
Abstract
Keywords
Introduction
Total joint arthroplasty is one of the most important surgical operations in the 21st century, it is widely used in advanced arthritis. Periprosthetic joint infection is one of the most severe complications that occur in patients who undergo total joint arthroplasty. At present, the two-stage revision is the main way to treat the periprosthetic joint infection following total joint arthroplasty, but there is still a risk of failure after the two-stage revision, reinfection rates reported in the literature range from 4 to 50%.1–4
More than 500 million people are obese worldwide, including one-third of men and women in the United States.5,6 Obesity increases the risk of osteoarthritis, and it is a key component in the sustained rise in the number of patients undergoing TJA. Obesity (BMI [body mass index], ≥ 30 kg/m2) is a well-established risk factor for PJI.7–11 However, the role of obesity or BMI in two-stage revision failure of PJI following TJA is unclear.
The correlation between BMI and two-stage revision failure of PJI following TJA have been reported by many lately, but the results of studies are divergent and even controversial. In this study, we retrieved the published literature on two-stage revision failure of PJI following TJA, extracted high-relevant data for a systematic review and meta-analysis, and evaluated the correlation between BMI and two-stage revision failure of PJI following TJA, in a bid to provide a reference for the prevention of two-stage revision failure of PJI.
Methods
Search strategies
The Pubmed database literature search strategy.

Study selection criteria
Two independent investigators analyzed the initially selected articles to verify their relevance with the topic of the correlation between BMI and two-stage revision failure of PJI following TJA. Studies had to fulfill the following criteria for inclusion: outcome was two-stage revision failure of PJI following TJA; study design included case-control, retrospective and prospective cohorts, and cross-sectional studies; participants were selected without limitations to regions, ages, or social status. Trials were excluded according to following identifications: duplicate or overlapping data, animal experiments, conference abstracts, letters, and review articles. In case of any disagreement the results were discussed and unified by senior authors.
Data extraction
Data from the included studies were extracted and independently categorized by two of the authors in a predefined data extraction form. All disagreements were resolved by discussion. Design information, baseline population characteristics (mean age, sample size, and country), surgical approach, risk factors from all included studies were stratified into a standardized evidence table. All the data were rechecked to ensure accuracy. Study selections were shown in a PRISMA flow diagram.
Methodological quality assessment
The methodological quality of the included studies was evaluated by two independent reviewers based on the items of modified Newcastle-Ottawa Scale (NOS), 14 comprising patient selection, study group comparability, and outcome assessment. The observational studies scored 0 to 9. Divaricate opinions were discussed among the authors.
Statistical analysis
The meta-analysis and statistical analysis were performed using Stata 13.0 software (Stata Corp, USA) and Cochrane Collaboration Review Manager software (RevMan version 5.3, Nordic Cochrane center, Copenhagen, Denmark). The OR and 95% CIs were calculated. The I-square (I2) test was adopted to evaluate the influence of heterogeneity on the output of the meta-analysis. I2 values of 0%, 25%, 50%, and 75% represented no, low, medium, and high heterogeneity, respectively. Heterogeneity was tested using Cochran’s Q statistic and the I2 metric: a I2 > 25% was the cutoff of significant heterogeneity, and a fixed-effect model was used when a I2 < 25%; otherwise, a random effect model was preferred. 15 A p value of less than 0.05 was accepted as statistically significant. A sensitivity analysis 16 was conducted by excluding one study at a time to evaluate the quality and consistency of the results. Egger’s and Begg’s linear regression tests for publication bias were carried out. Subgroup analyses were performed according to different countries, operation methods, and effect type.
Results
Study selection process
As a result, 1231 references were initially retrieved, 539 were left after eliminating duplicate literature; and then 499 without high-relevant to our topic were discarded by reading titles and abstracts, and 40 studies remained. Finally, 25 full-text articles were abandoned because of the following reasons: 15 studies on irrelevant topics; five studies without full-text materials; three studies without sufficient data for extraction; one study was poster abstracts; one study was letters to the editor. Therefore, 15 observational studies with 1267 patients were included, of which 15 studies were included in systematic review and 11 studies in meta-analysis. The flow chart describing the selection process of the study was shown in Figure 1. The flow diagram of literature search and selection.
Study characteristics and methodological quality
Characteristics of the included studies.
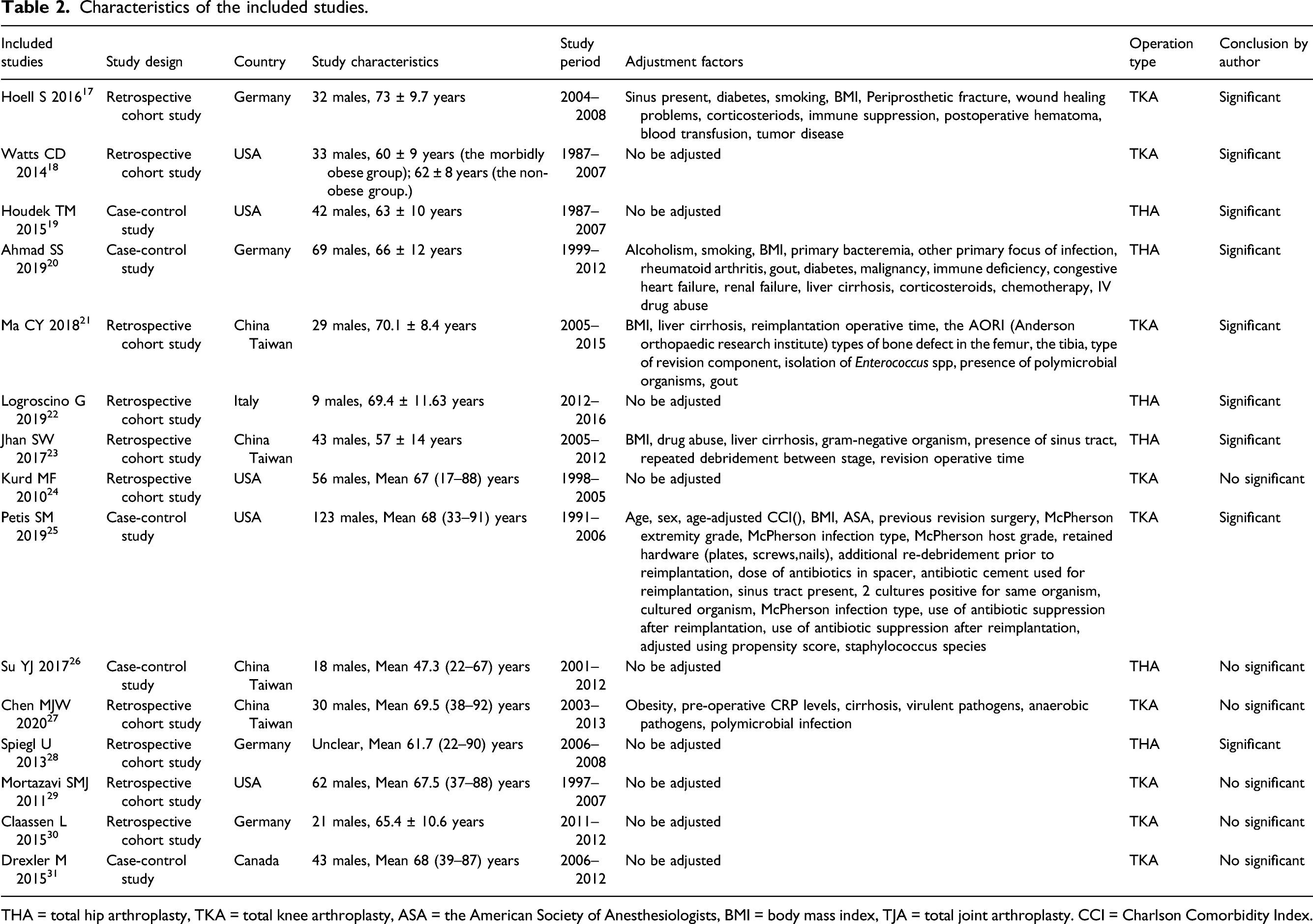
THA = total hip arthroplasty, TKA = total knee arthroplasty, ASA = the American Society of Anesthesiologists, BMI = body mass index, TJA = total joint arthroplasty. CCI = Charlson Comorbidity Index.
Characteristics of the included studies.

Overall meta-analysis
BMI ≥ 30 kg/m2 vs. BMI < 30 kg/m2
Data from six studies17,20,21,23,25,27 on BMI ≥ 30 kg/m2 vs. BMI < 30 kg/m2 were available for the meta-analysis by the random effect model due to a significant statistical heterogeneity (I
2
= 83.4%, p = 0.000). It was found that the risk of two-stage revision failure of PJI following TJA significantly boosted by 3.53 times in patients with BMI ≥ 30 kg/m2 (OR = 3.53; 95% CI = 1.63–7.64), with high heterogeneity (I
2
= 83.4%, p = 0.000; Figure 2). Thus, subgroup analyses were conducted to investigate the potential factors that could substantially affect the between-study heterogeneity. The meta-analysis of the correlation between BMI (BMI ≥30 kg/m2 vs. BMI <30 kg/m2) and two-stage revision failure of PJI following TJA.
BMI ≥ 40 kg/m2 vs. BMI < 30 kg/m2
Data from two studies18,19 on BMI ≥ 40 kg/m2 vs. BMI < 30 kg/m2 were available for the meta-analysis by the random effect model due to a significant statistical heterogeneity (I2 = 71.3%, p = 0.062). It was found that the risk of two-stage revision failure of PJI following TJA significantly increased by 2.92 times in patients with BMI ≥ 40 kg/m2 (OR = 2.92; 95%CI = 1.06–8.03; Figure 3). The meta-analysis of the correlation between BMI (BMI ≥40 kg/m2 vs. BMI <30 kg/m2) and two-stage revision failure of PJI following TJA.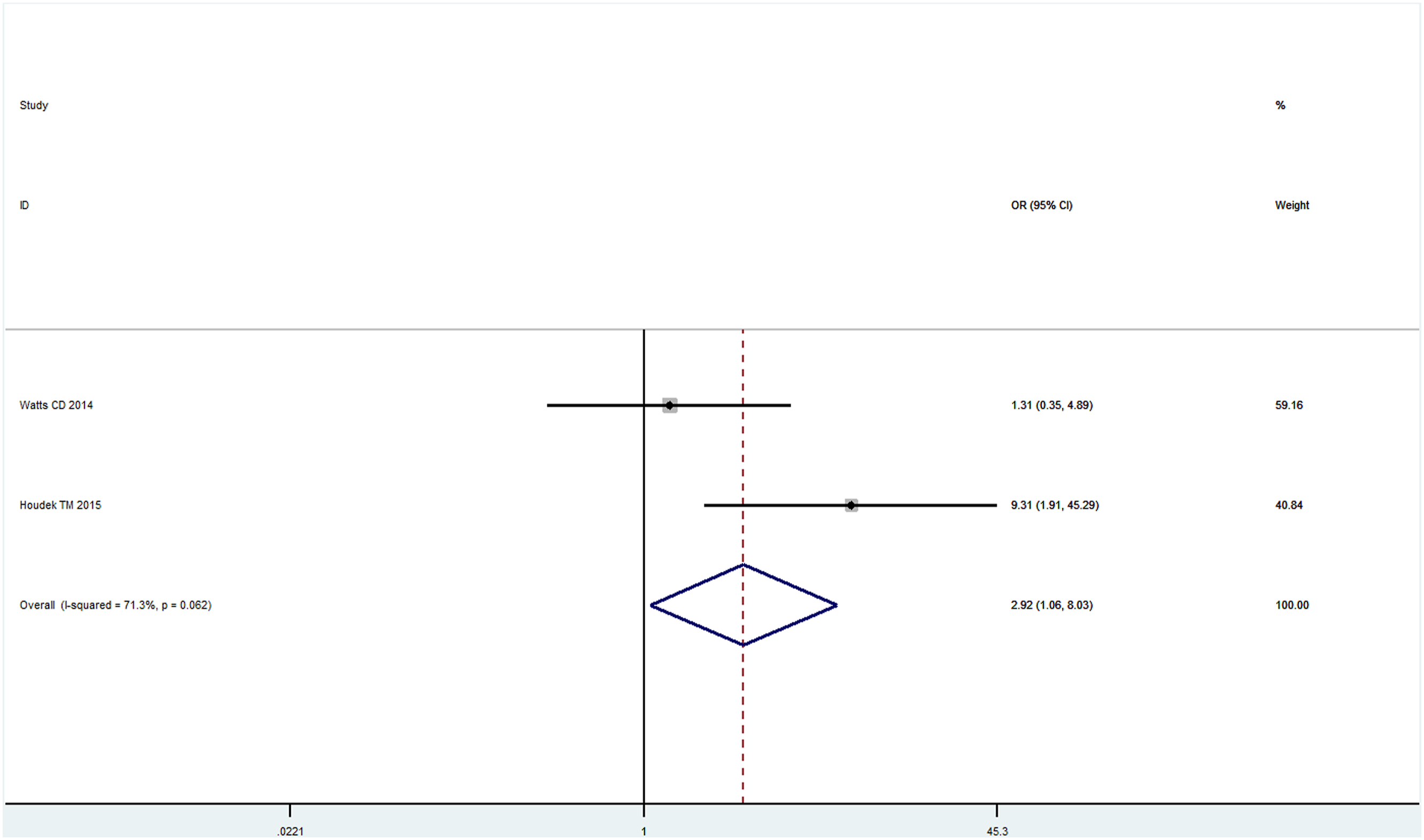
Other body mass index comparisons
Data from three studies22,24,28 on BMI (continuous variable) were available for the meta-analysis by the random effect model due to a significant statistical heterogeneity (I2 = 56%, p = 0.10). The results show that there were nonsignificant differences in BMI between the failure group and the success group (SMD = −0.48; 95%CI = −1.20–0.23; Figure 4). The meta-analysis of the correlation between BMI (continuous variable) and two-stage revision failure of PJI following TJA.
Subgroup analyses (BMI ≥ 30 kg/m2 vs. BMI < 30 kg/m2)
Subgroup analysis of different effect type
Subgroup analyses of different effect type were conducted. The subgroup analysis showed that significant correlations were basically consistent, significant association were observed among the studies performed in odds ratio (OR = 1.22; 95% CI = 1.07–1.40) and hazard ratio (OR = 4.10; 95% CI = 2.64–6.36). When original studies used hazard ratio as the effect type, there was no heterogeneity (I2 = 0.00%, p = 0.467; Figure 5). Subgroup analysis of different effect type.
Subgroup analysis of different countries
Subgroup analyses of different countries were conducted. The subgroup analysis showed that significant association were observed among the studies performed in China, Taiwan (OR = 5.41; 95% CI = 2.51–11.68) and USA (OR = 3.10; 95% CI = 1.61–5.95), but not among those conducted in Germany (OR = 2.191; 95% CI = 0.57–8.44). And the heterogeneity was low when studies performed in China, Taiwan (I2 = 12.3%, p = 0.320; Figure 6). Subgroup analysis of different countries.
Subgroup analysis of different operation method
Subgroup analyses of different operation method were conducted. The subgroup analysis showed that significant association were observed among the studies performed in TKA (OR = 3.63; 95% CI = 2.27–5.82), but not among those conducted in THA (OR = 3.06; 95% CI = 0.42–22.19). And the heterogeneity was no when studies performed in TKA (I2 = 0.0%, p = 0.653; Figure 7). Subgroup analysis of different operation method.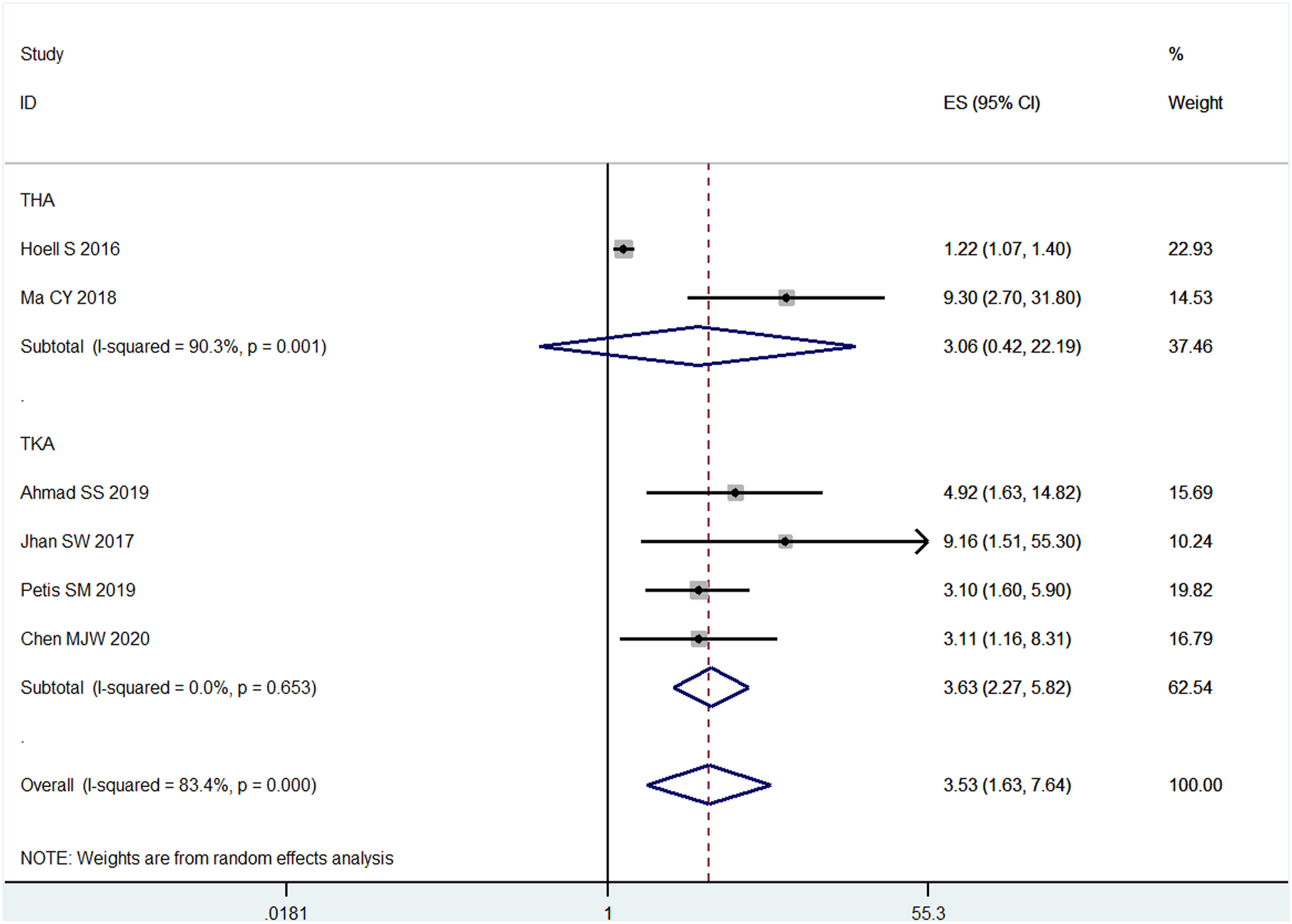
Sensitivity analyses (BMI ≥ 30 kg/m2 vs. BMI < 30 kg/m2)
The sensitivity analysis was performed to assess whether individual studies would affect the overall results. We evaluated the effect of each study on the methodological quality through the sequential exclusion of single studies. The results showed that there was a nonsignificant difference in the stability of the results (Figure 8), which validated the rationality and reliability of our analysis. The influence analysis of included studies.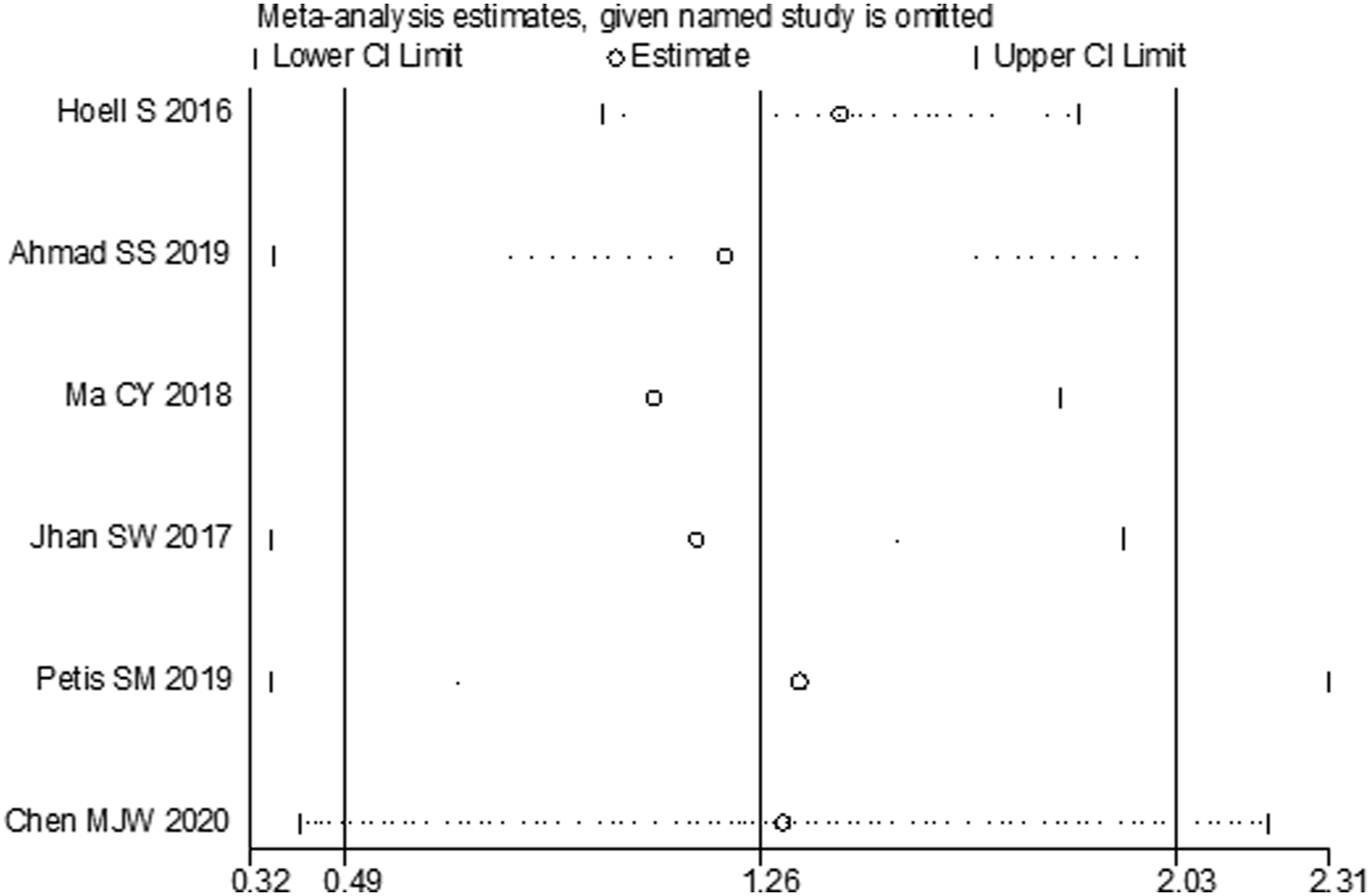
Evaluation of publication bias
Due to the insufficient number of included studies in the meta-analysis, evaluation of publication bias was not conducted (Including visual inspection of funnel plots, Egger and Begg tests).
Discussion
In this study, we conducted 15 observational studies which included 1267 patients, of which 15 studies were included in systematic review and 11 studies in meta-analysis. To ensure a reliable conclusion, previous published studies on the correlation between BMI and two-stage revision failure of PJI following TJA were retrieved, reviewed, and summarized to achieve those with high compliance and high quality, so as to answer various clinical questions of this malady. Our study shows that eight original studies found a correlation between BMI and two-stage revision failure of PJI following TJA, but seven other original studies found no correlation. The failure rate of two-stage revision ranged from 6.8% to 42.86%. And the meta-analysis results suggest that the risk of two-stage revision failure of PJI following TJA significantly boosted in obese patients. The subgroup analysis showed that significant association were observed among the studies performed in TKA (OR = 3.63; 95% CI = 2.27–5.82), but not among those conducted in THA (OR = 3.06; 95% CI = 0.42–22.19). A significant association remained consistent, as indicated by sensitivity analyses.
The two-stage revision is the gold standard for the treatment of periprosthetic joint infection following total joint arthroplasty, but there was still a 6.8%–42.86% failure rate. Previous meta-analysis32–34 showed that obesity was closely related to periprosthetic joint infection following total joint arthroplasty, however, the association between BMI and two-stage revision failure of PJI following TJA remains unclear. Though the correlation between BMI and two-stage revision failure of PJI following TJA has been rapidly reported, their results still remain divergent and even controversial.17–31 Our meta-analysis found that the risk of two-stage revision failure of PJI following TJA significantly boosted by 3.53 times in patients with BMI ≥ 30 kg/m2 (BMI ≥ 30 kg/m2 vs. BMI < 30 kg/m2) and 2.92 times in patients with BMI ≥ 40 kg/m2 (BMI ≥ 40 kg/m2 vs. BMI < 30 kg/m2), this shows a significant increase in the failure rate of two-stage revision in obese patients. When subgroup analysis was performed in different surgical methods, in the THA group, there was no statistically significant difference in failure rates between obese and non-obese patients, this may attribute to the insufficient inclusion of eligible studies. Systematic review found that nearly half of the original studies concluded that BMI was not associated with two-stage revision failure, therefore, we cannot yet conclude that BMI is associated with two-stage revision failure of PJI following TJA.
As the passages have exposed, two significant advantages of our study are clear. Firstly, as the correlation between BMI and two-stage revision failure of PJI following TJA were controversial, this meta-analysis assessed the potential correlation between BMI and two-stage revision failure of PJI following TJA through a thorough systematic study with rigorous analytical methods. Secondly, the rationality and reliability of our meta-analysis have been prudently and significantly improved in that the overall comprehensive estimation is based on a large sample size. In addition, sufficient sensitivity analysis has been carried out to ensure the reliability of this study.
The current systematically evaluated and meta-analysis has the following limitations and must be considered before our results are accepted. First, the selected studies in the systematically evaluated and meta-analysis were published between 2013 and 2020, the outcome evaluation indexes of the included studies were not completely consistent, and most of them did not adjust for confounding factors, meta-analysis evaluation data is insufficient. Second, the research included in this analysis is insufficient, and potential publication bias still exists. Third, this study only includes references in English. Therefore, we may have lost data from those in other languages.
Conclusion
In summary, our meta-analysis suggests that the risk of two-stage revision failure of PJI following TJA significantly boosted in obese patients. However, because there may be publication bias of this study, combined overall systematic review and meta-analysis results, we cannot yet conclude that BMI is associated with two-stage revision failure of PJI following TJA. This conclusion needs to be verified by more prospective studies.
Footnotes
Author contributions
(I) Conception and design: X Deng; (II) Administrative support: H Wang; (III) Provision of study materials or patients: J Guo, S Wu, W Chen; (IV) Collection and assembly of data: J Guo, H Wang; (V) Data analysis and interpretation: J Guo, S Wu; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.