
Abstract
Background:
Previous epidemiological surveys conducted in Japan highlighted problems with conventional approaches to treating chronic musculoskeletal pain. On the basis of prior studies, we initiated the “longitudinal investigation of chronic musculoskeletal pain” in 2010. In our first two reports, we revealed a high prevalence of chronic musculoskeletal pain, low satisfaction with treatment, and reduced quality of life. Those with severe and consistent low back pain had the highest risk of the persisting pain. The risk factors for developing chronic pain also included working in a professional, managerial, or clerical/specialist occupation, being female, having a body mass index ≥25, currently using alcohol or cigarettes, and having completed an educational level of vocational school or higher. As the final step of the epidemiological survey, the present study examined the effect of chronic musculoskeletal pain on a future decline in activities of daily living (ADL).
Methods:
A questionnaire was sent to individuals who participated in the research project in 2010. Follow-up research examining loss of basic or instrumental ADL, or certification of long-term care requirements, was conducted in 2013 (n = 4989 subjects).
Results:
The 3-year follow-up data revealed that chronic musculoskeletal pain was associated with a decline in ADL, even after adjusting for covariables such as age, sex, and smoking (adjusted odds ratio, 1.56; 95% confidential interval, 1.16–2.10).
Conclusions:
Chronic musculoskeletal pain is associated with future declines in ADL; therefore, relief of the chronic musculoskeletal pain may be important to maintain an active elderly population.
Keywords
Introduction
Chronic pain generally affects quality of life (QOL) and/or the ability to perform basic activities of daily living (ADL); thus, the social consequences of pain have received a lot more attention in recent years. 1,2 For example, research conducted in 2008 by the Institute of Medicine in America reported that approximately 100 million US adults had pain, with an approximate cost of $560–$635 billion per year. 3 The US government has taken these data seriously; indeed, a National Pain Strategy was conducted to deal with the problems associated with pain. 4 Research performed by the American Chamber of Commerce in Japan (ACCJ) in 2011 reported that the estimated economic losses due to pain were ¥37 million [approximately $340 thousand] a year, excluding costs of treatment. 1 Among different types of pain, the impact of chronic musculoskeletal pain has garnered much attention, principally because it is so prevalent. The National Livelihood Survey in Japan reported that low back pain, shoulder stiffness, and joint pain are the most common symptoms experienced by the Japanese general population. 5 Furthermore, in a large number of cases, musculoskeletal pain is expected to become chronic. Social and economic losses due to chronic musculoskeletal pain are thought to be huge; indeed, the Japanese government published a proposal in 2010 (a “Study Panel on Chronic Pain”) that proposed future measures for the management of chronic pain, and began to put such measures into practice. As a part of this initiative, we undertook a “longitudinal investigation of chronic musculoskeletal pain” in 2010, supported by the Ministry of Health, Labour, and Welfare. The results so far 6 –8 show that the prevalence of chronic musculoskeletal pain is 15.4%, and it is more common in females than in males. With regard to age, prevalence was highest in people aged 30–50 years. Pain was most commonly felt in the low back, neck, shoulders, and knees. Among symptomatic subjects, a high percentage of both men and women lost jobs, left school, were absent from work or school, or had to change jobs. When subjects with or without chronic musculoskeletal pain were compared in the areas of ADL and instrumental ADL (IADL), a decline of basic ADL was noted in men, and that of IADL was significant in women. In addition, the SF-36 QOL scores regarding mental and physical performance were significantly lower among the subjects with chronic pain, for both men and women, compared to those without the symptoms. These results from the cross-sectional analyses suggested that chronic musculoskeletal pain deprive one’s ability to do social and daily life activities, and impair physical and mental performance. 6 –8 Thus, chronic musculoskeletal pain is highly prevalent, resulting in a lower ADL and lower QOL. Previous studies reveal that musculoskeletal pain, especially low back pain, is the greatest cause of disability worldwide. 9,10 Another study shows that elderly people with pain at multiple sites are at an increased risk of developing disability. 11 However, these studies did not show whether chronic musculoskeletal pain results in a future decline of ADL or increased certification for Needed Long-Term Care in all age groups. If chronic musculoskeletal pain alone is a risk for developing disability, controlling chronic pain is an urgent priority, particularly in countries such as Japan, which has an aging society. Therefore, we conducted a longitudinal follow-up study to examine the association between chronic musculoskeletal pain and a future decline in ADL.
Methods
A baseline questionnaire-based survey was conducted in 2010 using the mail-based survey panel maintained by Nippon Research Center, Ltd. 11 In 2013, the questionnaire was again mailed to 6119 subjects who participated in the baseline (2010) survey. The questionnaire sent out in 2013 requested both basic information (age, sex, smoking habits, drinking habits, education, and marriage) and specific information about pain (presence of pain, site of pain, intensity of pain, frequency of pain, duration of pain, treatment history, and place of treatment), ADL (basic ADL [Katz ADL], IADL [Lawton’s score: males tested on a 5-point scale and females on an 8-point scale]), QOL (SF-36 scale), social loss (absence from, changes in, or quitting of work), and history of illnesses and need for care.
Of all 6119 subjects who received the questionnaire, 4989 subjects (81.5%) returned valid responses. Among 4989 subjects, 530 subjects met the definition of “decline in ADL (see below Outcome)” at the baseline survey and 4459 subjects (1909 males and 2550 females) did not show a decline in ADL at baseline.
Presence of chronic pain
The exposure variable was the presence or absence of chronic musculoskeletal pain at baseline. Chronic pain was defined as follows: (1) a symptom present within the past month that (2) has continued for at least 6 months, and (3) corresponds to a visual analog scale (VAS) of at least 5. 6 –8,12
Outcome
The outcome measure was a decline in ADL reported in 2013. A decline in ADL was noted when at least one of the following conditions was satisfied: Partially or fully dependent in terms of one or more activities (bathing, dressing, toileting, transferring, continence, and feeding) in the Katz basic ADL questionnaire
13
; Score <4 for males and <7 for females in the Lawton IADL questionnaire
14
; Official certification for Needed Long-Term Care or Needed Support. The present study considered any of the seven levels of long-term care insurance.
Covariates
Information obtained at the baseline survey included age, sex, smoking habits (currently smoking/quit smoking/nonsmoking), alcohol habits (currently drinking/quit drinking/nondrinking), education (high school or lower/college or higher), marriage (married/unmarried, bereaved, divorced), place of living, living circumstances (living together/alone), and annual family income (\5,990,000/\6,000,000[approximately $55,000]). Body mass index (BMI) was calculated by dividing the self-reported body weight by the square of the self-reported height (18.49/18.5–24.9/25.0 kg/m2). Information regarding a history of life-threatening diseases (stroke, myocardial infarction or angina, diabetes mellitus, femoral neck fracture, Parkinson’s disease, and cancer) was collected in the survey of 2013.
Statistical analysis
A 3-year longitudinal data analysis was conducted using data from 2010 as the baseline. The characteristics of the study subjects in terms of chronic pain were compared (t-test for continuous variables and the χ 2 test for categorical variables). The strength of the association between the presence of chronic pain and a decline in ADL (calculated by logistic regression analysis) was expressed in terms of the odds ratio (OR) and 95% confidence intervals (CI). First, a crude association was assessed. Second, calculations were adjusted for age (continuous variable) and sex. Third, the model was adjusted to include sex, smoking, alcohol intake, living circumstances, and BMI, as these variables were related to the outcome in univariate analysis (p < 0.1; multivariate-adjusted model 1). Fourth, the model was adjusted to include a history of life-threatening diseases, which were also related to outcome (multivariate-adjusted model 2).
To examine the impact of age, analysis was restricted to those aged 50 years or older or 60 years or older. Statistical analysis using multivariate-adjusted model 2 was then repeated. The subjects were also grouped according to the major site of pain, and statistical analysis was repeated using multivariate-adjusted model 2.
To assess potential selection bias, the data of study in 2010 were used. Among the participants of the study in 2010, 1770 subjects had chronic musculoskeletal pain in 2010. Of these, who also participated in the study in 2013 was defined as “participants (1149 subjects)”, and who did not participate in the study in 2013 was defined as “nonparticipants (621 subjects).” The severity of pain in 2010 between participants and nonparticipants were examined.
All analyses were performed using STATA ver. 13 (STATA, College Station, Texas, USA). The study was approved by the Institutional Review Board of Keio University School of Medicine. Additionally, all data were subjected to an unlinkable anonymization procedure.
Results
At baseline, 1012 out of 4459 subjects reported chronic musculoskeletal pain and 3447 did not (Table 1). Answers to questions requesting basic information revealed that the chronic pain was significantly more prevalent among subjects who were younger, were female, lived with others, had a BMI >25, or had a history of life-threatening diseases. The prevalence of chronic pain was also relatively higher among subjects who smoked and/or drank alcohol.
Characteristics of the study subjects according to the presence of chronic pain.

aDue to missing values, the totals for the stratified subgroups are not equal.
b t-Test was used for continuous variables and the χ2 test for categorical variables.
cStroke, myocardial infarction or angina, diabetes mellitus, femoral neck fracture, Parkinson disease, and cancer.
Of 4459, 11 subjects were missing on the outcome information, thus 4448 subjects were subject to the later analysis. During the 3-year follow-up, 273 subjects met one of the criteria for a decline in their ability to perform ADL. Among these, 26 showed a decline in basic ADL, 232 showed a decline in IADL, and 63 were officially certified as needing long-term care or support. (NB. There was some overlap between criteria.) When we examined the association between chronic pain and decline in ADL, we found that 77 subjects (7.6%) with chronic pain and 196 subjects (5.7%) without chronic pain met the criteria for ADL decline (Table 2). When the crude OR for those without chronic pain was used as the base (OR = 1.0), the crude OR for those with chronic pain was 1.36 (95% CI, 1.04–1.79). The OR from multivariate-adjusted model 1 remained statistically significant at 1.63 (95% CI, 1.22–2.17). Even after adjusting for a history of life-threatening diseases (model 2), statistical significance was maintained (Table 2). When the definition of ADL decline according to the Lawton questionnaire was changed to <3 for males and <6 for females, the adjusted OR (model 2) increased to 1.93 (95% CI, 1.21–3.07), though still retaining significance.
Association between chronic pain and decline in activities of daily living.

OR, odds ratio; CI, confidence interval.
aAdjusted for age, sex, smoking, alcohol drinking, living circumstances, and BMI category.
bFurther adjustment by a history of life-threatening diseases was carried out in addition to the variables included in model 1.
When subjects were grouped according to age (50 years and older and 60 years and older) the OR for the multivariate-adjusted OR (model 2) was 1.60 (95% CI, 1.13–2.27) and 1.48 (95% CI, 1.01–2.18; Figure 1). In addition, the multivariate-adjusted OR (model 2) by the major site of pain was as follows: the neck (OR, 1.15; 95% CI, 0.70–1.91), the shoulder (OR, 1.80; 95% CI, 0.93–3.46), the lower back (OR, 2.05; 95% CI, 1.29–3.24), and “other” (OR, 1.49; 95% CI, 0.87–2.56; Figure 1).

The association between chronic pain and a decline in activities of daily living. Adjusted odds ratios (95% confidence interval) after grouping subjects according to age and site of pain.
Finally, the severity of pain reported by subjects with chronic pain in 2010 (n = 1770) was cross-checked. Neither the intensity (VAS score) nor the frequency of pain was statistically different from that at baseline between the participants (1149) and nonparticipants (621) for the study in 2013 (Table 3).
Comparison of strength and frequency of pain (in 2010) for the participants and nonparticipants.
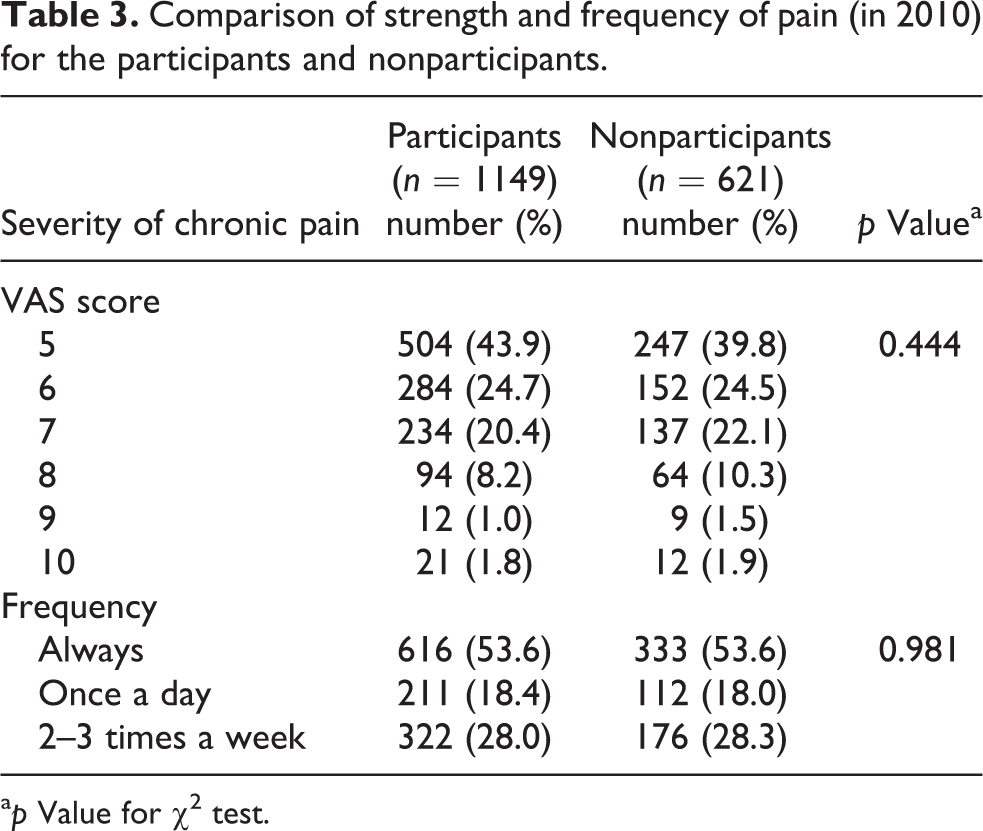
a p Value for χ2 test.
Discussion
The present longitudinal analysis combined data from 2010 and 2013 to assess whether chronic pain is linked to a decline in ADL. The results revealed that the OR for a decline in ADL over the 3-year period was 50% higher for those with chronic pain than for those without. Thus, preventing chronicity is important to ameliorate a future decline in ADL. Although OR adjusted according to the site of pain can be used only as a guide, we found that low back pain was most strongly associated with a decline in ADL (Figure 1). This information should be taken into account when prioritizing treatment or preventative measures.
This is the first longitudinal follow-up study to report a decline in ADL for subjects with chronic musculoskeletal pain across all age groups, although other cross-sectional studies report reduced ADL in pain sufferers, particularly in those with low back pain. 10,12,15 One study reported increased disability or a clinically meaningful decline in morbidity in those who have pain, but only in older community-dwelling adults. 11 Here, we show that individuals in all age groups are at high risk of a future decline in ADL. Thus, controlling musculoskeletal pain is vital for preventing such a decline in future.
We found that low back pain was most strongly associated with a decline in ADL. This may be because the low back occupies a central position, and stability and free movement are required for efficient movement of both the upper and lower extremities; therefore, pain in this area affects most ADL. Also, subjects with low back pain are likely to have a weak gluteus medius 16 or weakness of the muscles involved in trunk stability, which would also impair activity. However, chronic pain often occurs at multiple sites. 11 A complex network of factors underlies chronic musculoskeletal pain, including joint degeneration, neural pathways, 8,17 muscle weakness, 16 and psychosocial factors. 8,17,18 Accordingly, the mechanisms underlying a decline in ADL is also likely to be multifactorial. Pain can be very distracting, which in itself can also reduce mobility and functional independence. 11,19,20 Thus, a thorough assessment of each subject’s pain must be undertaken when considering appropriate measures to prevent the onset of disability.
This study has several limitations, and the results should be interpreted with a degree of caution. First, this study was based on answers to a follow-up mail survey. We mailed questionnaires to 6119 subjects who participated in the 2010 study and received valid responses from 4989 of them. The response rate (81.5%) was good. However, it may be that subjects with more severe symptoms were more likely to respond, leading to an overestimate of the OR. On the other hand, subjects who had a severe decline in ADL may be less likely to respond, leading to an underestimate of the OR. Nonetheless, selection bias did not cause the large difference between pain at baseline. Second, data regarding history of life-threatening diseases at baseline were lacking. Such “life-threatening” diseases may have been confounding factors as they could be responsible for a decline in ADL. However, adjustment for the presence of life-threatening diseases did not alter the OR significantly. Thus, the presence of life-threatening diseases at baseline is unlikely to have had a significant effect.
In conclusion, we found that chronic musculoskeletal pain leads to a decline in ADL over time, with an increased risk of future disability. Therefore, relief or prevention of chronic musculoskeletal pain, especially low back pain, might reduce the number of subjects requiring certification for long-term care and so should be actively considered. As previous researches have shown, management of chronic musculoskeletal pain is difficult. Even the conventional treatment at medical facilities has not shown a high degree of the satisfaction for the subjects with chronic musculoskeletal pain. 7,21 It is possible that the pain of the nonrespondents to the conventional treatment likely to become chronic, and we are at the urgent need to seek for another approach. Management of chronic musculoskeletal pain may be a key factor for supporting “active” aging, particularly in countries such as Japan, which have an aging society.
Footnotes
Acknowledgments
This study was carried out as a 2010 multidisciplinary research project for measures to help the handicapped (survey study of chronic musculoskeletal pain), supported by a Grant-in-Aid for Scientific Research from the Ministry of Health, Labour, and Welfare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.