
Abstract
Objective
Revision surgeries for periprosthetic joint infections (PJIs) in arthroplasty can follow either one- or two-stage treatment protocols. Previous studies have reported similar reinfection rates and reductions in complication rates for both treatment options. However, the literature on the selection of one protocol is still controversial. Thus, our aim was to compare the outcomes, including reinfections, complications, reoperations, and mortality, associated with one- and two-stage revision surgeries for PJI via a systematic review and meta-analysis of comparative studies.
Methods
Comparative studies were identified through searches in PubMed, EMBASE, the Web of Science, and the Cochrane Library as of November 2023. RevMan version 5.3 was used for the analyses. The included studies directly compared one-stage revisions with two-stage revisions for PJI. The primary outcomes included reinfection, complications, reoperation, and mortality.
Results
Sixteen cohort studies (fifteen retrospective and one prospective) were included in the systematic review. All studies comprising 2039 patients were included in the meta-analysis. Fourteen studies reported reinfection patient risk postrevision; when pooled via random effects models, 10.02% of patients in the one-stage group and 14.75% of patients in the two-stage group were reinfected, indicating low heterogeneity (risk ratio = 0.69; 95% CI = 0.50 – 0.94, I2 = 0%). A pooled analysis of ten studies reported complications between the two groups. Compared with the two-stage group, the one-stage group was associated with significantly fewer complications (risk ratio = 0.76; 95% CI = 0.63 – 0.91, I2 = 27%). The meta-analysis revealed no significant difference in reoperation events between the 1st-stage and 2nd-stage groups in nine studies (risk ratio = 0.77; 95% CI = 0.59 – 1.01, I2 = 20%) or in mortality in ten studies (risk ratio = 0.93; 95% CI = 0.49 – 1.78, I2 = 0%).
Conclusions
Among the available observational studies, the meta-analysis revealed a lower incidence of reinfection and complications in the one-stage group than in the two-stage group, but there were no significant differences in reoperation events or mortalities.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a challenging complication and is the most serious complication following shoulder, hip and knee arthroplasty, often necessitating revision surgery. The volume and cost of PJIs are increasing in parallel with the increasing number of joint replacements being used in aging populations. 1 The annual hospital cost of treatment for periprosthetic joint infection is estimated to be $1.85 billion by 2030. The incidence of PJI after primary joint arthroplasty has been reported to range from 0.7 – 4% after primary arthroplasty to 4 – 15% following revision arthroplasty. 2
The diagnosis of PJI, which is detected based on clinical, microbiological, histopathological, and biochemical criteria according to the definition of the Musculoskeletal Infection Society, 3 can be challenging. The optimal approach to PJI management, whether through debridement, antibiotics, or implant retention (DAIR) one- or two-stage revision protocols, continues to be a subject of debate in the orthopedic community. It has been reported that the risk for reoperation is as high as 36.6% after DAIR. 4 Certainly, PJI cannot be cured with antibiotics alone. The prosthesis needs to be exchanged using either a one-stage or two-stage surgical procedure; however, little information indicating which is better is limited.
Five recent meta-analyses support the view that one-stage revision is at least equally as effective as two-stage revision in controlling infection in shoulder, knee and hip PJI.5–9 However, the conclusions drawn from the above meta-analysis are based on a series of case reports rather than randomized controlled trials (RCTs) or comparative studies. Despite these studies analyzing the reinfection rates between both procedures, no comparative studies have analyzed patient prognosis. The heterogeneity of the results was high, and the reference value of the evidence was low. Therefore, this systematic review and meta-analysis, which is based on comparative studies aimed at critically evaluating and comparing patient prognosis, including reinfections, complications, reoperations, and mortality, is associated with one- and two-stage revision surgeries for PJI. We hypothesized that one-stage revision would have a better prognosis.
Methods
To systematically identify comparative studies contrasting one-stage and two-stage revision procedures for PJI, we conducted comprehensive searches in prominent databases such as PubMed, EMBASE, Web of Science, and Cochrane CENTRAL up to November 2023. For the purpose of analysis, we employed RevMan version 5.3 software.
Search strategy
This systematic review and meta-analysis adhered strictly to the Cochrane Review methods and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. Prior to commencing, we searched the PROSPERO database to confirm that no similar reviews were ongoing or recently completed, and we obtained a registration number (CRD42023464102) for this study. Our comprehensive search encompassed the MEDLINE, Embase, Web of Science, and Cochrane Library databases, spanning from their inception to November 2023. Additionally, we cross-checked the references of the included studies to further increase our recall ratio. The search was conducted via key terms such as “periprosthetic joint infection,” “PJI,” “revision,” “arthroplasty,” “two-stage,” and “one-stage.” To ensure the inclusivity of the latest research, we repeated the literature search just before Feb 29, 2024, to capture any newly published studies since the initial search.
Inclusion and exclusion criteria
The inclusion criteria were set to include studies that directly compared the outcomes of one-stage and two-stage revision surgeries for PJI. Our primary focus was on reinfection rates, postrevision complications, reoperations, and mortality. We did not apply any restrictions on country, study design, or methodology. However, we limited the search to articles published in English. All other types of studies, including editorials, letters to the editor, commentaries, brief abstracts, and case reports, were excluded from our analysis.
To ensure consistency and accuracy, two authors (D-X and YY-S) independently screened the studies identified through our searches based on the established inclusion criteria. In cases where there were any disagreements or uncertainties, the third author (X-L) served as an arbitrator to resolve any differences and ensure a unified approach.
Quality appraisal and assessment of risk of bias
The quality and assessment of the risk of bias for each study included in the review and meta-analysis were independently rated by two authors (H-X and X-L). The Newcastle–Ottawa Scale was used to assess the quality of the eligible studies. The scale is divided into three broad stratifications including selection (consisting of four items), confounder (including one item), and exposure (containing two items), each with a maximum score of four, one, or two points, respectively. The assessment was resolved by a third author (D-X).
Data collection and abstraction
Two reviewers (D-X and YY-S) independently extracted data from the included studies. They used a pretested data extraction form to ensure accuracy and consistency. The form captured key information such as the author, publication year, country, sample size, infection site, average follow-up duration, and any reported complications. The primary outcomes of interest were reinfection rates, postrevision complications, reoperations, and mortality. Any discrepancies between the two reviewers were promptly resolved through discussion with a third reviewer (H-X), ensuring the integrity and reliability of the extracted data.
Meta-analysis methods and subgroup analysis
A meta-analysis was carried out, encompassing data from a minimum of three studies, to gain a comprehensive understanding of the subject matter. Review Manager software (RevMan Version 5.3; Nordic Cochrane Centre; Copenhagen, Denmark) was utilized for this purpose. Heterogeneity among the included studies was rigorously assessed via both the chi-square test and the I2 statistic. A p value from the χ2 test less than 0.05 indicated the presence of significant heterogeneity. Consistent with the Cochrane Handbook for Systematic Reviews of Interventions, we adopted the following interpretation framework for the I2 statistic: values ranging from 0% to 40% were considered to represent low or possibly nonexistent heterogeneity; 30% to 60% indicated moderate heterogeneity; 50% to 90% suggested substantial heterogeneity; and values between 75% and 100% were indicative of considerable heterogeneity. If both I2 was less than 50% and p was greater than or equal to 0.1, it was concluded that there was insufficient statistical evidence of heterogeneity; thus, a fixed-effects model was employed for data analysis. However, in cases where these criteria were not met, a random effects model was chosen to account for the observed heterogeneity. Statistical significance was determined by comparing p values to an alpha level set at 0.05. Additionally, a sensitivity analysis was conducted to further explore potential sources of high heterogeneity among the studies. Finally, to assess the potential for publication bias, a funnel plot was generated for a single outcome derived from at least eight randomized controlled trials (RCTs). This analysis aimed to identify any systematic patterns or asymmetries in the distribution of study results that might indicate publication bias.
Results
Search results and qualitative analysis
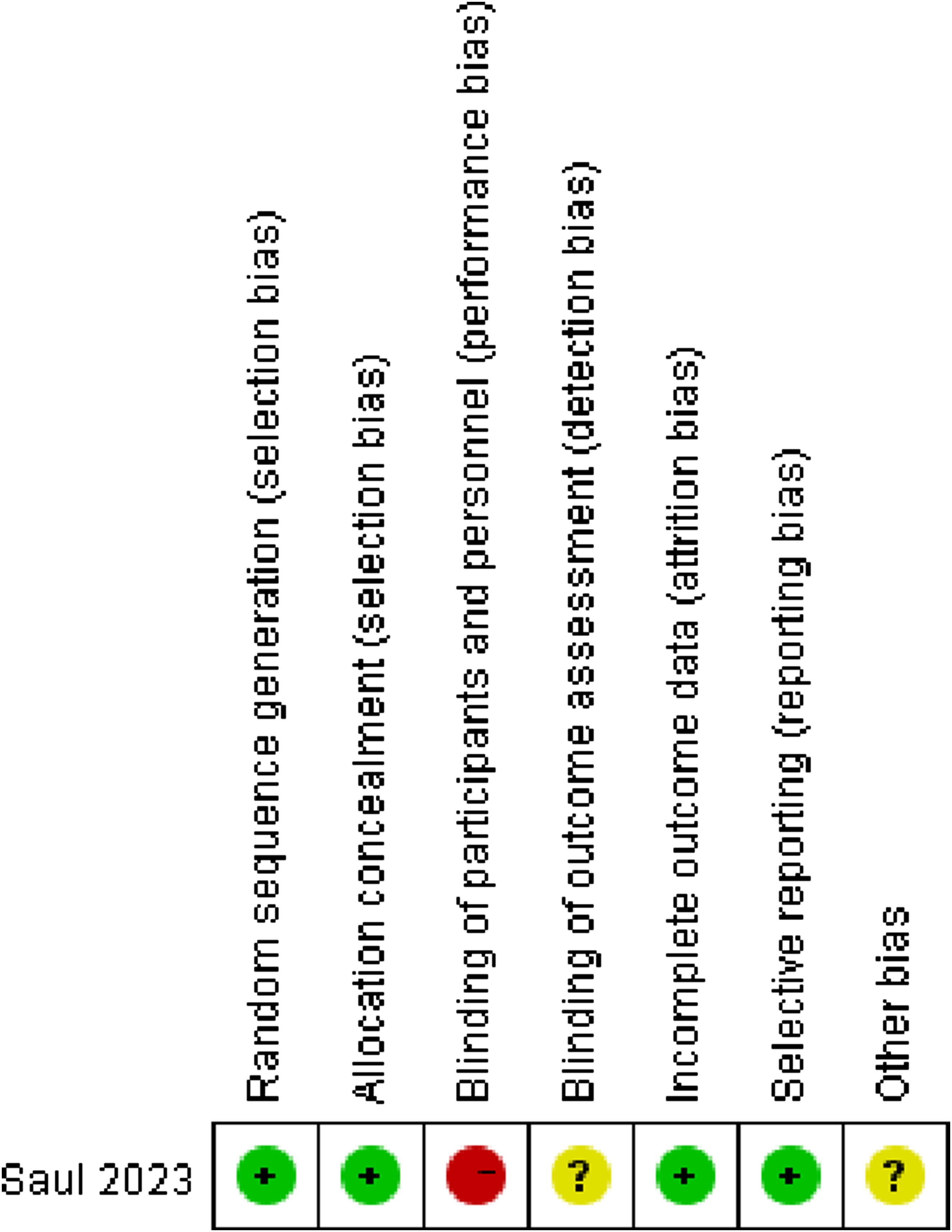
Our initial search identified 1006 potentially relevant citations plus 2 articles identified manually from the reference list. A total of 685 citations were identified after the removal of duplicates. Following title and abstract screening, 54 studies were assessed for full-text eligibility. A further 38 articles were excluded, leaving sixteen studies.4,10–24 Most of the studies were excluded on the basis of type and outcome relevance. A PRISMA flow diagram outlining the screening process and all the reasons for study exclusion is presented in Figure 1. A summary funnel plot was generated to assess publication bias that may have been present across studies reporting reinfection, with asymmetry testing performed suggestive of low risk (Supplementary File). The systematic search yielded a single randomized trial and fifteen cohort studies (comprising fourteen retrospective studies and one prospective study) eligible for inclusion in the systematic review. All studies evaluated using the NOS were confirmed to be of good quality. The range of the reported scores was 7–8. One included trial was at moderate risk of bias, as it satisfied four criteria used to assess the risk of bias (see Figure 2). The trial reported a low risk of bias in random sequence generation by concealed computer generation and allocation concealment by an independent statistician. However, owing to the nature of the intervention and recovery, surgeons and patients were informed of the allocation before surgery. Loss to follow-up was deemed satisfactory, as 90% of the patients randomized were analyzed at the endpoint. It seems unlikely that outcomes had been selectively reported as we obtained results, but it was unclear whether any other bias may have been present. If the surgeons were the ones making the assessment, they were unblinded (clearly), and there may be a moderate to high risk of bias. Study flow diagram. Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
The meta-analysis of the observational studies revealed a lower incidence of reinfection and complications in the one-stage group -than in the two-stage group. However, there were no statistically significant differences observed in terms of reoperation events or mortality between the two groups. Possible explanations include limited statistical power, severity of remaining complications, unrelated causes for reoperations, patient factors, study design biases, short follow-up periods, variability in surgical techniques, inconsistent outcome definitions, and random variation.
Study characteristics and relevant data.

Note: “-” represents not applicable. WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; SF-12: Short-Form 12; KSS: Knee Society score; PMA: Postal-Merle-Aubigne; VAS: visual analog scale; PROM: patient-reported outcome measure; IKS: International Knee Society; KOOS: knee injury and osteoarthritis outcome score.
Meta-analysis of reinfection
Fourteen included studies reported reinfection after revision of PJI. The meta-analysis demonstrated a significant difference between the one-stage group and the two-stage group (risk ratio = 0.69; 95% CI = 0.50 – 0.94; p = 0.02; Figure 3(a)). The statistical risk of heterogeneity for reinfection in the two groups was I2 = 0% (p = 0.59). A fixed effects model was applied. (a) Forest plots showing reinfection; (b) forest plots showing complications; (c) forest plots showing reoperation events; (d) Forest plots showing mortality.
Meta-analysis of complications
Additionally, pooled data from ten studies indicated significantly fewer complications associated with the one-stage approach than with the two-stage approach (risk ratio = 0.76; 95% CI = 0.63 – 0.91; p = 0.003). There was less heterogeneity (I2 = 27%; p = 0.20; Figure 3(b)).
Meta-analysis of reoperation
However, the meta-analysis did not reveal any significant difference between the one-stage and two-stage groups in terms of reoperation events (risk ratio = 0.82; 95% CI = 0.60 – 1.12, p = 0.05) based on data extracted from nine studies. A fixed effects model was used for low heterogeneity (I2 = 20%, p = 0.26; Figure 3(c)).
Meta-analysis of mortality
Ten studies recorded mortality after revision. The meta-analysis revealed no significant difference between the one-stage group and the two-stage group (risk ratio = 0.93; 95% CI = 0.48 – 1.8, p = 0.83). A fixed effects model was used because of the low heterogeneity (I2 = 0%, p = 0.82; Figure 3(d)).
Sensitivity and subgroup analysis
In this meta-analysis, the assessment of sensitivity and subgroup analysis is crucial, as it determines the validity and reliability of the combined results. We did not conduct subgroup analysis mainly for the following two reasons: first, some of the included studies did not clearly separate the surgical sites (such as the knee and hip joints), and other grouping methods were not suitable; second, the results of the meta-analysis showed low heterogeneity, and although all included studies were observational studies, the results have a certain degree of credibility. When heterogeneity is low in these findings, the studies included in the meta-analysis are relatively consistent, and the overall conclusions are more reliable. With respect to the outcomes, the removal of any single study from the analysis did not result in a deviation in the significance of the data.
Discussion
The results of this systematic review of sixteen studies suggest that there is a paucity of high-quality evidence comparing one-stage with two-stage revision surgeries for PJI. The findings from this systematic review and meta-analysis underscore the ongoing uncertainty regarding the comparative efficacy of one-stage versus two-stage revision surgeries for PJI. Although the analysis revealed lower reinfection rates and fewer complications associated with the one-stage approach, no significant differences were observed in reoperation rates or mortality between the two strategies.
The risk factors for PJI, which can be divided into patient- and surgery-related factors, are not easily modified except for intraoperative bleeding, high BMI, and advanced ASA class. 25 Improvements in treatment paradigms are needed, as are efforts to reduce orthopedic surgical site infections. Antibiotics are only one part of the therapeutic regimen and are auxiliary to the surgical strategy. 26 The common surgical procedures for PJIs include debridement, implant retention and antibiotic treatment (DAIR), two-stage exchange or two-stage exchange. DAIR has a relatively low success rate. Two-stage revision is the most common approach for the management of PJIs in the academic world. 27 However, reinfection rates have been shown to be similar between one- and two-stage revision for the treatment of PJI of the knee and hip in all published meta-analysis studies.5,7,8 Moreover, one-stage revision for PJI of the shoulder yields better results under appropriate conditions than does two-stage revision for infection control, with fewer clinical complications and possibly better clinical outcomes. The same result at 3 months after surgery was reported in the latest and, to date, the only published RCT. 11 Finally, no superiority was detected for prosthetic joint infection of the hip in the one-stage group at 18 months.
This is the first systematic review and meta-analysis to compare one-stage revision with two-stage revision directly on the basis of a comparative study. A meta-analysis of fourteen studies reporting reinfection rates after revision surgery revealed a reinfection rate of 10.02% in the one-stage group compared with 14.75% in the two-stage group. However, the reinfection rates in our study for both one- and two-stage revision arthroplasty were surprisingly greater than those reported in previous meta-analyses6. Possible explanations for this observed increase are an insufficient sample size and different durations of follow-up. With the extension of follow-up time, the rate of reinfection also increases. 24 To maintain baseline consistency, we did not include any case series reports, and approximately half of the included articles were from the past 3 years.
One-stage revision was associated with fewer complications than two-stage revision was in this meta-analysis. The Infectious Disease Society of America has published guidelines indicating that one-stage revision is more likely suitable for PJI patients with fewer comorbidities. 28 In Matar’s report, 23 patients who lacked systemic sepsis or a communicating sinus underwent one-stage revision. Thiesen et al. 16 reported that patients were 3.5 times more likely to suffer from medical complications if a two-stage revision was performed, and the average ASA score of the one-stage group was greater than that of the two-stage group. Like our findings, the meta-analysis by Rodrigues-Lopes revealed a greater rate of complications in the two-stage group for shoulder PJI. 29 Possible reasons include two-stage revision resulting in a longer length of stay, more damage to tissue, medical conditions ineligible for two major surgeries, later physiotherapy and recovery.30–32
Undoubtedly, reinfection and complications are the top concerns for PJI patients, and our failure outcomes also include reoperation and mortality. Previous meta-analyses did not analyze reoperation events, and not all patients who failed revision underwent remedial surgery.5–8 A meta-analysis of nine studies reporting reoperation rates after revision surgery revealed a reoperation rate of 15.25% in the one-stage group compared with 20.17% in the two-stage group. The occurrence rate of reopening after revision has been reported to range from 0% to 36.36%. Moreover, the impact of two-stage revision surgery might be greater than that of one-stage revision because a wait time between two stages indicates a longer period of immobility and greater psychological pressure. 33 Another study demonstrated that patients who experienced failure after revision of PJIs may never complete multiple reimplantation surgeries. 34 Repeated surgeries and uncertainty in prognosis are serious problems for patients and can increase the confidence of doctors. Regarding mortality during follow-up, previously published data on the differences in mortality rates after different PJI revision strategies are limited. Tirumala 20 and Thiesen et al. 16 reported no significant differences between one-stage and two-stage revision, which is analogous to our data. The mortality rate after revision was reported to be 0–2.5% in a previous report. 35 The medical condition of elderly patients is not always suitable for repeated extensive surgery. No patient was eager to undergo serial indefinite procedures for infection treatment. A higher ASA class was associated with increased mortality. 4
All these results highlight the need for further high-quality research, preferably randomized controlled trials, to provide more definitive conclusions regarding the optimal approach for managing PJI. A better understanding of the nuanced differences in patient populations, surgical techniques, and postoperative care between one-stage and two-stage revision surgeries is crucial in guiding clinical decision-making and improving outcomes for patients with PJI.
There are limitations that merit emphasis. Owing to the limited number of included RCTs, these results need careful interpretation, and our hypothesis could not be confirmed. The clinical results may be influenced by the low-quality evidence of the included studies, and it is difficult to provide conclusive opinions. Moreover, the uneven distribution of cases, antimicrobial therapy regimens and follow-up periods between the groups may also lead to potential bias. When deciding on treatment, surgeons should consider patient preferences and quality of life more. The reasons for the difference in prognosis between primary and secondary repair surgery should also include factors such as the surgical process, postoperative antibiotic treatment, and patient characteristics. These outcomes were not analyzed because of inconsistencies in the indicators and the lack of data on functional outcomes available for meta-analysis.
Conclusion
Prosthetic hip and knee joint infections are challenging to eradicate. There are not enough randomized clinical trials to provide reliable evidence for the indication of one-stage exchange or two-stage exchange. A previous meta-analysis suggested that one-stage revision might lead to a better prognosis in PJI patients. One-stage revision for PJI can represent an attractive option because there is no need for extensive second-stage surgery, and decreased reinfection and morbidity are expected in direct one-stage revision. Future research directions can include improving the research design, expanding the sample size, and delving deeper into specific patient groups.
Supplemental Material
Supplemental Material - Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis
Supplemental Material for Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis by Yiyuan Sun, Menghao Liu, Dan Xiao, Qi Li, Huan Xiong, Xue Luo, Boyu Zhu and Weili Fu in Journal of Orthopaedic Surgery
Supplemental Material
Supplemental Material - Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis
Supplemental Material for Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis by Yiyuan Sun, Menghao Liu, Dan Xiao, Qi Li, Huan Xiong, Xue Luo, Boyu Zhu and Weili Fu in Journal of Orthopaedic Surgery
Supplemental Material
Supplemental Material - Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis
Supplemental Material for Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis by Yiyuan Sun, Menghao Liu, Dan Xiao, Qi Li, Huan Xiong, Xue Luo, Boyu Zhu and Weili Fu in Journal of Orthopaedic Surgery
Supplemental Material
Supplemental Material - Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis
Supplemental Material for Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis by Yiyuan Sun, Menghao Liu, Dan Xiao, Qi Li, Huan Xiong, Xue Luo, Boyu Zhu and Weili Fu in Journal of Orthopaedic Surgery
Footnotes
Acknowledgments
We thank the Science and Technology Department of Sichuan Province for their contribution in the acquisition of the funding that supported this paper. This work was supported by the Sichuan Science and Technology Program (2024NSFJQ0041); 1.3.5 Project for Disciplines of Excellence of West China Hospital Sichuan University (ZYJC21030). This study was supported by the Department of Orthopedics, Orthopedic Research Institute, West China Hospital, Sichuan University.
Author contributions
Conceptualization, Y.S. and W.F.; methodology, Q.L.; software, Y.S. and D.X.; validation, D.X., X.H., and X.L.; formal analysis, Y.S.; investigation, Y.S.; resources, Y.S.; data curation, X.H.; writing—original draft preparation, Y.S.; writing—review and editing, all authors.; visualization, Y.S. and D.X.; supervision, W.F. and Q.L.; project administration, Y.S.; revision, M.L. and BY.Z.; funding acquisition, W.F. All authors have read and agreed to the published version of the manuscript.
Author’s note
We acknowledge i) that all authors listed meet the authorship criteria according to thes latest guidelines of the International Committee of Medical Journal Editors, and ii) that all authors are in agreement with the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sichuan Science and Technology Program (2024NSFJQ0041); 1.3.5 Project for Disciplines of Excellence of West China Hospital Sichuan University (ZYJC21030).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.