
Abstract
Keywords
Introduction
Chronic pain is a public health problem, incurring burden on patients’ lives 1 as well as the economy and society. 2 Musculoskeletal pain is especially important as it is a major driver of hospital and outpatient visits 3 and complementary and alternative medicine (CAM) use. 4 CAM is a category of medicine that includes various treatment approaches that fall outside the realm of conventional medicine. 5 It includes acupuncture, chiropractic, and osteopathy and is often used in combination with conventional treatment.6–8
For relief from persistent pain, many people seek care from multiple healthcare providers 1 and visit them frequently;1,9 however, it is common that pain is not adequately managed from the patients’ perspectives. 1 In previous studies conducted in Japan, of the 42% patients with chronic musculoskeletal pain sought treatment from conventional medical and CAM practitioners (approximately 20% for each), only 36% were satisfied with the treatment 10 and a majority of the patients changed healthcare providers10–12 or even withdrawn from treatment.11,12 Furthermore, 55% do not seek professional help and remain untreated despite persistent pain and disability. 10
To improve the treatment of chronic musculoskeletal pain, it is important to identify the factors associated with decisions regarding the use of healthcare. Consideration should be given to the relationship between pain and mental health (depression and anxiety disorders12–14 and communication with the therapist 15 ) and the importance of understanding patient’s expectation in pain management, 16 and factors that influence treatment satisfaction should also be considered.
A comprehensive framework, the Behavioural Model, was established by Andersen in 1973 to help understand the use of healthcare by patients, incorporating multi-dimensional factors.17,18 When this model is adopted, the care-seeking behaviour of the people can be classified into three factors: (1) predisposing (individuals’ predisposition to use services, e.g. demographic characteristics and social status, and attitude/beliefs about health and healthcare), (2) enabling (ability to allow oneself to use services, e.g. personal or community resources), and (3) need (perception and/or objective judgment on health status or severity level of illness and their need for medical care).17,18 These factors contribute to healthcare resource use, while the use does not take place only by one factor.17,18 Adopting the Behavioural Model, a previous study performed in Iceland found that access, and pain- and disability-related factors and physical health-related quality of life (HRQOL) is related to healthcare utilisation of subjects with chronic pain. 19 Another study performed in the US reported that socio-demographic, medical, and pain- and disability-related factors and perception of care and pain control predicted use of CAM by chronic pain subjects. 20
By understanding the whole picture of the characteristics and care-seeking behaviours of patients with chronic musculoskeletal pain, we may be able to suggest an important hint to improve the quality of pain management. Such suggestion is expected to lead to prevent patients from withdrawing from the necessary treatment, to achieve desirable pain relief.
Therefore, we conducted this study to delineate the care-seeking behaviours of people living with chronic musculoskeletal pain, which limits activities of daily living (ADL) and/or work and explore the factors behind the choice of healthcare providers across Japan. An online survey method was adopted in order to include participants who were determined not to consult healthcare providers and to ensure the enrolment of a sufficient number of participants to obtain reliable results while reflecting the demographic composition of the Japanese population. Using the data collected online, we described the characteristics of people with chronic musculoskeletal pain who consulted: 1) physicians, 2) CAM practitioners and 3) no healthcare providers; explored possible factors associated with healthcare utilisation; described subjective reasons for the current and past healthcare utilisation and analysed the factors that affect satisfaction with the healthcare providers of choice.
Methods
Study design
This is a cross-sectional questionnaire survey among people with chronic musculoskeletal pain, which interferes with ADL/work. The survey was conducted online from February to March 2019. The survey consisted of two stages. First, a simple initial survey was performed to screen eligible participants for the main survey. Second, the main questionnaire that tackled more focused questions was sent to the eligible participants identified in the initial screening.
Study population
As an initial survey for screening, a randomly selected sample group created via an online survey panel (Macromill Inc., Tokyo, Japan) composed of approximately 1,300,000 voluntary registrants residing all over Japan was used. The panel is designed to avoid double registration as much as possible. In order to create the sample group, which was intended to reflect the demographic composition of the Japanese population, participants were specified as being residents of Japan who were ≥ 20 years of age, and quotas were then set for age, sex, residential areas and personal annual income distributions to correspond to the Japanese population as a whole.
For the initial survey, age ≥ 20 years was the only criterion for obtaining the sample group, and no exclusion criterion was set. The invitation for the initial survey was e-mailed to 573,729 survey panel registrants online in February 2019. This sample size was set on the basis of collecting responses from up to 10,000 participants in the main survey, taking into account the panel’s intention to reflect demographic composition of the Japanese population, prevalence of chronic musculoskeletal pain in Japan (15–28%)10,21,22 and the expected response rate (around 10% by the panel performance). For those who agreed to participate, the following questions were asked: (1) their age, (2) presence of pain (yes/no) within the past month at any of the following parts of the body: neck, back, lumber, shoulder, arm, elbow, hand, hip, thigh, knee, lower leg and foot, (3) duration of pain (<3 months/3–<6 months/6–<12 months/1–<2 years/2–<3 years/3–<4 years/4–<5 years/≥5 years), (4) interference of pain on ADL or work (yes/no) and (5) whether the cause of the pain was diagnosed as cancer or fracture (yes/no/do not want to answer). The categorisation of pain duration was determined based on a previous study. 10
From the respondents in the initial survey, individuals who met all of the following criteria were included in the main survey: age ≥ 20 years and musculoskeletal pain that was present within the past month, persistent for ≥6 months, and interfering with ADL/work, but the cause of pain was not cancer or fracture. Those who did not want to answer the cause of pain in the initial survey were excluded. For those who met the above criteria, invitations for the main survey were sent online in March 2019.
Measures
For those who agreed to participate in the main survey, detailed questions on their characteristics, condition of pain and healthcare utilisation were asked.
Respondent characteristics
Information on sex, educational attainment, employment status, types of work involved and annual household income in Japanese yen was collected (details in response choices to these questions are shown in Supplementary Table S1a).
Conditions of pain- and health-related quality of life
The frequency of pain interfering with ADL or work (<once a month/≥once a month to <once a week/≥once a week to <twice a week/≥twice a week), the intensity of pain on a numeral rating scale (NRS) (0: no pain to 10: worst pain) 23 and the distribution of pain was asked. Information on neuropathic component of pain was collected using painDETECT,24,25 and information on catastrophizing of pain was collected using the pain catastrophizing scale (PCS).26,27 Considering the NRS, scores ≤4, 5–7 and ≥8 were used to classify the intensity of pain as mild, moderate and severe, in line with a previous study. 1 The Japanese-validated version of Short Form 8™ Health Survey (SF-8) 28 was used to assess health-related quality of life, taking into account the burden of participants answering a large number of questions.
Healthcare utilisation
The respondents selected the healthcare provider they had chosen at the time of the survey or previously for the treatment of chronic musculoskeletal pain from: 1) physicians (at hospitals and clinics), 2) CAM practitioners (osteopathy, Japanese bone setting [hereafter, osteopathy {bone setting}], chiropractic, massage, and acupuncture and moxibustion) or 3) no consultation (no consultation with the above healthcare providers, i.e. untreated).
For those who visited physicians or CAM practitioners, information was obtained on the clinical department, type of CAM therapy, the type of physician’s facility, types of treatment/therapy provided by physician, average waiting time at the treatment facility, accessibility of visiting the treatment facility for the treatment/therapy of chronic musculoskeletal pain and assistance for healthcare visits. Perception of the treatment/therapy effect was measured by a change in the respondent’s overall status since they started the healthcare consultation using a modified version of Patient’s Global Impression of Change (PGIC). 29 Additionally, subjective reasons for current and past healthcare utilisation (detailed response choices shown as Supplementary Table S1c), and satisfaction with healthcare providers (very satisfied/satisfied/somewhat satisfied/somewhat dissatisfied/dissatisfied/very dissatisfied) were asked. To assess the relationship between patient and healthcare provider, positive impressions of communication (agree/disagree), of physicians/practitioners’ attitudes (agree/neutral/disagree) and of ownership over treatment decision making (agree/neutral/disagree) were also asked.
Statistical analysis
For the analysis, respondents of the main survey were grouped into 1) physician, 2) CAM and 3) untreated groups, based on the use of current healthcare providers. Respondents who were consulting with physicians and CAM practitioners concurrently were grouped into the physician group.
Descriptions of factors included in the survey.

ADL: activities of daily living
aRespondents in untreated group did not respond to the questions regarding accessibility.
bOnly the respondents who visited physicians and/or CAM practitioners responded to the questions regarding this factor.
The association of predisposing, enabling, and need factors with the current healthcare utilisation was described based on the summary of these factors and a multivariate multinomial logistic regression model to consider potential confounding effects between the factors. Preliminary analysis was conducted using Spearman correlation coefficients and univariate logistic regression to construct the analysis model. All independent variables of predisposing, enabling and need factors were considered relevant and were included in the final model. The final models were evaluated using fitness parameters (pseudo R-squared, and the likelihood ratio). The variance inflation factor (VIF) was also measured to ensure that there was no concern for multicollinearity (VIF <10).
Furthermore, subjective reasons for the current healthcare utilisation and reasons for the past healthcare utilisation patterns (e.g. switch from physicians to CAM practitioners, switch from CAM practitioners to physicians) were also summarised.
Finally, the degree of satisfaction with healthcare providers, assessed as a part of perception of the respondents, was summarised based on the current usage of healthcare providers, except for the untreated group. The association between the satisfaction and respondents’ perceptions (impression of communication, physician’s/practitioner’s attitudes and ownership over treatment decision making) and healthcare details (clinical departments that the respondents visited and types of CAM therapies) were analysed using multivariate logistic regression models for each group of healthcare provider adjusting the effect of covariates of age, sex, annual household income, NRS, painDETECT score, PCS score, physical component of SF-8, and mental component of SF-8, types of physician’s facility (for physician group), types of treatment provided by physician (for physician group), average waiting time at the physician’s and CAM practitioner’s facility and impression of treatment effect (modified version of PGIC 29 ) provided by physicians and CAM practitioners. To perform this multivariate logistic regression analysis, the options of very satisfied, satisfied and somewhat satisfied were categorized as ‘satisfied’, and those of somewhat dissatisfied, dissatisfied and very dissatisfied were categorized as ‘dissatisfied’. In deciding the variables to be included in the model, factors that are known to affect patient satisfaction from previous research were chosen from all the variables collected like (details shown as references) sex, 30 age, 31 annual household income, 32 pain intensity, 33 catastrophizing, 34 neuropathic component of the pain, 35 HRQOL, 36 waiting time at the treatment facility, 37 types of physician’s facility 38 and impression of treatment effect.
For the logistic regression analyses, association was considered significant at a p-value of <0.05. Completion of the initial screening and main surveys required mandatory responses to all the questions, and thus there were no missing data. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethical statements
This study was approved by the Institutional Review Board of Keio University (approval number: 20180217). All the survey respondents gave their consent electronically and were compensated by vouchers (shopping points). In both the initial survey and the main survey, participants were instructed to answer alone. As a helpline, an inquiry form was set on the panel page so that respondents could ask about how to answer questions, how to operate and how to cancel the answer (including withdrawal of consent).
This study was conducted in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects. 39 No personally identifiable information was included in the dataset provided by Macromill Inc.
Results
Current healthcare utilisation
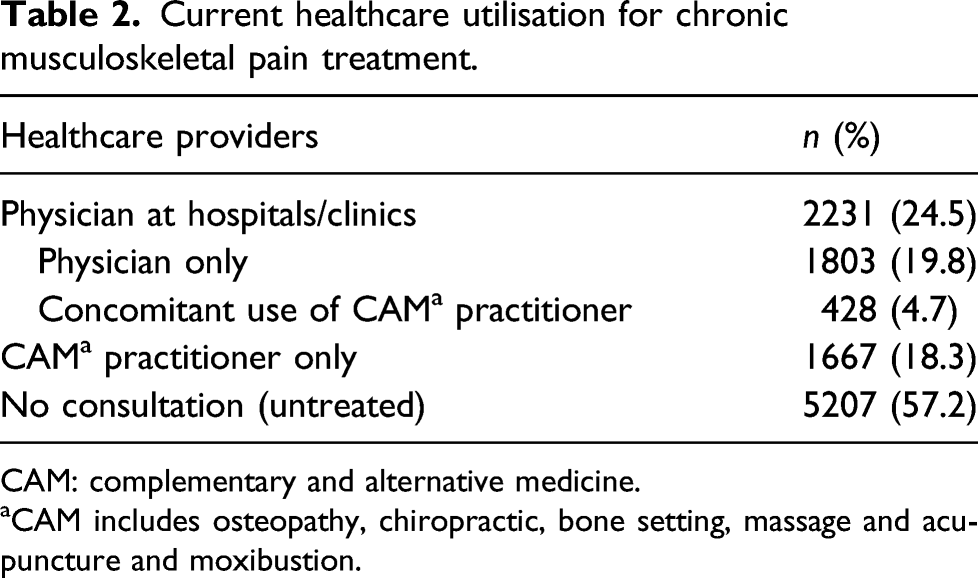
Among 94,911 respondents from the initial screening survey, 94,780 completed the questionnaire. Among these, 12,467 met the screening condition for the main survey. The questionnaire of the main survey was sent to them, and 9105 completed this questionnaire (Figure 1). Among these main survey respondents, 2231 (24.5%) were currently visiting physicians at hospitals or clinics (physician group); 1803 (19.8%) were consulting with physicians only and 428 (4.7%) were concurrently consulting with CAM practitioners. 1667 (18.3%) were currently visiting CAM practitioner (CAM group); and 5207 (57.2%) were currently visiting no healthcare providers (untreated group) (Table 2). Scheme of the participants recruitment. (ADL: activities of daily living). Current healthcare utilisation for chronic musculoskeletal pain treatment. CAM: complementary and alternative medicine. aCAM includes osteopathy, chiropractic, bone setting, massage and acupuncture and moxibustion.
Characteristics of the respondents according to the type of current healthcare utilisation
Characteristics of respondents according to the current usage of healthcare providers.

CAM: complementary and alternative medicine, PCS: pain catastrophizing scale, ADL, activity of daily living, NRS: numerical rating scale.
aCAM includes osteopathy, chiropractic, bone setting, massage and acupuncture and moxibustion.
b1 million (1,000,000) JPY = 9,412.63 USD as of September 2, 2019.
About the perceived treatment effect, the overall status was slightly improved or much improved in the physician group (46.9% and 25.1%, respectively) and in the CAM group (53.9% and 32.9%, respectively) (Supplementary Table S3). Concerning the area of the body where pain was experienced, most patients in the physician group experienced pain in the lower body whereas most patients in the CAM group experienced pain in the upper body (Supplementary Table S4).
Factors associated with the current healthcare utilisation
Multivariate logistic regression for current healthcare utilisation a (vs. untreated).

CAM: complementary and alternative medicine, SE: standard error, OR: odds ratio, ref: reference, CI: confidence interval, PCS: pain catastrophizing scale, ADL, activity of daily living, NRS: numerical rating scale, HRQOL: health-related quality of life, SF-8: Short Form 8™ Health Survey.
aThis model includes the variables of educational attainment, employment status and types of work involved (results shown in Supplementary Table S5), in addition to all the variables shown in this table. The pseudo R-squared value, likelihood ratio chi-square and the statistical degrees of freedom were 0.18, 1550.87 and 90, respectively.
bPhysician at hospitals/clinics includes respondents who were consulting with physicians and CAM practitioners, concurrently.
cCAM includes osteopathy, chiropractic, bone setting, massage and acupuncture and moxibustion.
d1,000,000JPY = 9,412.63 USD as of September 2, 2019.
Factors positively associated with selecting CAM practitioner were gender (female), a higher painDETECT score, a higher household income, pain duration of ≥5 years (vs 6–<12 months), more frequent interfering pain and a higher NRS. Negative associations were found in the age of 50–59 years (vs 20–29 years), employment status of temporary employee, helping family business, housewife/househusband, and unemployed (vs regular employee), absence or no need of assistance for healthcare visit and a SF-8 mental component score of ≥50.
Subjective reasons for the current healthcare utilisation
Regarding the subjective reasons for selecting the current healthcare provider, expertise (49.0%) was most common in the physician group, and expectation of treatment effect (46.0%) was most common in the CAM group (Supplementary Table S6). In 45.3% of untreated group who had never consulted with either healthcare providers, cost was the most common reason for not consulting for never visiting physicians and CAM practitioners (Supplementary Table S7).
Past experience of healthcare utilisation
Among the respondents, 49.2% (4480/9105) had experienced switching or withdrawing from the healthcare provider visits; 30.9% (690/2231) in the physician group had previously visited CAM practitioner only, and 56.6% (944/1667) in the CAM group had previously visited physicians and 54.7% (2846/5207) in the untreated group had withdrawn from visiting physicians or CAM practitioners. Those who resumed consultation accounted for 44.6% (996/2231) in the physician group and 59.7% (1251/2095) in the CAM group and in those who were concomitantly visiting CAM practitioner in the physician group.
The most common reasons for the switch in the physician group were cost (27.1%) and treatment not being effective (25.9%). The most common reasons for the switch in those in the CAM group were treatment not being effective (40.6%) and long waiting time (20.7%).
Among those who had withdrawn from visiting physicians or CAM practitioners (untreated group), reasons for withdrawal from physicians were treatment not being effective (35.9%) and pain improvement (26.2 %); and reasons for withdrawal from CAM practitioner were cost (38.2 %), not enough time for visits (34.1%).
In those who resumed physician consultation after withdrawal, the common reasons were pain worsening (17.5%) and incapability of self-management (15.9%); in those who resumed CAM practitioner consultation, their common reasons were expectation of treatment effect (21.3%) and pain worsening (13.3%).
Satisfaction with the current healthcare providers
In the physician group, the proportions of the respondents who were very satisfied, satisfied, somewhat satisfied, somewhat dissatisfied, dissatisfied and very dissatisfied with the physician were 5.6%, 23.7%, 48.2%, 17.3%, 4.0% and 1.2%, respectively. In the CAM group and those who concomitantly used CAM practitioner in the physician group (n = 2095), the corresponding proportions were 8.5%, 34.0%, 46.9%, 9.1%, 1.0% and 0.5%, respectively.
Factors associated with satisfaction with the current healthcare providers

CAM: complementary and alternative medicine, SE: standard error, OR: odds ratio, CI: confidence interval, ref: reference.
aReponses on satisfaction with the current healthcare provider were dichotomized to ‘satisfied’ (very satisfied, satisfied and somewhat satisfied) and ‘dissatisfied’ (somewhat dissatisfied, dissatisfied and very dissatisfied).
bThe pseudo R-squared value, likelihood ratio chi-square and the statistical degrees of freedom of this model were 0.52, 934.95 and 48, for physicians at hospitals/clinics, and 0.46, 534.99 and 35, for CAM practitioners, respectively.
cPhysician at hospitals/clinics also includes respondents who were consulting with physician and CAM practitioners, concurrently.
dCAM practitioners include also respondents who were consulting with physician and CAM practitioners, concurrently.
eOdds ratios were adjusted for sex, age, numerical rating scale, painDETECT, pain catastrophizing scale, annual household income, Short Form 8™ Health Survey scores (physical and mental components), types of treatment provided by physician (for physician group), types of physician's facility (for physicians group), average waiting time at the treatment facility and impression of treatment effect (Patient’s Global Impression of Change) provided by physicians and CAM practitioners. This model also includes the variables of visiting clinical department and types of CAM therapy (results shown in Supplementary Table S8), in addition to all the variables shown in this table.
fReference category is not visiting respective clinical department.
gReference category is not visiting respective type of CAM therapy.
Discussion
This study elucidated the care-seeking behaviours of the people living with chronic disabling musculoskeletal pain that interferes with their ADL/work and explored the factors behind the healthcare utilisation. It was found that while 24.5% and 18.3% consulted physicians and CAM practitioners, respectively, 57.2% did not consult either. Respondents with more intense pain visited either healthcare provider, and those with particularly severe conditions (higher NRS, PainDETECT, and PCS scores) and advanced age visited physicians. Those who visited CAM practitioners were younger and had a higher socio-economic status (more regular employees and higher annual income). The patients who did not consult either had overall less severe conditions, compared to those who consulted physicians and/or CAM practitioners.
The characteristics of healthcare users and reasons cited by them may implicate that need for relief from the severe pain compels people to visit any healthcare provider, weighing less on other factors such as financial burden of healthcare utilisation. People with particularly severe conditions, for example, those with higher pain intensity and the feature of pain likely attributing to the neuropathic component. Considering this trend with the most common cited reasons for selecting physician, that is, ‘expertise’ and ‘incapability of self-management’, respondents may have considered that physicians should provide specialised treatment with a high level of expertise to manage persistent pain that had gone beyond their capacity of self-management. This conclusion is reinforced by previous studies, in which the influence of socio-demographic factors varied, but pain-8,19,40,41 and disability-related factors8,19,41 were consistently identified as determining factors for care-seeking behaviour. Following historical trends of care-seeking and reasons for changes in the physician group in our research, about 30% had discontinued consultation with CAM practitioners previously because they were concerned over ‘cost’ and/or ‘treatment not being effective’, and switched to the professional help of physicians, setting their hopes on physicians’ ‘expertise’. Advanced age also differentiated the physician group from the others; particularly, the likelihood of visiting physicians based on odds ratio, increased five-fold in the age group of 70–79 years. This may be because elderly people may be less concerned over cost associated with physician visits than the younger generations, due to the Japanese public health insurance system, where co-payment rate for medical care cost accounts for 30% for 6–69 years old individuals, decreases to 20% for those aged 70–74 years, and further to 10% for 75 or older, at the time of the survey. From the greater proportion of those with PainDETECT of ≥19 and PCS of ≥ 30 among those who visited both physicians and CAM practitioners than the other groups, it was demonstrated that respondents with pain likely of neuropathic origin and pain catastrophizing visited physicians and CAM practitioners concurrently. For such patients, pain did not improve enough with the conventional treatment from their perspective and thus may have tried anything that could alleviate their pain.
The CAM group was characterized by a higher proportion of regular employees and patients with higher income than the other groups. In Japan, public health insurance does not cover all types of CAM therapies. Thus, those who can afford the cost for CAM therapies, that is, in this survey, respondents with middle income (4 million yen) or above, sought care from CAM practitioners. Full-time regular employees accounted for majority of CAM users. Time restriction for regular employees may set barriers to physician visits, whose reception hour coincides with their working hours. However, CAM may be more accessible to regular employees than medical institutions as CAM receptions tend to be open until later at night in Japan. Furthermore, before starting consultation with CAM practitioners, the majority of the people from the CAM practitioner group had discontinued physician visit (approximately 57%); the most common reason was ‘treatment not being effective’ (40.6%). Considering that more respondents were suffering from chronic pain for longer than 5 years, during a long course of search for pain relief, patients who were dissatisfied with suboptimal conventional treatment may have resorted to CAM therapies. Concerns regarding ‘long waiting time’ for physician visits was cited as the second most common reasons for switch from physician to CAM practitioner, which may underscore the importance of accessibility of time for those who utilised CAM services.
The overall trend in the factors characterized and associated with the untreated group was less severe condition than in the other two groups, consistent with the previous study. 42 However, it is important to note that a considerable number of respondents did not seek professional help despite severe conditions: about 60% of the untreated group had moderate or severe pain (NRS ≥ 5), some with likely involvement of neuropathic component (painDETECT ≥19), and their cognitive aspects were affected (PCS ≥ 30), and approximately 88% and 67% were with poor physical and mental HRQOL, respectively (SF-8 physical and mental components, respectively, <50). Based on the reasons cited for never visiting physicians despite their chronic disabling pain, approximately 23% of the untreated considered that they were successfully managing pain on their own (‘capability of self-management’), endorsed by the recent guidelines.43,44 However, in addition to the major concern regarding ‘cost’ (48.8% not consulting a physician and 53.2% not consulting a CAM practitioner), a lack of promising outlook for conventional medical treatment and CAM therapy effects (‘no expectation of treatment/therapy effect’) (25.2% and 20.9%) may affect cost-benefit balance, hindering them from starting to seek care. Among the untreated, majority had previously consulted with healthcare providers (40.9% physicians and 13.8% CAM practitioners) but had withdrawn from the visits ever since. Some of them withdrew the treatment or therapy because they successfully improved their pain (‘pain improvement’) (26.2% and 17.0% of those who withdrew from physician and CAM practitioner visit, respectively) and they saw no need for anymore visits. Meanwhile, pain aggravation (‘pain worsening’) was a key reason for treatment resumption of both physician and/or CAM practitioner visits after withdrawal. A possible common scenario drawn from these reasons for treatment/therapy withdrawal is the perceived disappointment with lack of treatment outcome by conventional treatment (‘treatment not being effective’) (35.9%) and concerns regarding ‘cost’ for continuing CAM therapy (38.2%) may have discouraged them from continuing consultation. To reach out to those suffering alone and facing barriers to initiate and continue healthcare utilisation, it is important to provide patients with appropriate diagnosis and treatment and to further raise awareness regarding available treatment options and their expected outcome in patients.
Our results regarding factors that affect patient satisfaction were consistent with previous reports, confirming the importance of communication and patient-centred care. Patient-centred care was reported to increase treatment satisfaction, 45 and promote adherence 46 and finding a common ground with the patient decreased a number of diagnostic tests and referrals. 47 Greater satisfaction in those who were convinced of the reasons for and expected outcome of recommended treatment may corroborate the importance of better patient-healthcare provider communication. A patient-centred care, that is, empathetic and attentive attitudes and better user–provider interactions that may empower patients to communicate their experience of their pain and to take control over their own treatment, may satisfy and encourage them to continue treatment/therapy.
A strong point of this study is that it includes a larger number of participants reflecting the demographic composition of the Japanese population, including those who do not use healthcare providers. However, this study has several limitations, and the results should be interpreted with caution. First, cross-sectional design precludes causal inference. Second, nature of online survey may warrant consideration. Recruiting via the pre-existing survey panel where a proportion of female elderly registrants are relatively small regardless of the effort to reflect the demographic composition of Japan may limit the representativeness of the survey respondents. Moreover, there may be a possibility of over-representing those with a greater motivation to participate. Third, for logistic regression analysis, all the relevant factors may not be covered, for example, outcome of the past care-seeking. Fourth, we developed three models, including the following numbers of independent variables: 14 (2–10 categories each) in the model for current healthcare utilisation, 16 (2–9 categories each) in the model for association between satisfaction with physicians, and 14 (2–6 categories each) in the model for the association between satisfaction with CAM practitioners. Nevertheless, as an explanatory analysis, no adjustment for multiple testing (multiplicity) was made. Interpretation of logistic regression analyses requires a consideration of this point. Fifth, responses on the past care-seeking behaviour may be subject to recall bias. Sixth, since we did not ask about the cause of pain in the main survey, we could not eliminate the confounding effect of pain comorbidities other than cancer and fractures (e.g. spinal cord injury, rheumatoid arthritis and fibromyalgia). There is a possibility that patients with nervous-related diseases may have preferred physicians, considering the result of the painDETECT. Seventh, since Japan is almost a homogenous nation ethnically, with public health insurance system, care must be taken when applying the results to other countries. Lastly, this survey is exclusively based on the respondents’ self-reports. Nevertheless, these self-reports may have allowed us to describe the care-seeking behaviours from the perspectives of people afflicted by chronic disabling musculoskeletal pain. In addition, online survey, conducted without the presence of the healthcare providers, may have elicited sincere perceptions of the respondents.
Conclusion
This internet survey revealed that among the people living with chronic disabling musculoskeletal pain, those with severe conditions consulted physicians for their expertise. Compared to respondents who consulted physicians, those with higher income, regular employees, who were considered too busy to visit physicians, and those with less severe conditions consulted CAM practitioners. Compared to the other groups, those with less severe conditions did not seek help, although greater than 60% had pain rated ≥5 on NRS. The majority of reasons for not visiting physicians nor CAM practitioners were financial.
Utilizing the results of this research is recommended, in order to develop better strategies for CMP treatment in the future. For example, in addition to developing more effective treatments, there seems to be a need to develop lower-cost treatments for those who have never visited treatment facilities. For those who visit physicians, treatment that emphasizes reducing the degree of pain by making the best use of their expertise may lead to improvement in satisfaction. In addition, the efforts to create environment to make it easier to visit to the treatment facilities may be effective to let patients visit physicians, for example, or flexible work arrangements at workplaces, online reservation system or telemedicine system at physicians to avoid long waiting time. At any treatment facilities, a patient-centred care, empathetic attitudes and better communication that allows patients to take control over their own pain management is recommended to improve patient satisfaction.
Supplemental Material
sj-pdf-1-osj-10.1177_23094990211044836 – Supplemental Material for Internet survey on factors associated with care-seeking behaviours of people with chronic musculoskeletal pain in Japan
Supplemental Material, sj-pdf-1-osj-10.1177_23094990211044836 for Internet survey on factors associated with care-seeking behaviours of people with chronic musculoskeletal pain in Japan by Keiko Sugai, Osahiko Tsuji, Shoko Takahashi, Morio Matsumoto, Masaya Nakamura and Nobuyuki Fujita in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
We thank Dr. Koichi Fujii, Takuma Sumikawa, Kazutaka Nozawa and Dr. Kanae Togo for helpful discussions and comments on the manuscript.
Author contributions
Keiko Sugai, Osahiko Tsuji, Morio Matsumoto, Masaya Nakamura, Shoko Takahashi, and Nobuyuki Fujita conceived the work, interpreted the data, and substantively revised the work. Shoko Takahashi designed the work. Keiko Sugai, Osahiko Tsuji, Nobuyuki Fujita, Shoko Takahashi analysed and interpreted the data. Shoko Takahashi drafted the work. Keiko Sugai, Osahiko Tsuji, Nobuyuki Fujita substantively revised the work. All the authors approved the submitted version and agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by Pfizer Japan, Inc. Support for statistics and medical writing/editing was provided by Takahiro Hirano and Emiko Sato at Clinical Study Support, Inc. and was funded by Pfizer Japan, Inc. ST is an employee of Pfizer Japan, Inc.
Data availability
The datasets generated during and/or analysed during the current study are not publicly available due to a contract between Keio University and Pfizer Japan, Inc., but are available to be provided privately on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.