
Abstract
Purpose:
The purpose of this meta-analysis was to summarize the evidence of associations between obesity factors and spinal epidural lipomatosis (SEL) and to evaluate the strength and validity of these associations.
Methods:
Electronic databases such as Wiley Online Library, PubMed, Embase, Cochrane Library were searched and manual retrieval of references, the time limit was from the establishment of the database to May 2020. Methodological quality evaluations of the included studies were assessed using the bias risk assessment tool recommended by the Cochrane Guidelines. The RevMan 5.3 software was used for meta-analysis.
Results:
Finally, seven studies were included for meta-analysis, all of which were observational studies with mixed bias risk. These studies involved 807 patients, with an average age of 64 to 73.6 years, and 59.4 percent of the participants were male. The sample sizes for the included studies ranged from 28 to 288. The results of meta-analysis showed that high body mass index (BMI) was one of the factors affecting SEL (P < 0.01, MD 1.37, 95% CI [0.81, 1.92]). All reviews had a high risk of bias, and the most common source of bias was that there was no strict unified case diagnosis standard between researches, and some studies (four items) did not clearly describe the confounders that they controlled.
Conclusions:
We suggest that physicians should consider high BMI as a factor leading to SEL, and to control body weight actively should be considered as the preferred treatment strategy before surgical intervention is conducted.
Introduction
With the aging of the population, the improvement of social and economic level, and the increase of the number of people who are overweight, obesity-related issues have become a research hotspot. The probability of people of overweight or obesity presenting with back pain has been reported as high as three times as likely as those who are not obese. 1,2 Spinal epidural lipomatosis (SEL) is characterized by hypertrophy of unwrapped adipose tissue in the epidural space of the spinal canal. 3 –5 This thickening of fat often compresses the spinal cord or nerves leading to low back pain. The pathological manifestations are mostly mature adipocyte tissue, and there are few naive adipocytes with no biological characteristics of malignant tumors. Although SEL has been described as a rare disease by many scholars, the recent literature shows that the prevalence of SEL is between 6.2% and 8.6%, far more than previously reported. 6,7 This may be due to the combined effects of the development of imaging technology, the increase in obesity, and the aging of the population. 8 However, the reasons for the formation and development of SEL are still unclear. There are currently several hypotheses to explain the pathological mechanism of epidural fat accumulation. The widely evaluated factors are the use of exogenous steroids and the endogenous steroid overproduction caused by endocrine diseases such as Cushing’s disease, etc. 3,9 Fogel et al. 3 suggested that exogenous steroids group represents 55.3% of cases, 3.2% of the patients are due to the existence of diseases that increase endogenous steroid secretion, and obesity-associated disease represents 24.5% of cases. Another patients without steroid hormone interference is considered to be idiopathic SEL, and these patients often have increased body mass index (BMI); The high obesity rate of patients with idiopathic SEL suggests that obesity and SEL have a causal relationship. Other factors include that men are more likely to suffer from SEL than women. 10,11
In some cases, weight loss alone was sufficient to alleviate the clinical symptoms and reduce the volume of epidural adipose tissue. 12,13 Some scholars have suggested that for every percentage point increase in body weight, the likelihood of suffering from SEL increases by 13%. 14 Up to now, although many literature has shown that obesity has a clear correlation with SEL, most of them are isolated case reports and small sample case series. In general, whether obesity is an influencing factor is still controversial. Some reported studies showed that there is no significant correlation between SEL and BMI. 15 It has also been suggested that patients with SEL have a high BMI. 16,17 We hope to clarify the correlation between obesity and SEL through systematic search and review of the literature, to provide a reference for further discussion of the etiology and mechanism of SEL.
Methods
We conducted a systematic review of reviews in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (http://www.prisma-statement.org/).
Search strategy
A comprehensive search was conducted in the electronic databases such as Wiley Online Library, PubMed, Embase, Cochrane Library, the time limit was from the establishment of the database to May 2020. Taking PubMed as an example, the specific search strategy is shown in Table 1. In addition, the related review literature is consulted, and the references of the included literature are manually searched.
Search strategy.

Inclusion and exclusion criteria
We applied specific inclusion criteria in the selection process. (a) All studies that report the correlation between BMI and SEL (as a relative risk, or the assessment of sensitivity and specificity, or sufficient evidence can be obtained from the article); (b) The diagnosis of SEL is derived from the symptoms and signs displayed by the patient or from the imaging findings; (c) The experimental design was a cross-sectional study, a cohort study, a case-control experiment, and a prospective or retrospective analysis experiment.
The main exclusion criteria that were applied during the selection process were as follows: (a) Studies that participants have a long history of systematic steroid injections (≥3 months); (b) Participants have other pathological features: any primary or secondary tumor in the spinal canal, abscess, hemangioma, and epidural hematoma; (c) Non-chinese or English literature; (d) Repeated publications of the same data; (e) Animal experiments, meeting abstracts, reviews, etc.
Data extraction and quality assessment
Two reviewers independently screened the literature based on the established study selection and exclusion criteria. Initially identified the article title and abstract, read the full text of the remaining literature, and finally determine the included studies. The other two reviewers extracted the relevant research data of the included articles, including the first author of the article, year, country, sample size, experimental design, BMI, age and sex ratio of each group and medical history. Any differences in the above process shall be settled through consultation with a third reviewer. If the article data is incomplete, we will contact the author to obtain relevant experimental data. If the corresponding data is still not available, the article will be included in the systematic review for a qualitative description.
The methodological quality assessment of the included studies was conducted using the Newcastle-Ottawa Quality Assessment Scale (NOS), a bias risk assessment tool recommended by the Cochrane Guidelines. The NOS scale scoring system evaluates the quality of the included literature through the selection of study subjects, comparability between groups, determination of exposure factors and outcome indicators in case-control and cohort studies. Articles with a NOS score of six or more are eligible for meta-analysis, and studies with a score of seven or more are considered high-quality literature. The quality evaluation process was conducted independently by two reviewers. All disputes were settled through discussion with a third reviewer.
Statistical analysis
Meta-analysis was performed using RevMan 5.3 software provided by Cochrane Collaboration Network. Continuous variable data was expressed as mean difference (MD) and its 95% confidence interval (CI), and count data was expressed as Odds Ratio (OR) and its 95% CI. The heterogeneity test between the included studies was analyzed using I 2 statistics. If there was no heterogeneity or the heterogeneity was small (I 2 ≤ 50%, P ≥ 0.05), the fixed-effect model was used to calculate the combined effect. On the contrary, if the heterogeneity is large (I 2 > 50%, P < 0.05), analyze the source of heterogeneity. If there is only statistical heterogeneity, the random effect model is used to combine the effect sizes. Otherwise, only descriptive analysis is performed. Potential publication bias was assessed for meta-analysis by graphical and statistical tests, namely the funnel plot and Egger’s test. These were conducted with the Stata version 12 (Stata Corporation, College Station, USA). P < 0.05 was considered statistically significant.
Result
Study selection
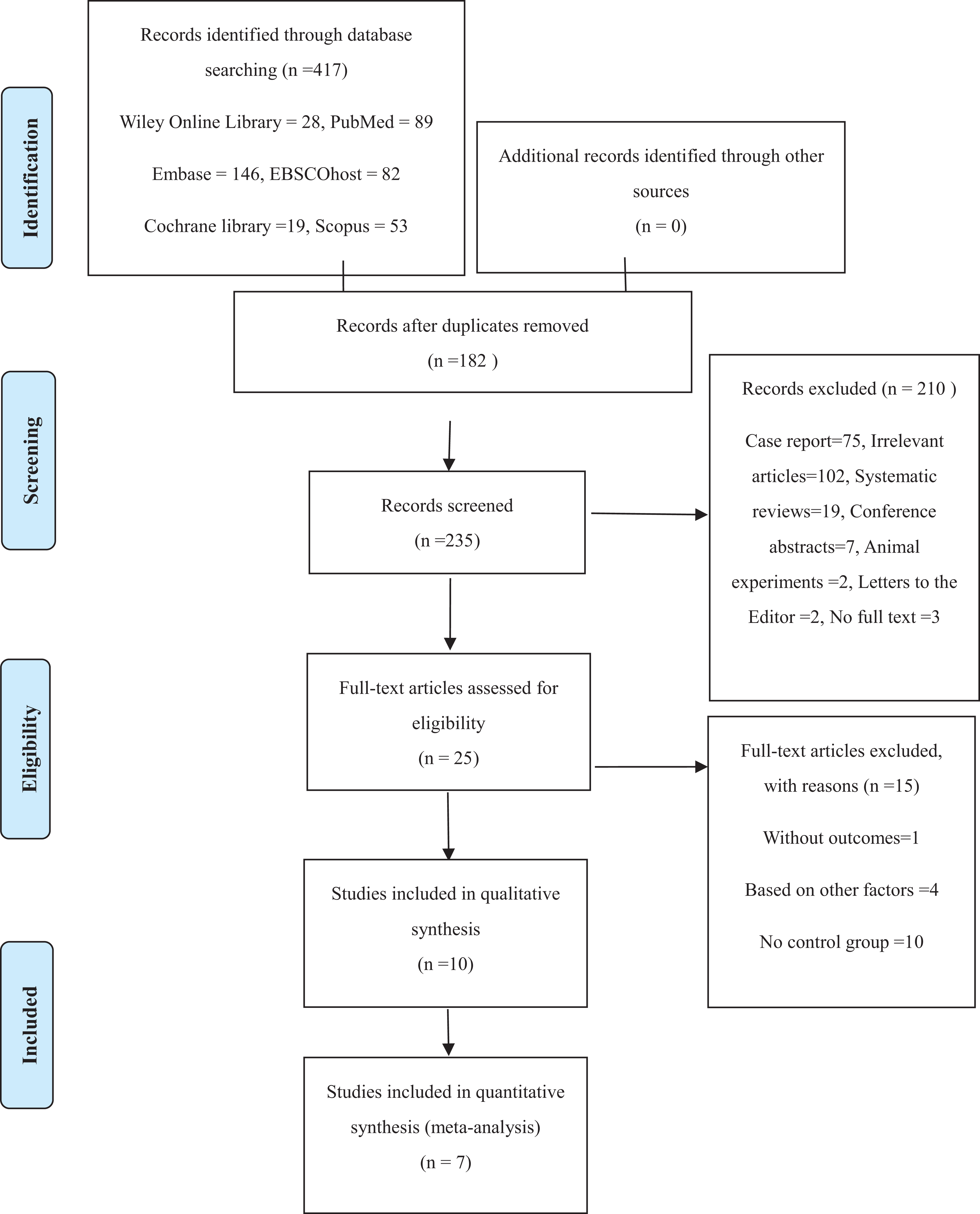
In total, 417 studies were found in the electronic database search, of which 182 were duplicates. After screening the title and abstracts, 25 relevant studies remained and underwent detailed full-review. Of these, 15 was excluded due to lack of a suitable outcome, inappropriate study design, or based on other factors. A total of seven articles met the eligibility criteria and were included in the meta-analysis. The process of relevant studies selection and the number of articles excluded at each stage are outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Table 2).
Study flow diagram.

Characteristics of the include studies
Table 3 describes the study characteristics of the seven studies included in our meta-analysis. A total of 807 individuals were identified in seven studies. We found one prospective study and six retrospective studies involving case-control studies in five countries: five from Japan, one from Germany, one from Jordan. Sample sizes ranged from 28 to 288. The average age of the participants ranged from 64 to 73.6. And 59.4% of the patients were male. The medical histories of the patients in each study we collected are shown in Table 3.
The general characteristic of the included studies.

Note: DM, diabetes mellitus; HD, heart disease; HL, hyperlipidemia; HTN, hypertension; NA, not mentioned.
Risk of bias
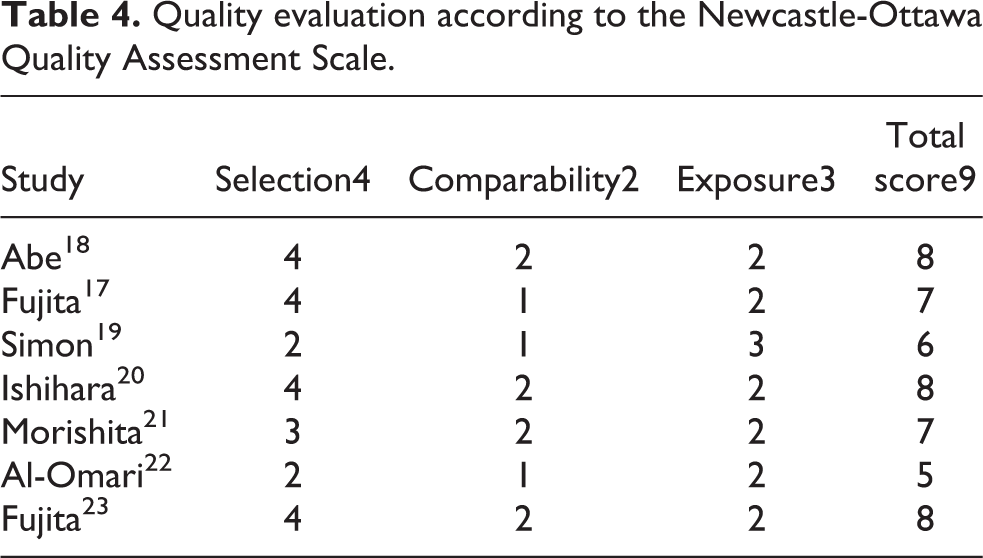
The Newcastle-Ottawa Scale was applied to assess the selection, comparability, and exposure of the case-control study. These methodological quality scores included in the study are shown in Table 4. There were seven articles of high quality, one article of medium quality and two articles of low quality. Retrospective experiments usually have a higher risk of recall bias.
Quality evaluation according to the Newcastle-Ottawa Quality Assessment Scale.
Meta-analysis
Seven literature met the meta-analysis criteria. The statistical results show that the heterogeneity between the initial studies is significant, the source of heterogeneity may be that there is no uniform standard for the diagnosis of SEL in various studies. Four studies 17,18,20,23 defined SEL as an EF/SpiC index greater than 0.4 or 0.6, four reviews 19,21,24 diagnosed as SEL based on MRI showing enlarged fat tissue compressing the dura sac, two studies 14,22 obtained the diagnosis basis based on clinical symptoms and signs and MRI imaging but did not clearly explain. The results showed significant heterogeneity after the initial combination of effect sizes (I 2 = 98%). However, we searched for sources of heterogeneity by the article-by-article elimination method, and after excluding one study, 24 the heterogeneity between studies was significantly reduced (I 2 = 17%). The results suggest a positive correlation between SEL and BMI (Figure 1). Under the fixed-effect model, the MD given by the meta-analysis is 1.37, 95% CI [0.81, 1.92], indicating that there is a positive correlation between the observed variable and the outcome variable. Still the strength of the correlation is weak.

Mean difference of BMI between the SEL group and the non-SEL group. SD standard deviation, CI confidence interval, IV inverse variance.
We also conducted a meta-analysis to determine whether coexisting systemic diseases have an impaction between SEL versus non-SEL patients. The result showed that there was no statistically significant difference between the SEL group and the non-SEL group in terms of combined diabetes (OR 1.39; 95% CI [0.87, 2.23]; P = 0.17; Figure 2), HL (OR 1.46; 95% CI [0.93, 2.32]; P = 0.10; Figure 3), HD (OR 1.42; 95% CI [0.73, 2.76]; P = 0.30; Figure 4).

Odds ratio of diabetics between the SEL group and the non-SEL group.

Odds ratio of hyperlipidemia between the SEL group and the non-SEL group.
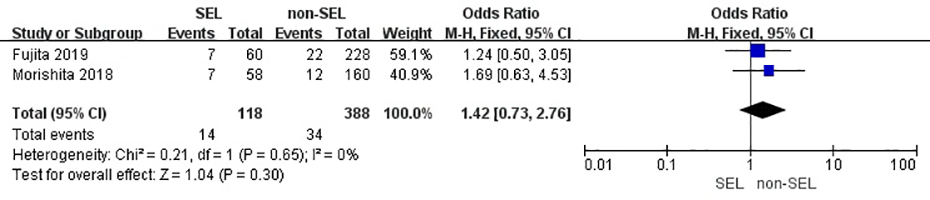
Odds ratio of heart disease between the SEL group and the non-SEL group.
Publication bias
According to the Egger’s test, there was no evidence of significant publication bias for BMI in meta-analysis comparing SEL versus non-SEL (t = 0.90, P = 0.419), and funnel plot showed a good symmetry (Figure 5). Therefore, our results indicated that there was little presence of potential publication bias.

Funnel plot to assess publication bias of efficacy rate.
Discussion
The results of this study showed that SEL was positively correlated with BMI, although the correlation was weak. We considered the influence of coexisting other systemic diseases on SEL. And the results showed that there was not enough evidence to prove that patients with systemic diseases such as hyperlipidemia, diabetes and heart disease were more likely to develop SEL. To a certain extent, the interference of other factors was controlled, which further proved the conclusion that BMI was positively correlated with SEL. Furthermore, in this meta-analysis, we managed to balance the heterogeneity of the included literature as much as possible through the article—by—article elimination method. However, heterogeneity might have arisen from several sources, among which study design was the most prominent sources. Relatively small sample sizes, incomplete matching, and insufficient representative samples generated from a single center constitute some limitations that may have caused additional heterogeneity. Certainly, the observed heterogeneity could be attributable to differences in behavioral factors, the country of origin, and methodological factors concerning the study design.
This is the only meta-analysis that has reported association of obesity and SEL. SEL is one of the representative diseases of fat ectopic deposition. Because the morbidity of the disease is relatively low, clinical studies of large samples are almost rare. Asymptomatic SEL is generally only found during a health examination. At a same time, symptomatic SEL affects the quality of life of patients with varying degrees of low back pain or cauda equina syndrome.
We consider that the pathological mechanism of obesity leading to epidural fat deposition may be the disorder of glucose and lipid metabolism firstly. Based on the close relationship between visceral fat accumulation and abnormal lipid metabolism, 25 –27 it is speculated that SEL may be another site of systemic fat accumulation caused by abnormal lipid metabolism; Secondly, high BMI and obesity are considered as a chronic inflammatory state, which may be one of the causes of excessive growth of adipose tissue in the spinal canal. Hypertrophic adipocytes continued to express pro-inflammatory cytokines, tumor necrosis factor TNF-α, interleukin-1β, etc. High levels of adipocytokines (such as adiponectin and leptin), are involved in energy metabolism and inflammation regulation. These factors are also expressed in the adipose tissue of SEL patients with hyperplasia. 28 Fujita et al. 23 also confirmed the increased expression levels of inflammatory cytokines such as tumor necrosis factor-a and interleukin-1b in the adipose tissue of patients with SEL hyperplasia. Besides, we hypothesized that ectopic lipid deposition is also regulated by genes or molecules: Khan et al. 29 reported that mice lacking collagen VI (mainly expressed in adipose tissue) might experience unrestricted expansion of adipose tissue and a significant increase in insulin sensitivity under a high-fat diet. It shows that when the fat stored in adipose tissue is reduced, it will cause the lipid to be stored in non-adipose tissue (e.g., liver, skeletal muscle, pancreas, etc.), and affect the metabolic function of these organs. Leptin is synthesized and secreted by white adipose tissue. Its physiological role is to bind to the leptin receptor in the hypothalamic appetite center, which plays a role in inhibiting food intake, increasing energy consumption, and inhibiting fat synthesis. Therefore, the leptin regulatory system is considered to be one of the endocrine mechanisms that play a central role in body weight, body fat distribution, and metabolic diseases; Leptin expression is reduced, and the expression of the cellular inflammatory factor adiponectin is reduced, resulting in abnormal body fat distribution. 30 In addition to obesity, other factors may also lead to abnormal fat distribution and cause the occurrence of SEL, such as deformed osteoarthritis, congenital spinal stenosis, and the use of lipase inhibitors, there is insufficient evidence-based evidence. 31 –35
Limitations
Compared with previous studies, we were no longer limited to the evidence provided by the case report, but scientifically proved the relationship between BMI and the development of SEL by using the meta-analysis method. However, there are limitations in our study: the first is that most of the included studies are retrospective observational studies. Inevitably, the results of comprehensive analysis of various studies can only provide weak clinical evidence to prove the relationship between variables; In addition, we have not collected information about the percentage of body fat, these can make up for BMI indicators can only provide simple evidence of obesity. In a given BMI category, differences in the average percentage of body fat among ethnic groups may also contribute to some of the differences observed. For example, Asians generally have higher levels of fat compared to Caucasians for the same BMI. 36 Therefore, their independence and potential confounding effects remain unknown. Besides, there are few relevant case-control studies published at domestic and overseas, our analysis may have a higher risk of mixed bias. However, the results of this study still have particular reference value. In the future, more high-quality randomized controlled trials are still needed to determine the clear correlation between BMI and SEL.
Conclusions
The exact mechanism of SEL development is difficult to determine, suggesting that large demographic studies with appropriately selected control groups are needed to establish pathogenic factors. Our results are only a reference for the etiology of SEL. We suggest that surgeons should consider obesity as a possible factor leading to SEL and take active control of BMI as the preferred treatment strategy before considering surgical intervention, to reduce the mental and economic burden of patients.
Supplemental material
Supplemental Material, sj-doc-1-osj-10.1177_23094990211027391 - Obesity is a risk factor for epidural lipomatosis: a meta-analysis
Supplemental Material, sj-doc-1-osj-10.1177_23094990211027391 for Obesity is a risk factor for epidural lipomatosis: a meta-analysis by Bi Zhang, Haifeng Yuan, Lihong Hu and Muhammad Saad in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Natural Science Fundation of China (no. 81160220), The Natural Science Fundation of Ningxia Province (no. NZ17153), First-Class Discipline Construction Founded Project of NingXia Medical University and the School of Clinical Medicine (NXYLXK2017A05).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.