
Abstract
Background:
Long-term consequences and the activities of daily living of bilateral lower limb amputation are not well documented.
Objectives:
The aims of our study were to identify the long-term effects of bilateral lower extremity amputations on daily activities and understand how these amputees cope with their mobility assistive devices.
Study design:
Cross-sectional study.
Methods:
A total of 291 veterans with war bilateral lower limb amputations accepted to participate in a cross-sectional study.
Results:
The average of follow-up was 25.4 years. A total of 152 amputees (54%) were involved in sports averagely 6.7 h per week. Bilateral amputees walk 10 m by the average of 15 ± 33 s, and they could walk continuously with their prosthesis 315 ± 295 m. They wore their prosthesis 6.8 ± 1.7 days per week and 7.9 ± 8.1 h per day. Of these, 6.7% of bilateral lower limb amputees needed help to wear their prosthesis; 88.3% of amputees used assistant device for walking. According to this survey, 73 (42%) prostheses in right limb were appropriate, 95 (54.6%) needed to be replaced, and 6 (3.4) needed to be fixed. On the left side, it was 76 (42%), 92 (52.0%), and 9 (5.1%), respectively. A total of 203 (74.9%) amputees reported limitations in at least one domain of the activities of daily living. The most common single item that affected the patients was ascending and descending stairs by the score of 66% of normal population.
Conclusion:
Veterans with bilateral lower limb amputations suffering from vast categories of daily problems.
Clinical relevance
This study and its results confirm that bilateral lower limb amputees have major progressive disabilities in daily activities and their social performance. This should attract the attention of amputees’ administrative organizations, social workers, health-care providers and caregiver providers.
Keywords
Background
The war between Iraq and Iran (1980–1988) was one of the longest wars of the previous century. As a result, according to the Organization of Veterans and Martyrs Affairs of Iran, there are currently 20,801 veterans with various levels of limb amputations, and among them 12,981 are lower limb amputees. War-related lower limb amputations are a different entity from those secondary to diabetic or vascular disease, as they occur more frequently in the healthy and younger male population.1–6 In addition, concurrent trauma to the head, neck, chest, extremities, and visceral organs may make the situation more complicated. 5
Twenty-five years after the end of the war, many veterans still have major problems secondary to their lower limb amputations. By identifying the major issues that bilateral lower limb amputees are facing during their daily activities, particularly during prosthetic usage, it is possible to improve their quality of life.
The aims of our study were to identify the long-term effects of bilateral lower extremity amputations on daily activities and understand how these amputees cope with their mobility assistive devices.
Methods
Out of 500 Iranians with war-related bilateral lower limb amputations that were registered in the Organization of Veterans and Martyrs Affairs of Iran, 291 were enrolled into our cross-sectional study. Inclusion criteria of the amputees were having bilateral primary or secondary lower extremity amputations, resulting from a single battlefield injury that happened during the Iraq–Iran war (1980–1988). The study was approved by the Research Committee of Mashhad University of Medical Science.
The research team consisted of three orthopedic surgeons, a physiatrist, and a prosthetist. The orthopedic surgeons supervised the study and evaluated the amputated limbs, focusing particularly on subjective and objective problems that were related to quality of life. Furthermore, the activities of daily living (ADL) and instrumental activities of daily living (IADL) forms were filled out under the supervision of the orthopedic surgeons. The physiatrist managed the follow-up protocol and identified the patient’s rehabilitation needs. The prosthetist evaluated the veterans’ prosthesis in terms of satisfaction or need to be repaired or replaced.
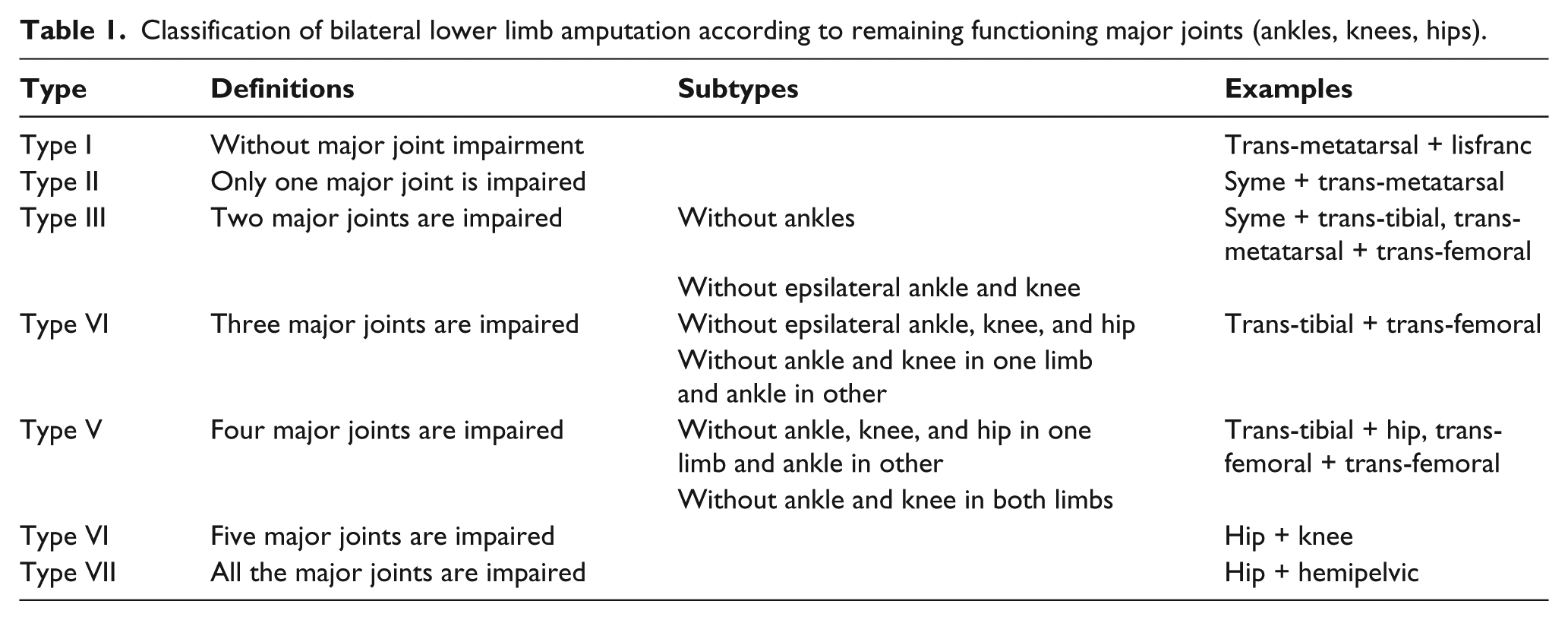
We classified the bilateral lower extremity amputees based on the remaining functioning major joints (ankles, knees, hips) in the lower extremities (Table 1). We believe that the functional major joints with active range of motion are essential for the amputee to be able to ambulate from one place to another. Furthermore, it is difficult to include all the different scenarios of bilateral amputations in a classification and have a reasonable and useful classification.
Classification of bilateral lower limb amputation according to remaining functioning major joints (ankles, knees, hips).
To evaluate the effect of amputation levels in both lower extremities, three different questionnaires were completed for each amputee.
Prosthesis Usage Questionnaire
The Prosthesis Usage Questionnaire focuses on evaluating the demographic features, prosthesis usage, kind of prosthesis used for ambulation, problems in wearing prosthesis, duration of prosthesis usage, gait problems, and prosthesis hygiene.
The ADL
The Barthel ADL score is a questionnaire that evaluates 10 important items for daily routine activities related to physical self-maintenance and basic mobility. 7
These items include eating, taking a bath, grooming, dressing, bowel continence, urine continence, toilet use, transfers (bed to chair and back), mobility (on level surfaces), and stair ascend and descend. Each item was considered as “independent,” “needs help,” or “dependent.”
According to the total score of all items, patients were categorized into two groups “without limitations” in the case of receiving a full total score (= 100%) and “with limitations” when the total score was below 100%.
IADL
The IADL score was developed by Lawton–Brody. 8 It evaluates the ability of a person to use instruments which are routinely used in daily living. This questionnaire consists of eight items that evaluate the ability to use the telephone, shopping, food preparation, housekeeping, laundry, traveling by car or public transportation, responsibility for own medications, and ability to handle finances. The scale has different scorings related to gender. As food preparation, housekeeping, and laundry items are not routine works for men in Iranian context, they are excluded for men. The average score ranges from 0 (completely dependent) to 8 (completely independent) for women and 0–5 for men. Domains of IADL show ability of adaptation to the environment and represent functional competence.
Finally, we used SPSS 17 software (SPSS Inc., Chicago, IL, USA) to analyze our results. Categorical and continuous variables were analyzed with Fisher’s exact test and chi-squared test, respectively. For analysis of continuous variables, we used independent samples t-test. The p value of less than 0.05 was deemed to be statistically significant.
Results
Demographic criteria
A total of 291 (58%) out of the 500 bilateral lower extremity amputees from the Iraq–Iran war, with an average age of 45 years (range: 37–89 years), participated in our study. Of these, 282 (97%) participants were male and 9 (3%) female. At the time of injury, the average age of the participants was 20 years (range: 14–65 years) and the average follow-up age was 25.4 years (range: 21–28 years). In all, 26% of the participants lost their jobs after being injured; however, according to a four-scale question, 77% of employed amputees rated their level of job satisfaction as complete or good.
Amputation evaluation
The most common type of amputation was type III (36%) followed by type IV (33%), but there was neither type I nor type VII in our study. The most common amputation level was the trans-tibial (48%). A total of 15 amputees (5.4%) had additional upper limb amputations. Eight of them were in the right upper extremity (four finger amputations, two trans-radial, one elbow disarticulation, and one trans-humeral) and seven in the left upper extremity (four finger amputations, two trans-radial, and one elbow disarticulation).
Physical status
A total of 152 amputees (54%) were involved in sports. The amputees exercised an average of 6.7 h per week (range: 15 min to 42 h). Bilateral amputees were able to walk 10 m in an average of 15 ± 33 s and could walk continuously 315 ± 295 m with their prosthesis (Table 2). Anterior bending (21%) and lumbar lordosis (16%) were the most common problems during gait assessment. Among the 226 amputees, 40.3% had a history of a serious fall during daily activities in the previous 3 months.
Prosthesis usage criteria for different bilateral amputation types.
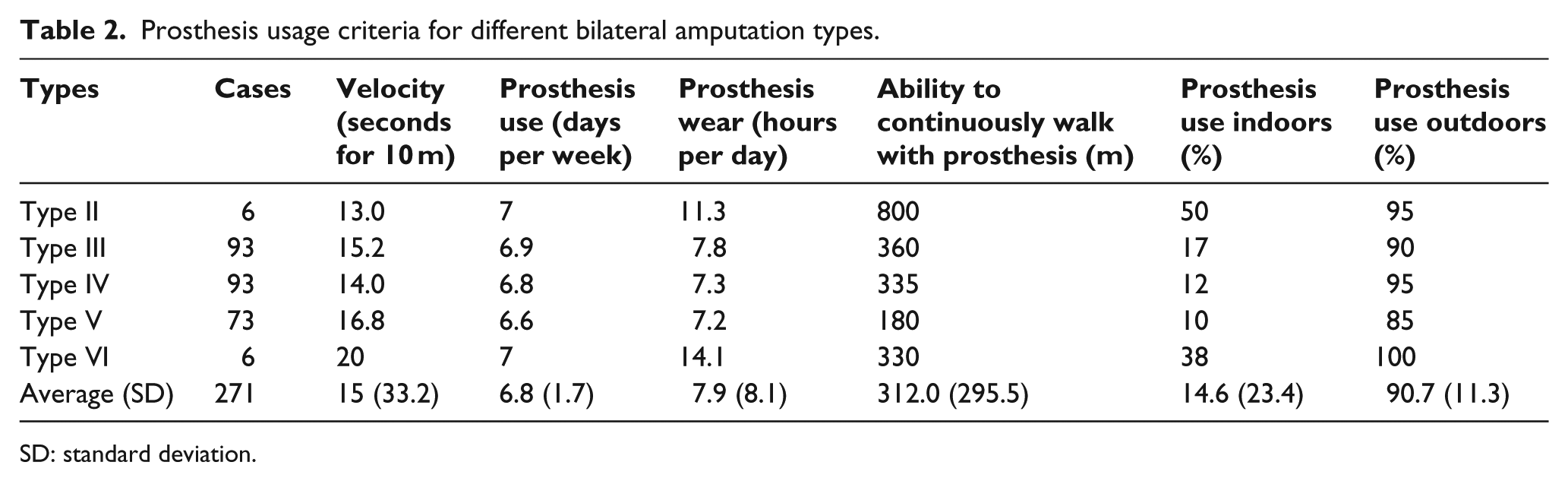
SD: standard deviation.
Prosthetic usage
Among the 291 patients who answered the Prosthetic Usage Questionnaire, 227 had prosthesis on the right side (78%) and 226 on the left (77.7%). A total of 198 veterans (72.8%) had bilateral prosthetic legs, 19 (6.5%) had one prosthetic leg, and 55 (18.9%) did not wear any prosthesis. Of these, 126 (51.6%) amputees were satisfied with their right prosthetic leg and 124 (50.6) with their left one. However, 70 amputees did not use their prosthesis and the reasons for not wearing the prosthesis were excessive weight (43%), prosthesis needs replacement (20%), prosthesis needs revision (13%), ulceration (7%), pain during prosthesis use (7%), skin problems (6%), dislike (1%), prosthesis needs repair (1%), or neuroma (1%). Moreover, the prostheses were worn 6.8 ± 1.7 days per week and 7.9 ± 8.1 h per day (Table 2).
Prosthesis usage problems
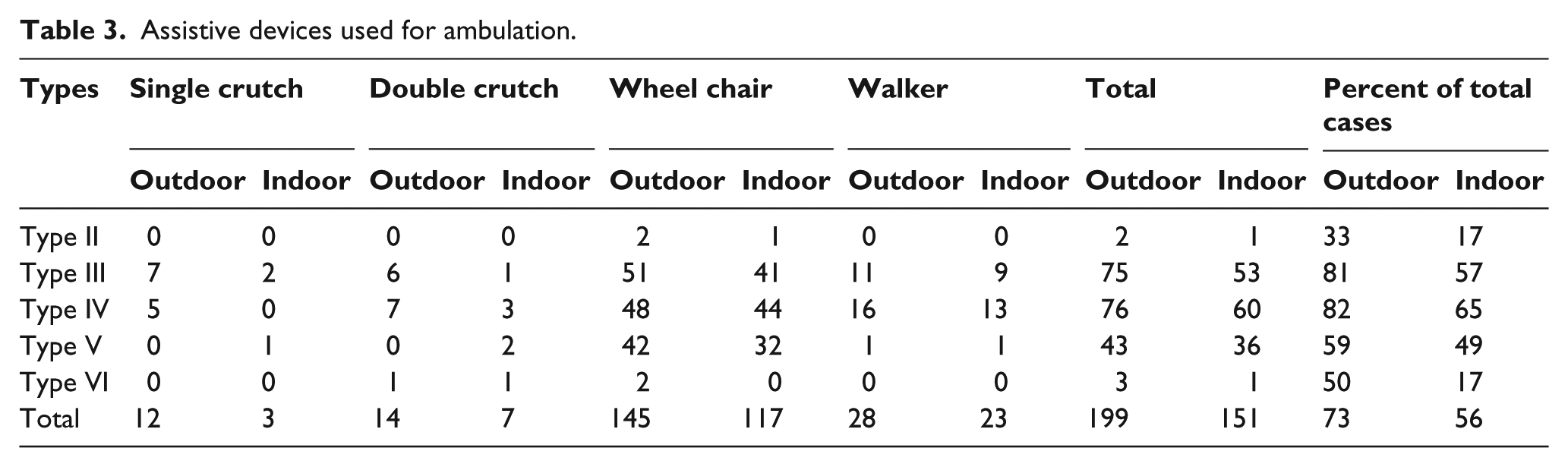
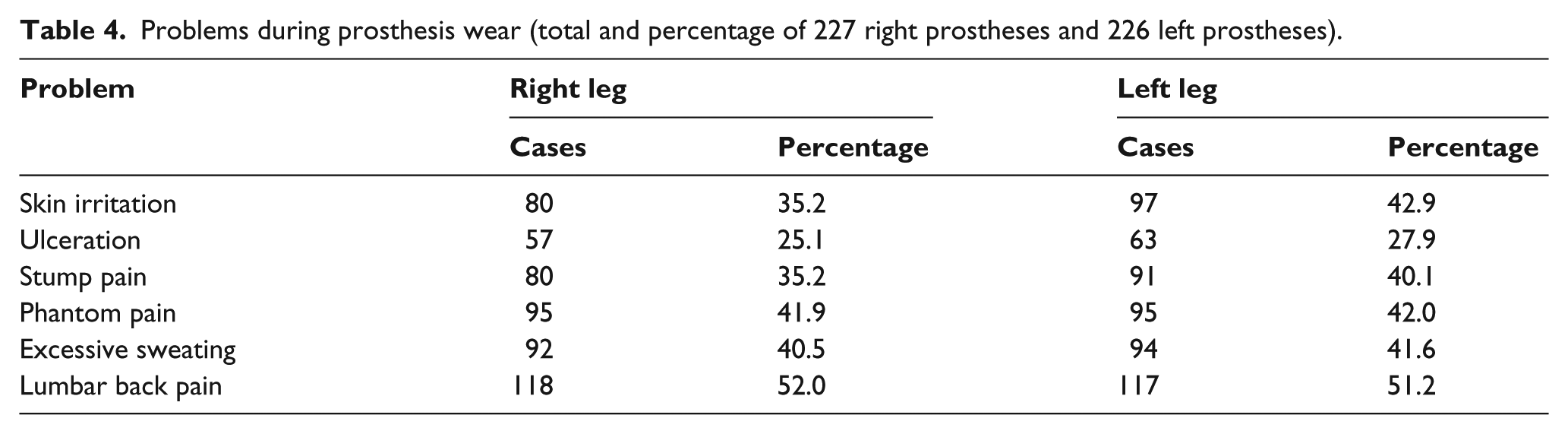
Regarding assistance to wear their prosthesis, 6.7% of bilateral lower limb amputees needed help, 88.3% used assistive devices for walking (84% for assistance and 16% instead of prosthesis). Prostheses were used 15% ± 23% indoors and 95% ± 11% outdoors (Table 2). The various kinds of assistive devices that were used in different types of amputations are demonstrated in Table 3. The major problems with prostheses were lumbar back pain (52%) and Phantom pain (42%). Table 4 shows the problems with prosthesis usage.
Assistive devices used for ambulation.
Problems during prosthesis wear (total and percentage of 227 right prostheses and 226 left prostheses).
Prosthetic hygiene
We evaluated the amputees’ concern about their stump, socket, and sock hygiene. The amputees washed their stumps, socks, and sockets by the averages of 0.9, 0.4, and 0.7 times per day, respectively.
Prosthesis evaluation
According to this survey, in the right prosthetic legs, 73 (42%) were appropriate, 95 (54.6%) needed to be replaced, and 6 (3.4%) needed to be fixed. In the left prosthetic legs, it was 76 (42%), 92 (52.0%), and 9 (5.1%), respectively.
ADL score
Of the 274 amputees who answered this questionnaire, 203 (74.9%) amputees reported limitations in at least one domain of the ADL. The most affected ADL was ascending and descending stairs which was 66% of the normal population’s score. Although, the score of this item decreased with amputation type, it was not statistically significant.
Table 5 shows the scores achieved in ADL dominants in different types of amputations. Except for type VI amputation, the total score decreased by severity of amputation level.
ADL score in different bilateral lower limb amputation types (independent amputees were those with a perfect score in each domain).
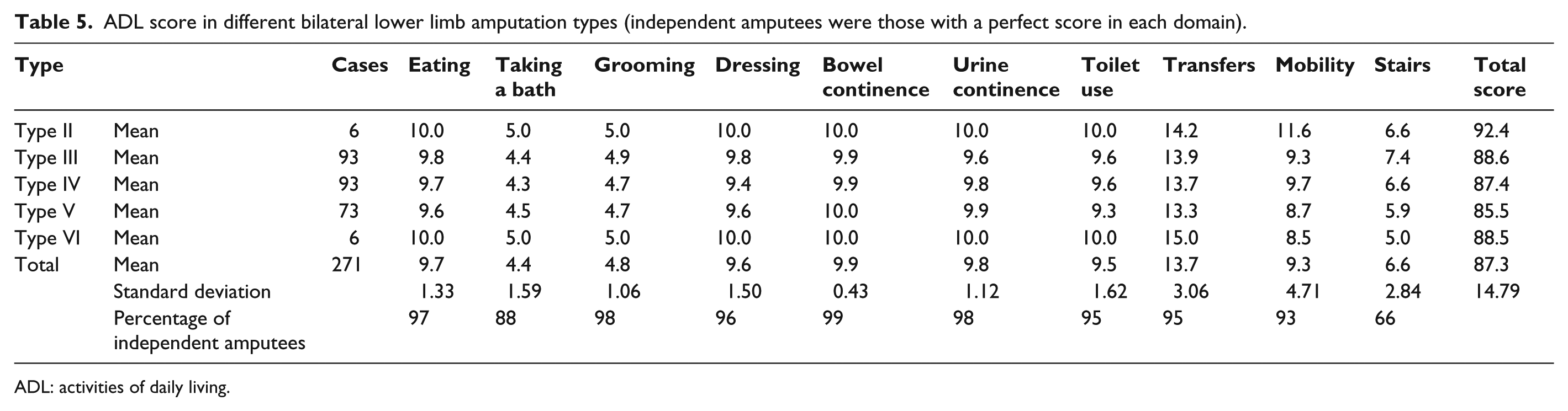
ADL: activities of daily living.
IADL score
In the 271 amputees, 179 (66.05%) had limitations in at least one domain of the IADL. The most commonly affected IADL was shopping, which was reported by 118 (44%) veterans followed by traveling in 30 (11%) as shown in Table 6.
Number and percentage of dependant bilateral lower extremity amputees according to IADL score in different domains.
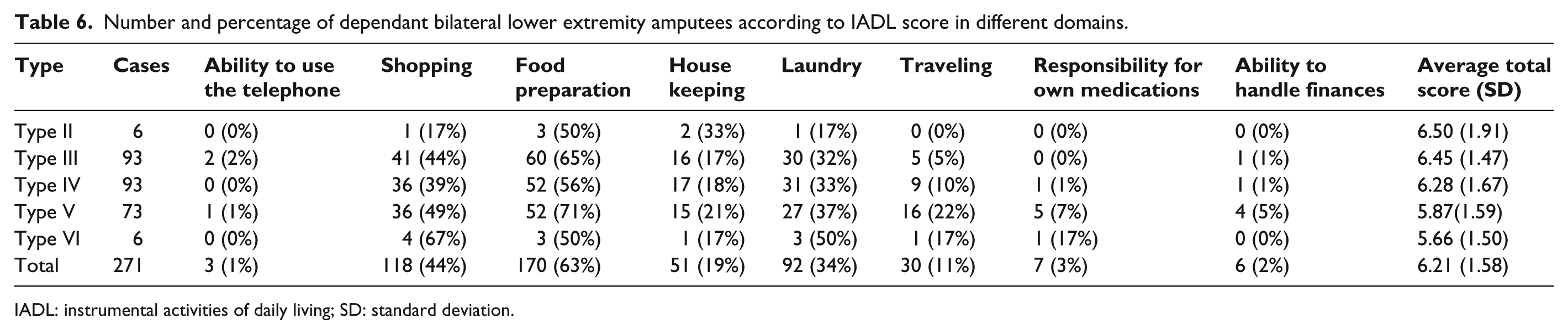
IADL: instrumental activities of daily living; SD: standard deviation.
The responsibility for own medication and laundry domains and total score decreased with severity of amputation level (Table 6), but the difference was not statistically significant.
Correlation between ADL and IADL
We calculated the correlation between the total scores of ADL and IADL. Spearman correlation coefficient of total scores of ADL and IADL amounted to r = 0.44 (p ≤0.001), showing a moderate correlation and significance.
Discussion
During a war, catastrophic human injuries and economic damages occur. The war injuries are not limited to battle time as many soldiers return with psychological or physical injuries, making their return to normal life very difficult. In this study, we evaluated the common problems which bilateral lower limb amputees engage in, especially in prosthesis usage and handling assistive devices that facilitate tasks needed for daily living.
The limitations of our study were that the number of veterans who agreed to participate in our study was only 291 amputees out of a total of 500 possible enrollees, but the number of participants was still more than other similar studies.6–17 Another limitation was that there was no type I or type VII amputation, although we tried to include all possible varieties of bilateral lower extremity amputations.
The average age of veterans at the time of injury was 20 years. Other studies done on Iraq–Iran war amputees reported the same age group (range: 18–25 years).11–14,17–19
In this study, the most common type of amputation was trans-tibial amputation. Other studies on bilateral lower extremity amputations have shown the same result.1,5,7,9,15,18–22 In all, 70% of the amputees had lost three or four out of six major joints, which shows the severity of their injuries.
Additionally, 5.4% of amputees had accompanied upper limb injuries which made the use of assistive devices such as walkers and wheelchairs even more difficult. More than half of the amputees were involved in sport activities, and this demonstrates that their amputation is not a limitation for sport activities. The outliers may be related to amputees involved in professional sport teams for the disabled. Walking velocity was inversely correlated with amputation level: higher amputation levels resulted in less walking. With the exception of participants with type VI amputation, who used a wheelchair for ambulation, with the increase in the type of amputation, continuous walking distance diminished (Table 2). At least one serious accident had happened for 40% of amputees in the last 3 months. The usage of assistive devices (crutch, walker, and wheelchair) and appropriate trainings could reduce such events.21,23
Only 78% of amputees used their prosthesis regularly, which is less than what was previously reported in unilateral amputees.11,13
The most common causes of prosthetic usage abandonment were lumbar back pain and skin irritation. In a survey done by Almassi et al. 18 in 2009, 56% of amputees reported skin complications with 71% of them having contact dermatitis. Moreover, the amputees considered stump and sock hygiene more important than the sockets. Perhaps considering socket hygiene as well could reduce the risk of skin complications.
A few amputees (6.7%) had difficulties donning and doffing their prosthesis on their own; however, most (88.3%) needed other assistive devices such as a crutch or wheelchair for ambulation. Prosthesis evaluations showed that a high number of prostheses needed revision or fixation (58%) and periodic examination of the prostheses could resolve such problems.
In our study, daily activities were evaluated with the Barthel index and Lawton–Brody scale. A high percentage of amputees had an above 90% ADL score. The most common problems were stair ascend and descend and taking baths. According to this result, modifications in the amputees’ environment to facilitate their transfer and bathing could be helpful. Although the stair ascend and descend score had a reverse relationship with amputation level, it was not statistically significant. In a study on war-related hip amputations, the stair domain had the lowest score, 17 and Roehrig et al. 24 reported similar low results as well. In another study, Ashraf et al. 20 evaluated 335 bilateral lower limb amputees using the Barthel index. They concluded that the amputees were mostly dependent during transfer and bathing. Paul et al. 21 in a study on bilateral lower limb amputees in India found no statistical difference in ADL scores between trans-femoral and trans-tibial amputations. But he found statistical difference in ADL scores between amputees who used their prosthesis and those who did not. In our study, except type VI amputation level, the ADL score decreased with increase in the amputation type.
Our study showed that the most dependency in the IADL score was in the shopping domain. A study performed on war-related hip amputations also expressed the same result. 17 As the level of amputation increases, the IADL index score decreases which will make the amputee more dependent.
Conclusion
Veterans with bilateral lower limb amputations suffer from a vast category of daily problems. Nearly all of them are male and young with long-term life expectancy rates. One-fourth lost their jobs, and this requires more attention to the socioeconomic conditions of amputees. Although most of the amputees lost more than half of their major joints in their lower extremities, they have a high tendency to be involved in sport activities; hence, facilities to provide appropriate equipment is essential. Since around 60% of prostheses need revision or replacing, periodic examination of stumps and prostheses and education for their care could prevent users from abandoning their prosthesis. Finally, we believe that the management of an amputated limb should start at the time of the amputation procedure and continue throughout the life of the amputee.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.