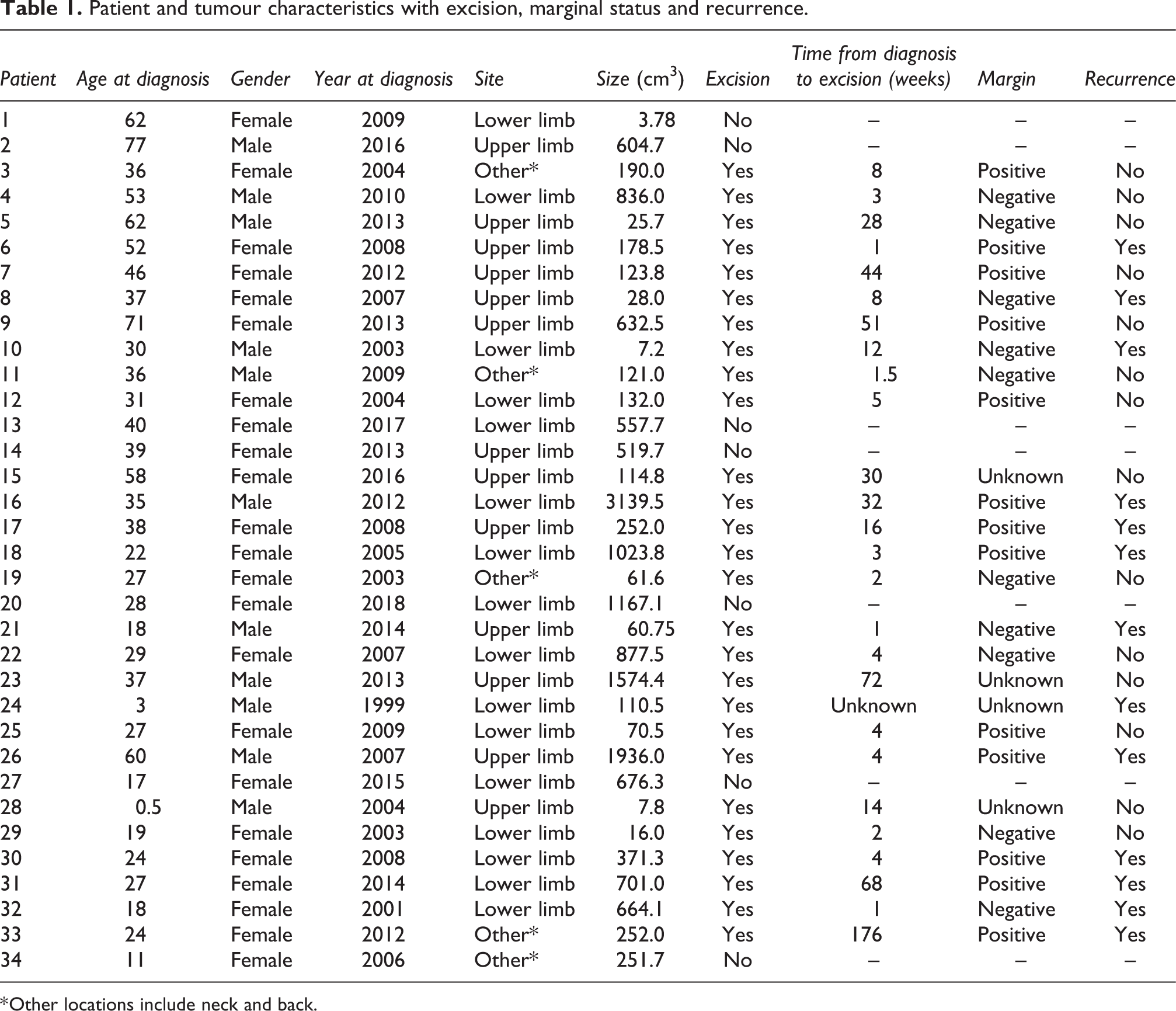
* Other locations include neck and back.
Pharmacological treatment included non-steroidal anti-inflammatory drugs (NSAID), anti-oestrogen (Tamoxifen), targeted therapy (such as imatinib), and chemotherapy. Eighteen patients received NSAID, mainly indomethacin. Seven of them received NSAID for less than 1 year, and 11 received for more than 1 year. Cessation of NSAID was mainly due to gastrointestinal discomfort. No major complication was reported from patients who took NSAID. Eight patients received Tamoxifen, five of them received for less than 1 year and three for more than 1 year. One patient received targeted therapy for 3 months. One patient received chemotherapy for 1 month before surgical excision. No patients received radiotherapy alone or pre-operative radiotherapy. Four patients received post-operative adjuvant radiotherapy. Two patients opted for ‘watchful waiting’ without any pharmacological, surgical treatment or radiotherapy.
Among the 34 patients, 27 of them underwent excision. Before 2011, 18 out of 20 patients underwent excision (90%); while 9 out of 14 patients underwent excision after 2010 (64.3%). Main indication for excision was pain (14). Other indications were: neurovascular compression (7), increasing size of tumour (six), joint contracture (three) and patient’s preference (three). Indication for excision was not documented in four cases. One patient might have more than one indication for excision. Fifteen patients underwent excision within 2 months after diagnosis confirmed: 14 of them were operated in the period of 2001 to 2010, and the remaining one was operated in 2014. The other 12 patients underwent excision 12 to 176 weeks after diagnosis confirmed. Out of these 12 patients, 8 of them received pharmacological treatment prior to excision in the period of 2011 to 2018. These pharmacological treatments were NSAID and/or Tamoxifen. Neo-adjuvant chemotherapy was given in one case. Imatinib was considered in two cases but it was not prescribed due to patients’ financial concern. Out of the 27 patients who underwent excision, 10 had clear margins and 13 had involved margins. In the remaining four cases, marginal status was not mentioned in pathology report.
Fourteen patients had recurrence of tumour as diagnosed by MRI. Biopsy was performed in five cases to confirm diagnosis. Recurrence rate was 51.9%. In cases with clear excisional margins, recurrence occurred in 4 out of 10 cases. In cases with involved excisional margins, recurrence occurred in 8 out of 13 cases. Fisher’s exact test showed no statistically significant relationship between marginal status and recurrence (p = 0.41). Time from excision to recurrence ranged from 3 to 37 months. Again, Fisher’s exact test showed no statistically significant relationship between marginal status and time from excision to recurrence (p = 0.58, Table 2). Further management included ‘watchful waiting’ (five), pharmacological treatment alone (three), re-excision alone (three) and combination of pharmacological treatment, radiotherapy and re-excision (three). Less than half (42.9%) of patients with recurrent tumour underwent excision again. For all patients who had undergone excision, 22.2% of them underwent second excision. Table 3 showed the relationship between patient demographics and marginal status versus recurrence.
Relationship between marginal status and time from excision to recurrence.
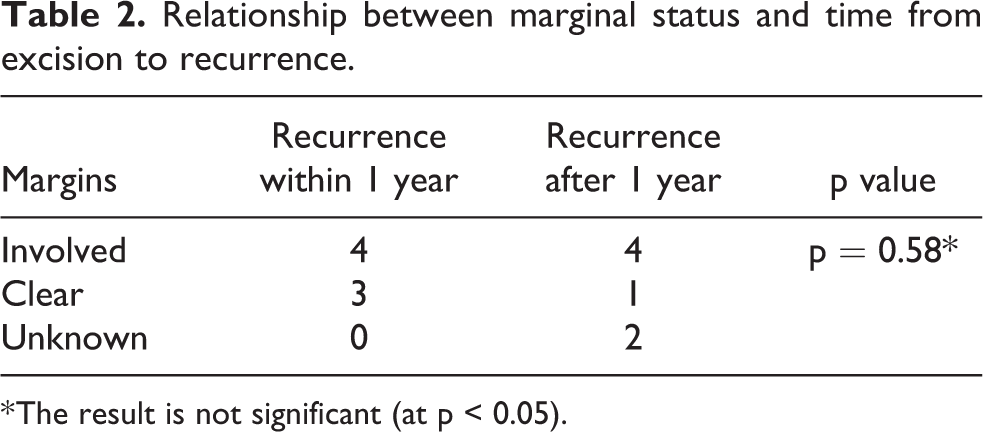
* The result is not significant (at p < 0.05).
Patient demographics and marginal status versus recurrence.
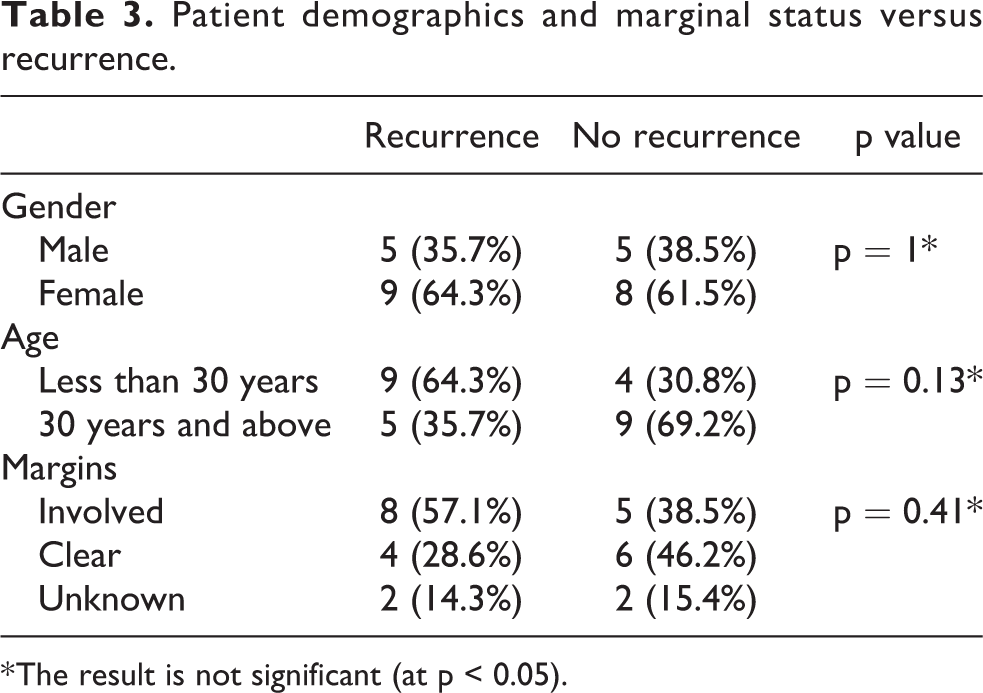
* The result is not significant (at p < 0.05).
The following four cases illustrate the management strategy of fibromatosis in our centre over the years:
Case 1
A 27 year old lady was referred to our clinic in November 2017 for incidental finding of right buttock mass in CT abdomen and pelvis. She reported buttocks asymmetry for years but was not aware of presence of mass. She complained of right buttock pain for 2 years. She was able to walk unaided. Physical examination revealed a right buttock mass with limitation in right hip external rotation to 20°. MRI showed a mass infiltrating tensor fascia lata with extension to gluteal muscles (Figure 1a). Diagnosis of fibromatosis was confirmed by needle biopsy.
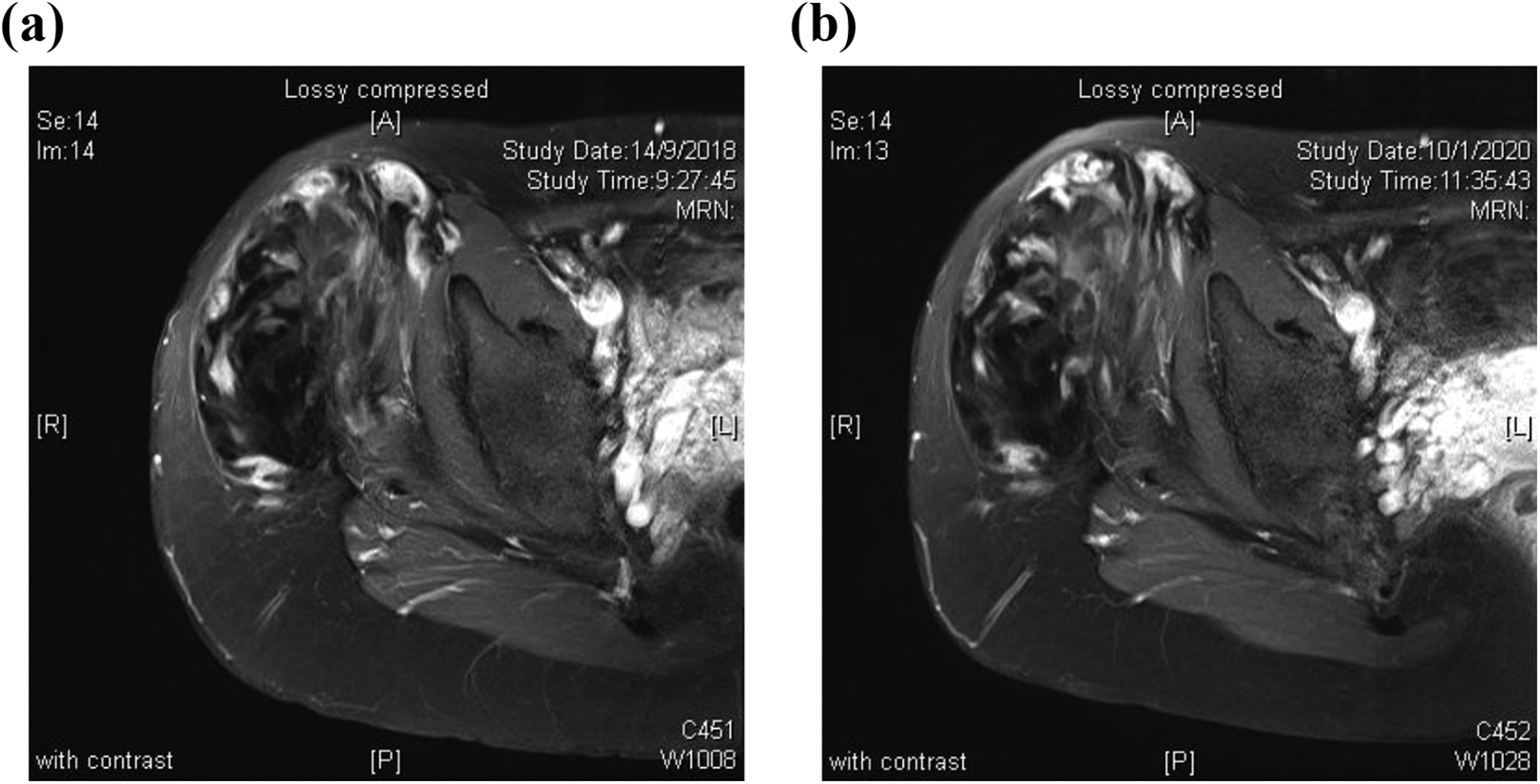
(a) and (b) Contrast-enhanced T1 weighted (fat suppressed) MRI taken in 2018 and 2020 respectively, showing similar characteristics of the fibromatosis.
During follow-up, she reported similar pain and size of mass. After discussion on pharmacological treatment, she opted for trial of NSAID, but not Tamoxifen. However, NSAID was stopped later due to intolerance of side effects, pregnancy and breastfeeding. There was no progression in tumour size or pain, with latest MRI in January 2020 (Figure 1b) showing no significant change in size and appearance of mass.
This case illustrates successful conservative management of fibromatosis. Patient lives with disease with tolerable symptoms.
Case 2
A 37-year-old lady presented with left posterior upper arm painful swelling for 1 year in September 2007. MRI showed a 3.4 × 3 × 5 cm infiltrative mass involving triceps and deltoid, suggestive of fibromatosis (Figure 2). Diagnosis was confirmed by needle biopsy. Excision was performed in January 2008. Pathology showed clear excisional margins. There was minimal pain after surgery. She was referred for physical therapy but weakness of triceps persisted.
Contrast-enhanced T1 weighted (fat suppressed) MRI of in October 2007 prior to excision, showing fibromatosis infiltrating triceps and deltoid.
She complained of increasing pain in mid-2009. MRI showed four small lesions close to previous deep operative field, suspicious of tumour recurrences. Options of radiotherapy and various pharmacological treatments were discussed. She received NSAID since August 2009, but stopped taking it due to epigastric discomfort 11 months later. She was then diagnosed to have gastritis by oesophageogastro-duodenoscopy.
Follow-up MRI in February 2011 showed enlarging masses over posterior upper arm and another nodule at lateral mid-arm. Symptoms were mild and the masses were not palpable, hence excision was not considered at that juncture. She opted to commence NSAID again.
She reported increase in pain in 2012. Options of Tamoxifen and radiotherapy were discussed again. She decided to try Tamoxifen in June 2012. Pain was increasing and serial MRI up till 2014 showed increasing size of tumours. She reported inconsistent use of Tamoxifen.
Throughout the years since then, she reported fluctuating pain and subjective size of masses. Follow-up MRI showed increase in size of tumours. She decided to stop NSAID and Tamoxifen in March 2016, and to continue with observation and follow-up MRI. Pain was similar. The most recent MRI in August 2018 showed static size of tumours.
This case illustrates the management strategy before 2011
Indications of excision were liberal, without pre-operative trial use of pharmacological treatment. Wide margin excision was planned if possible, which would inevitably lead to greater functional morbidities and cosmetic consequence. Despite clear margin excision was achieved, recurrence occurred. Fortunately symptoms from recurrent tumours were tolerable. They did increase in size but not to the degree of causing functional impairment. The patient could live with the recurrent tumours for long time without surgical intervention. Pharmacological treatment, be it NSAID or Tamoxifen, produced intolerable side effects and hence long-term compliance was poor. Radiotherapy was not delivered due to its potential side effects and complications.
Case 3
A 27-year-old lady presented in December 2014 with right thigh swelling for 6 months. Physical examination showed a 10 × 15 cm mass over the posterior thigh, with diminished light touch sensation on sole. MRI showed a heterogeneous contrast-enhancing mass involving right biceps femoris, abutting on sciatic nerve. Needle biopsy showed spindle cell lesion consistent with fibromatosis. She was initially given NSAID but the side effect of epigastric pain could not be tolerated. She was then given Tamoxifen. She reported decrease in pain, numbness and swelling. MRI the next year showed no increase in size of tumour (Figure 3).
Contrast-enhanced T1 weighted (fat suppressed) MRI in October 2015 prior to excision. This image illustrates the fibromatosis involving posterior compartment of thigh, closely abutting on femur, lying deep to sciatic nerve.
However, in January 2016 she complained of worsening pain and numbness affecting her daily activities such as sitting and hence she requested strongly for excision. At that time her straight leg raise was 60° with positive Lasegue test. In view of close proximity of the tumour to sciatic nerve, it was anticipated that excisional margins would be involved. In Combined Sarcoma Clinic (a conjoint clinic with Clinical Oncologist), patient accepted use of imatinib to maximize pharmacological control prior to surgery. However, it was stopped few months later due to nausea, while pain and numbness persisted. She was not keen for chemotherapy. Tamoxifen was also stopped due to per vaginal spotting.
Marginal excision was performed in March 2016. Pathology showed fibromatosis with involved excisional margins (Figure 4b). Post-operative radiotherapy was considered in Combined Sarcoma Clinic but it was withheld due to the risks to pelvic viscera. She reported much decrease in pain and absence of numbness on sole. Straight leg raise was full. Follow-up MRI in January 2019 showed suspicious tumour recurrence (Figure 5). Patient opted to resume use of Tamoxifen. When she was last seen in March 2020, she had only occasional mild pain but no distal numbness. There was neither palpable mass nor distal neurological deficit. The last MRI in February 2020 showed no interval change as compared to previous scan.
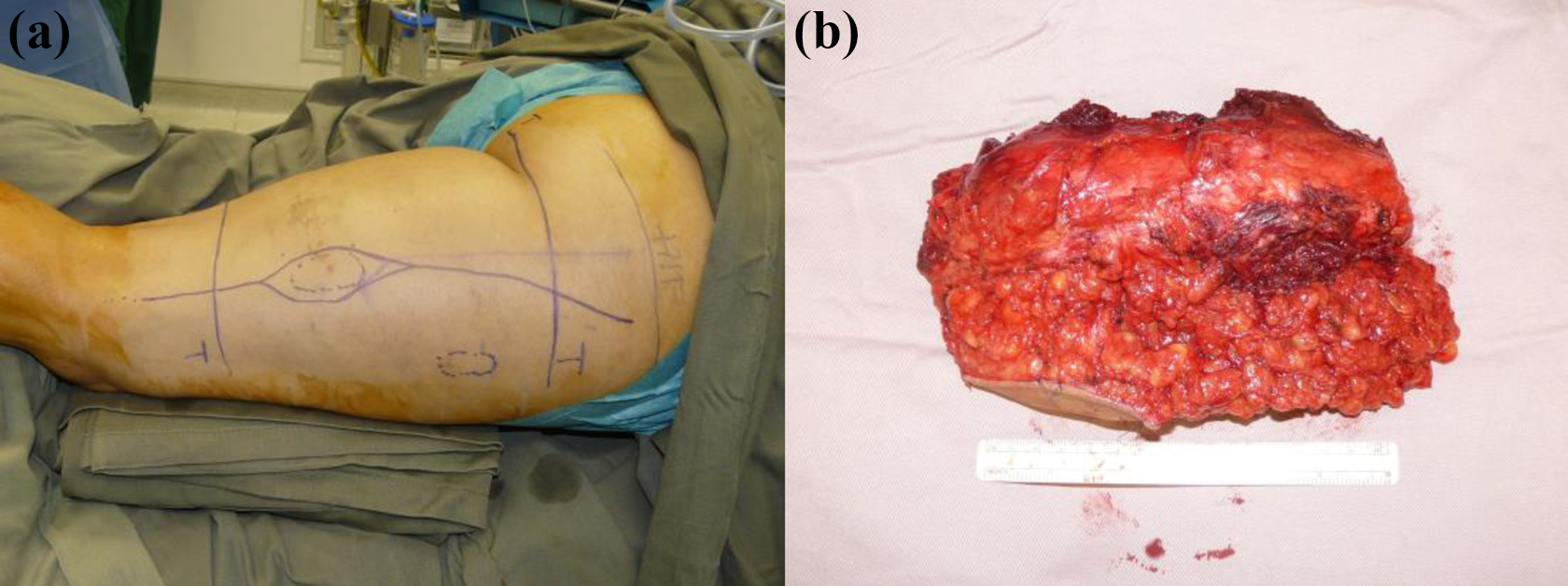
(a) and (b) Pre-operative incision planning and excised fibromatosis specimen.
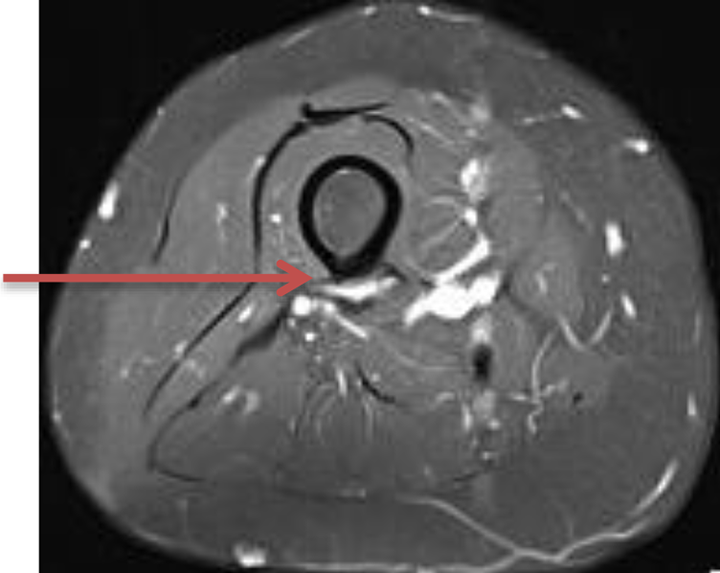
Contrast-enhanced T1 weighted (fat suppressed) MRI in January 2019 showing suspected tumour recurrence (arrow) along posterior femur and intermuscular plane between vastus intermedius and long head of biceps femoris.
This case illustrates the management strategy after 2010
‘Watching waiting’ with pharmacological treatment was suggested as initial management. In some patients the tumour did not progress over years. In some patients, such as this lady, the side effects of pharmacological treatment were not tolerated. The tumour progressed and produced neurological compression, which was a strong indication for excision. After excision, relief of symptoms was dramatic. Tumour recurrence was not surprising, as excisional margin involvement was anticipated. Many a times the recurrence did not progress as fast as the tumour did before excision and hence further excision was not needed. Radiotherapy was to be avoided as far as possible. The recurrence was observed under monitoring by serial MRI, with or without pharmacological treatment.
Case 4
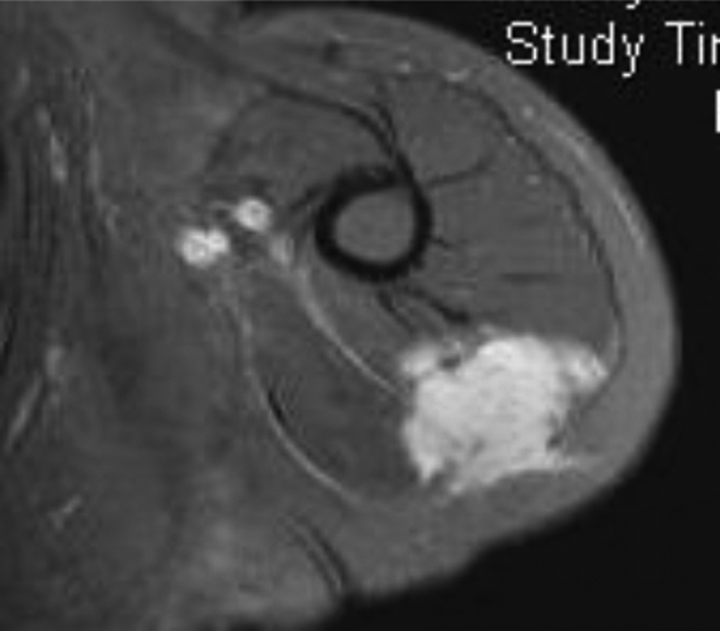
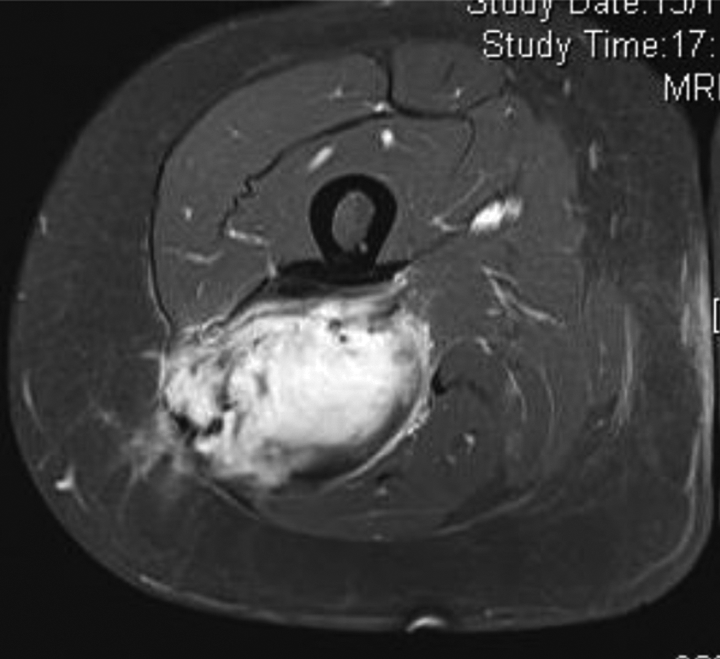
A 35-year-old gentleman presented with a left popliteal mass in February 2012. MRI showed a 6.2 × 4.5 × 8.5 cm tumour involving proximal gastrocnemius and soleus with encasement of popliteal neurovascular bundle. He complained of occasional numbness on sole but there was no distal neurological deficit. Dorsalis pedis pulse was palpable, although weaker than contralateral one. The range of movement of knee was only 10° to 110°. Needle biopsy confirmed the diagnosis of fibromatosis. He was started on NSAID in March 2012.
There was increasing flexion contracture of knee and calf discomfort on walking upon follow-up visits. He agreed to try Tamoxifen in July 2012. Despite the combined use of Tamoxifen and NSAID, numbness and weakness were increasing, while flexion contracture of knee and plantarflexion contracture of ankle were progressing. Serial follow-up MRI showed increasing size of tumour. The major neurovascular bundles were encased to the degree that they were not clearly delineated in MRI (Figures 6a and 6b). He was seen in Combined Sarcoma Clinic at the end of 2013. Use of imatinib was suggested but he was unable to afford financially. The size of tumour increased more rapidly in 2014 and his left dorsalis pedis pulse was no longer palpable. Tamoxifen was stopped due to palpitation. In view of progression of disease with severe symptoms and functional impairment despite pharmacological treatment, he accepted the plan of neo-adjuvant chemotherapy followed by surgical excision and post-operative radiotherapy. Second needle biopsy was performed to confirm diagnosis again prior to commencement of chemotherapy. CT-angiogram was performed for pre-operative planning of excision. The tumour was successfully excised in October 2014 with multiple margins involvement (Figure 7). Post-operatively he reported decrease in pain, numbness with improved power, knee and ankle contractures. Radiotherapy was completed in March 2015. First post-operative MRI in January 2016 showed no evidence of tumour recurrence.
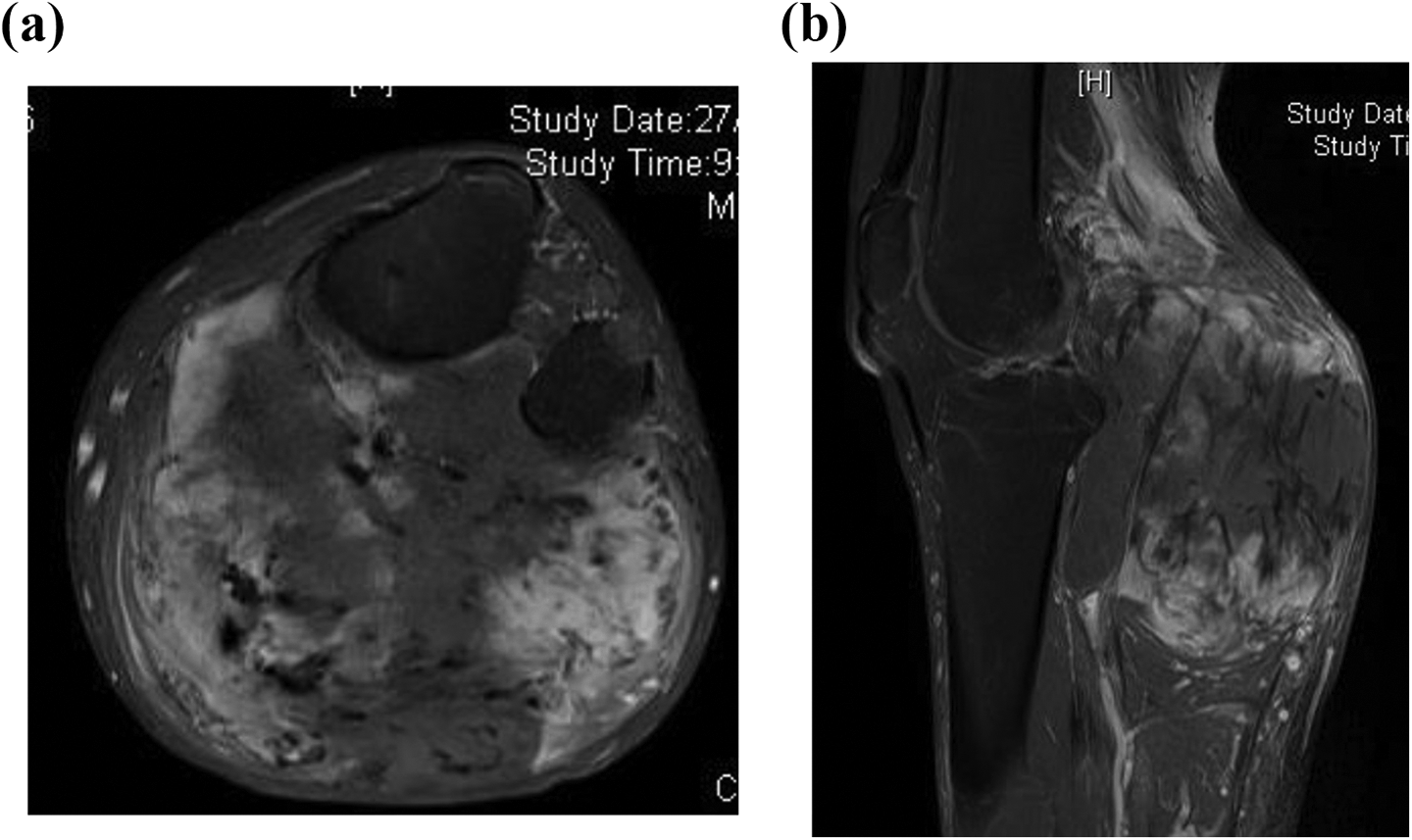
(a) and (b) Contrast-enhanced T1 weighted (fat suppressed) MRI in January 2014 prior to first excision. These images illustrate the large fibromatosis involving the gastrocnemius and soleus muscle, encasing the popliteal vessels and tibial nerve.

Specimen of excised fibromatosis.
However, second post-operative MRI in May 2017 showed mass lesion at distal biceps femoris, a location proximal to the excised fibromatosis but within previous operative and irradiated field. The mass was proven to be fibromatosis by needle biopsy. MRI in January 2018 showed increase in size of tumour. Patient requested for excision without trial use of pharmacological treatment basing on his previous experiences. Radiotherapy was not planned since the tumour was within previously irradiated field. Second excision was performed in February 2018.
Follow-up MRI in September 2018 showed recurrent tumour at distal biceps femoris, and new tumours in calf muscles, all within previous operative and irradiated field. The tumours increased in size with pain. He requested for excision of thigh tumour and one of the larger calf tumours. Surgery was performed in January 2019.
He noted recurrence of left thigh mass again in August 2019. MRI in November 2019 showed tumour in left upper thigh and lower calf. The thigh tumour was more proximal than the previous one, partially encasing the sciatic nerve. In Combined Sarcoma Clinic, he was advised to try imatinib. It was started in December 2019. However, MRI in February 2020 showed increase in size of thigh tumour (Figure 8) despite use of imatinib and hence the drug was stopped. Patient requested strongly for excision again as the tumours increased in size with much pain. It was explained that the thigh tumour might only be debulked as it encased sciatic nerve. Further recurrence would be highly likely. Post-operative radiotherapy might be considered but the irradiation field would overlap with previous one, and hence ulcers might be resulted. He was also informed that if ulcers could not heal, or tumour recurred at a more proximal location, amputation might become necessary. At the time of writing of this report, surgery has not yet been performed.
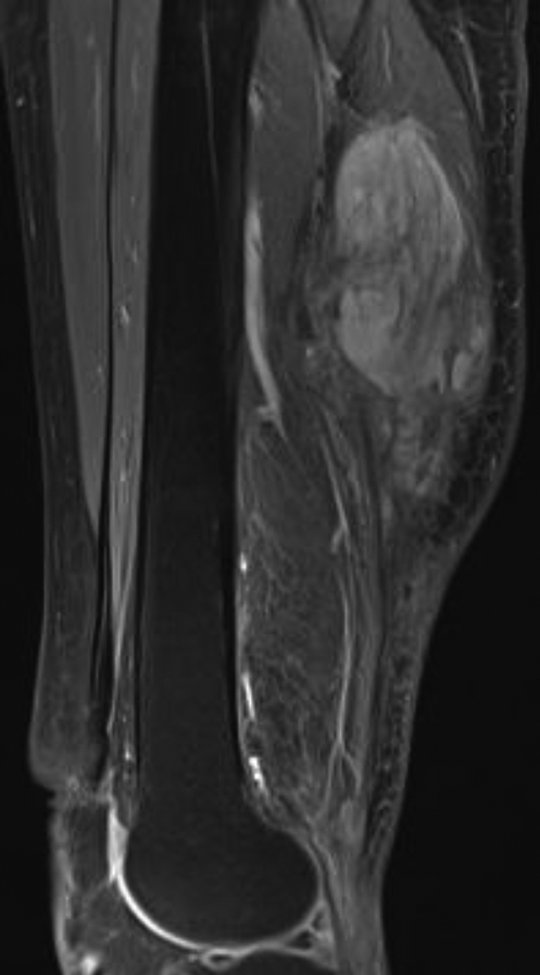
Latest contrast-enhanced T1 weighted (fat suppressed) MRI in February 2020, showing recurrence of fibromatosis in left thigh on proximal side of previous surgical field. Sciatic nerve is partially encased by tumour.
This case illustrates how difficult the management of fibromatosis can be. Patient was an active young adult. The tumour progressed fast despite pharmacological treatment, producing disabling symptoms and functional impairment. Surgical excision was the only option to relieve neurovascular compression, although margins involvement and recurrence had already been anticipated. Neo-adjuvant chemotherapy and adjuvant radiotherapy did not alter the disease course significantly. The tumour neither responded to targeted therapy. Repeated recurrences at proximal side of surgical and irradiated field were most worrying, and amputation might be the last resort to prevent recurrence of disease.
Discussion
Fibromatosis is a disease notoriously difficult to manage. Traditional mainstay of treatment was wide excision. As the tumour infiltrates into surrounding tissues, it is often difficult, if not impossible to excise with clear margins. Wide excision may result in great functional disturbances and poor cosmesis. Yet recurrence still occurs and it has been controversial whether wide excision reduces recurrence rate. 1 This disease occurs more frequently in young female and it has been postulated that pathogenesis is related to hormonal imbalance. 2 This explains why wide excision may not prevent recurrence. Various modalities of treatment including NSAID, anti-oestrogen, chemotherapy, 3 radiotherapy 4 and recently targeted therapy have been used for disease control. However, results with single or combined use of them varied widely as reported in literature. 5 –9 In our study, common reasons for cessation of pharmacological treatment were intolerance of side effects and tumour progression. The treatment modalities for malignancy are usually reserved for recurrent or inoperable cases due to their toxic side effects.
Knowing that surgical outcome not always satisfactory, there has been a trend towards conservative excision and even conservative management of disease. A management algorithm starting with ‘wait-and-see’ policy with concomitant pharmacological treatment was proposed and high control rate was reported. 10,11 Some recommended ‘wait-and-see’ regardless of symptoms for the first 1 to 2 years, with monitoring of disease by serial contrast MRI. 10 Spontaneous regression of fibromatosis was seen in 20–30% of patients in some reports. 12 In our centre prior to 2011, surgical excision was the mainstay of treatment and it was performed soon after diagnosis confirmed. This can be reflected from the fact that 90% of patients underwent excision before 2011. This percentage dropped to 64% after 2010. Moreover, for excisions performed within 2 months from diagnosis, 14 out of 15 cases were in the period of 2001 to 2010 (Case 2). The other 12 excisions were performed from 12 to 176 weeks after diagnosis confirmed. Out of these 12 patients, 8 of them received pharmacological treatment prior to excision in the period of 2011 to 2018. Although some tumours did respond to this management strategy as illustrated by Case 1, some progressed as illustrated by Case 3 and 4. Among the 27 patients who underwent excision, commonest indication for surgery was pain (14). Other indications included: neurovascular compression (seven), increasing size of tumour (six), joint contracture (three) and patient’s preference (three). There was no documented indication for excision in four patients. When tumour abutted on major neurovascular bundles, compression of these structures produced disturbing symptoms and functional impairment. Under this situation, surgical excision was the only effective option to relieve compression. Margin involvement and recurrence had been anticipated. The other important change in management was the adoption of a function-preserving excision i.e. preservation of function took higher priority than achievement of clear margins in excision.
Figure 9 shows our management algorithm of fibromatosis after 2010.
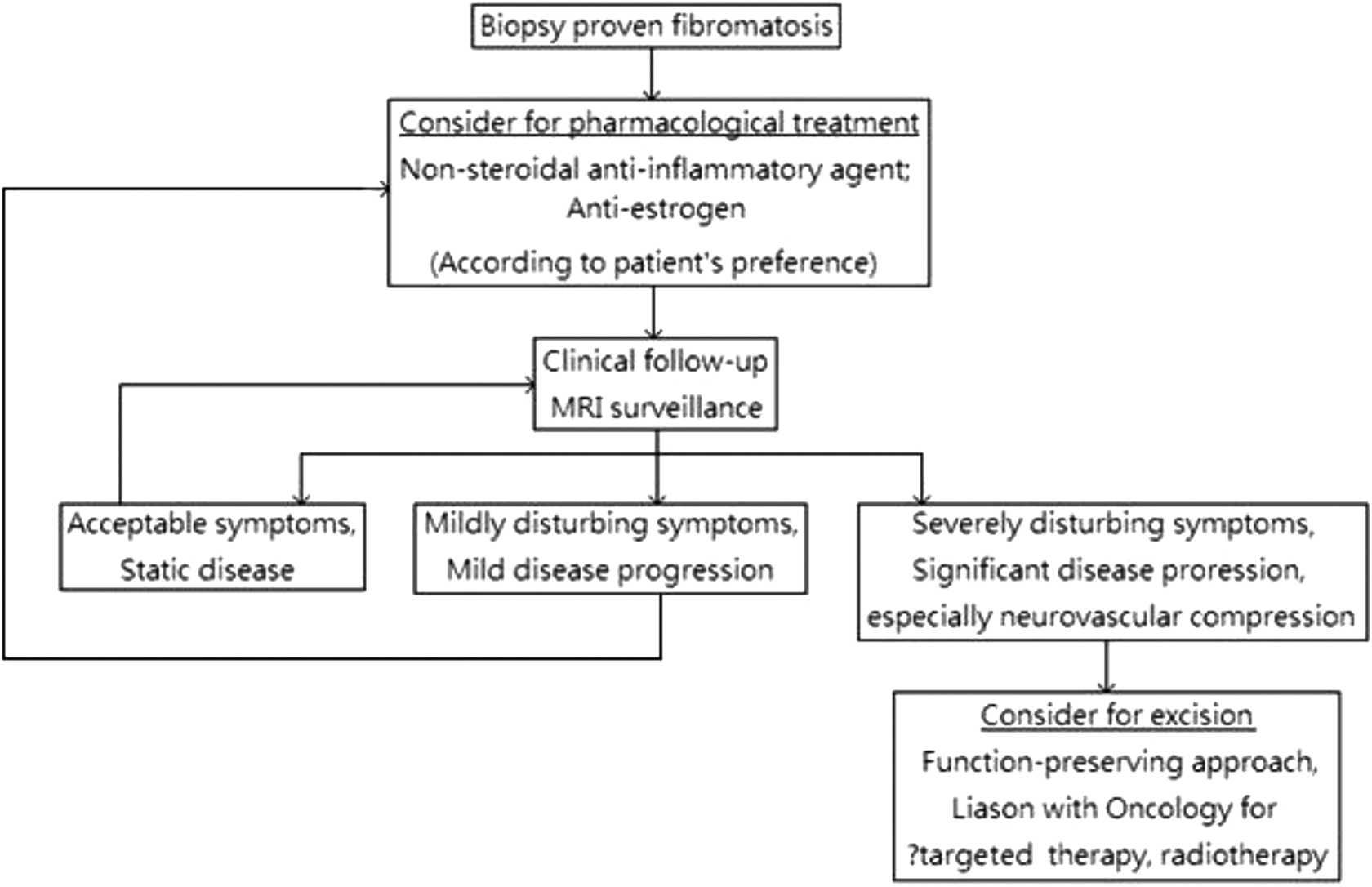
Fibromatosis management algorithm after 2010.
This study also confirms female predominance and they often present during the second and third decade of life. Recurrence rate in this study of 51.9% is comparable to literature. Recurrence rate ranges from 23 to 77% in some studies. 13 –16 Statistical analysis shows that recurrence is not related to marginal status, coinciding with some reports. 13 –16 Fortunately recurrent tumour may not progress as fast as the primary one. It may not produce symptom and the patient may live with the tumour for a long period of time. Only less than half (42.9%) of patients with recurrent tumour underwent excision again. For patients who had undergone excision, only 22.2% of them underwent second excision. There is also no statistical relationship between marginal status and time from excision to recurrence.
Limitations of this study include the retrospective nature of study, small number of cases and lack of microscopic marginal width measurement. In a small proportion of cases, tumour had already been excised prior to referral to our centre.
Conclusion
Management of fibromatosis remains controversial and challenging. We report our experiences on management of this disease with shift of strategy from early aggressive excision to a conservative approach starting with ‘watchful waiting’ with or without concomitant pharmacological treatment. Moreover, preservation of function now takes higher priority than achievement of clear margins in excision. Under certain situations, for example, when there is neurovascular compression, surgical excision still plays a role. This shift has been successful as reflected by a significant drop in excision rate and low re-excision rate. Disease control is generally satisfactory as far as symptoms are concerned.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.