
Abstract
Objective:
This meta-analysis aimed to systematically compare the clinical outcomes of intramedullary nailing (IMN) fixation and percutaneous locked plating (PLP) fixation in the treatment of proximal tibial fractures.
Methods:
We searched PubMed, Embase, Cochrane library, China National Knowledge Infrastructure (CNKI), China Science and Technology Journal Database (VIP), and Wan Fang to select relevant articles up to March 29, 2020 without language limit. Continuous variables were estimated by weighted mean difference (WMD) with a 95% confidence interval (CI) and dichotomous outcomes were calculated by relative risk (RR) with 95% CI. Moreover, heterogeneity analysis was evaluated. Furthermore, publication bias assessment and sensitivity analysis were conducted. Stata 11.0 software was used to perform the statistical analysis.
Results:
Ten studies involving 667 cases (321 from IMN fixation group and 346 from PLP fixation group) were included. The type of fractures involved in the included articles was extra-articular proximal tibia fractures. IMN fixation method achieved significantly shorter union time (WMD = −2.88, 95% CI: −3.23 to −2.53, p < 0.001) and full weight-bearing time (WMD = −2.81, 95% CI: −3.64 to −1.97, p < 0.001) than PLP fixation method. Meanwhile, IMN fixation resulted in lower risks of infection (RR = 0.50, 95% CI: 0.27 to 0.91, p = 0.02) and total complications (RR = 0.36, 95% CI: 0.22 to 0.60, p < 0.001) than PLP fixation. No significant differences were found in the incidence of nonunion (p = 0.33), malunion (p = 0.38), and osteofascial compartment syndrome (OCS, p = 0.62) between the two groups.
Conclusions:
Compared to PLP fixation, IMN fixation had several advantages in treating proximal tibial fractures, including the short time of union and full weight-bearing, as well as a low risk of infection and total complications.
Introduction
Tibial fractures are one of the most common types of long bone fractures 1 and extra-articular proximal tibia fractures account for approximately 5–11% of all tibial fractures. In order to maintain anatomical reduction and prevent destructive complications, surgical approaches are usually required for treatment. 2 However, the tibia is less covered by soft tissue, and fractures in this part are often accompanied by soft tissue injury. Meanwhile, the proximal tibia is highly susceptible to soft-tissue damage, and its posterior cortex is closely associated with the posterior tibial blood vessels, thus the incidence of arterial injury related to displaced fractures is high, which increases the challenge of treatment. 3 It is reported that nailing is considered the gold standard surgical method for tibial shaft fractures. 4 Nevertheless, complication of treatment and associated injures with extra-articular proximal tibia fractures have led to several approaches and fixation modes, so there is little consensus on optimal management. Thus, it is necessary to explore the appropriate treatment strategy.
During the operation, in order to maintain the stability of tibial shaft fracture fixation, various treatment modalities have been developed. Among these, percutaneous locked plating (PLP) and intramedullary nail (IMN) are two most frequently used surgical fixation methods for the treatment of extra-articular proximal tibial fractures. 5,6 In clinical application, proximal tibial fractures treated with IMN fixation sometimes require additional surgical techniques, such as percutaneous anterior plate assisted fracture reduction, which could be left or removed after IMN fixation. As two different fixation methods, each has its advantages. In brief, the PLP fixation method provides stable fixation and good functional results for proximal tibial fractures with a low complication rate. 7 The IMN fixation method involves minimal surgical dissection and can maintain blood supply without destroying the soft tissue surrounding the fracture. This soft-tissue preserving fracture fixation method uses a load-sharing device to achieve biomechanical stability of the fracture, allowing patients to weight-bear early after surgery. 8 Nevertheless, these two fixation methods may lead to certain complications. For example, IMN fixation may cause malunion of the fracture site and anterior knee pain. 9 In addition, the incisions of PLP fixation are longer than that of IMN, which may cause postoperative infection, wound complications, and implant prominence. 10,11
Although several studies have compared the clinical outcomes of IMN fixation and PLP fixation for extra-articular proximal tibial fractures, 12 –15 the results are conflicting. For example, several articles reported that IMN fixation had shorter fracture healing time and fewer complications than PLP fixation. 12,15 Conversely, other studies suggested that there was no significant difference in clinical efficacy between IMN and PLP fixations in the treatment of extra-articular and metaphyseal proximal tibial fractures. 13,16 Moreover, whether there are differences in the incidence of nonunion, malunion, osteofascial compartment syndrome (OCS), and total complications between these two different fixation methods are not completely clear. Therefore, we performed a comprehensive meta-analysis to compare the clinical efficacy of IMN fixation and PLP fixation in the treatment of proximal tibial fractures.
Methods
Retrieval strategy
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 Relevant literature was searched on PubMed, Embase, the Cochrane Library, China National Knowledge Infrastructure (CNKI), WanFang, and China Science and Technology Journal Database (VIP) up to March 29, 2020. The keywords used for searching included “tibial plateau fracture,” “proximal tibia fracture,” “IMN,” “plate,” and “plating.” Supplementary Table 1 shows the specific search step of PubMed. In addition, the authors also manually searched paper version of literature and screened the reference lists of relevant reviews as well as included studies to obtain more eligible studies. There were no limitations in language.
Inclusion and exclusion criteria
Studies meeting the following criteria were included: (1) the study subjects were patients diagnosed with proximal tibial fracture; (2) studies that compared the outcomes of IMN fixation vs. PLP fixation in patients with proximal tibial fracture; (3) studies reported at least one of the following research outcomes: union time, full weight-bearing time, nonunion, malunion, infection, OCS, and total complications; and (4) the type of study was not limited.
Studies meeting the following criteria were excluded: (1) studies did not record data on proximal tibial fractures; (2) the type of studies was review, letter, and comment; and (3) data were duplicate or incomplete.
Data extraction and outcome measure
Two reviewers independently collected the following data from each included studies: name of the first author, year of publication, the location of research, the characteristics of participants [age, sex, and body mass index (BMI)], sample size, and outcome measures.
The primary outcome was union time. Secondary outcomes included full weight-bearing time, nonunion, malunion, OCS, infection, and total complications.
Quality of studies assessment
Quality of the included studies was independently evaluated by two reviewers following the guidelines of the Cochrane Handbook for Systematic Review of Interventions. 18 Inconsistencies during data extraction and quality assessment were resolved by discussing with a third reviewer.
Statistical analysis
All the statistical analyses were conducted using Stata 11.0 software (Stata Corp LP, College Station, TX, USA). Continuous outcomes (union time and full weight-bearing time) were merged by weighted mean difference (WMD) with 95% confidence interval (CI), while the dichotomous outcomes (nonunion, malunion, OCS, infection, and total complications) were presented as relative risk (RR) with 95% CI. Cochran’s Q test and I 2 test were used to evaluate the heterogeneity. 19 p < 0.05 and I 2 > 50% indicating significant heterogeneity and the random effect model was used; otherwise, a fixed effect model was adopted. Furthermore, publication bias was evaluated by Egger’s test. Meanwhile, sensitivity analysis was conducted to assess the stability and reliability of results. p < 0.05 was considered statistically significant.
Results
Literature selection
The processes for literature search are shown in Figure 1. Initially, 446 articles were identified as potentially relevant studies. Among these, 79 duplicate articles were excluded. By scanning the titles and abstracts, 150 articles were removed according to the inclusion criteria. Then, seven articles were eliminated after reading the full text. Finally, 10 articles 12 –16,20 –24 fulfilled the selection criteria were included in this meta-analysis.

Flowchart of study selection and inclusion.
Characteristics of the included studies
Table 1 summarized the characteristics of included studies. These studies were published from 2009 to 2019 and conducted in USA, India, and China. The sample size of included studies ranged from 38 to 108, and a total of 667 participants (321 in IMN fixation group and 346 in PLP fixation group) were enrolled. The fracture type reported in the included studies was extra-articular proximal tibia fractures. There was no significant difference in sex, age, BMI, and AO classification between the IMN fixation and PLP fixation groups. However, the follow-up time of each study was significantly different. Among the studies, six studies reported the union time 12,16,20,21,23,24 ; four studies involved full weight-bearing time 12,14,21,23 ; four studies presented nonunion 12 –14,16 ; six studies reported malunion 12 –14,21 –23 ; eight studies compared infections 12 –16,21 –23 ; two studies reported OCS 12,23 ; and six studies reported total complications. 12,15,16,21 –23
Characteristics of 10 included studies in this meta-analysis.

F, female; NR, not reported; RCT, randomized controlled trial; IMN, intramedullary nail; PLP, percutaneous locked plating; K-wires, Kirschner wires.
a, Union time; b, Full weight-bearing Time; c, Nonunion, d, Malunion; e, Infection; f, Osteofascial compartment syndrome; g, Total complications.
Risk of bias assessment
Details of the risk of bias of included studies are displayed in Figure 2. There was low risk of attrition bias and reporting bias, while the performance bias of all studies was unclear. Only one study 14 reported the blinding of outcome assessment. Three articles 12,13,16 had a high risk of selection bias. Overall, there was high methodological bias of the included studies.

Quality assessment of the studies included in this meta-analysis. A: Risk of bias graph; B: Risk of bias summary. Plus sign, low risk; question mark, unclear risk; minus sign, high risk.
Meta-analysis results
Primary outcomes: Union time
No evidence of heterogeneity was observed (I 2 = 47%, p = 0.09), thus the fixed effect model was used for the analysis of the primary outcome. The results indicated that IMN fixation achieved shorter union time than PLP fixation (WMD = −2.88, 95% CI: −3.23 to −2.53, p < 0.001, Figure 3A).
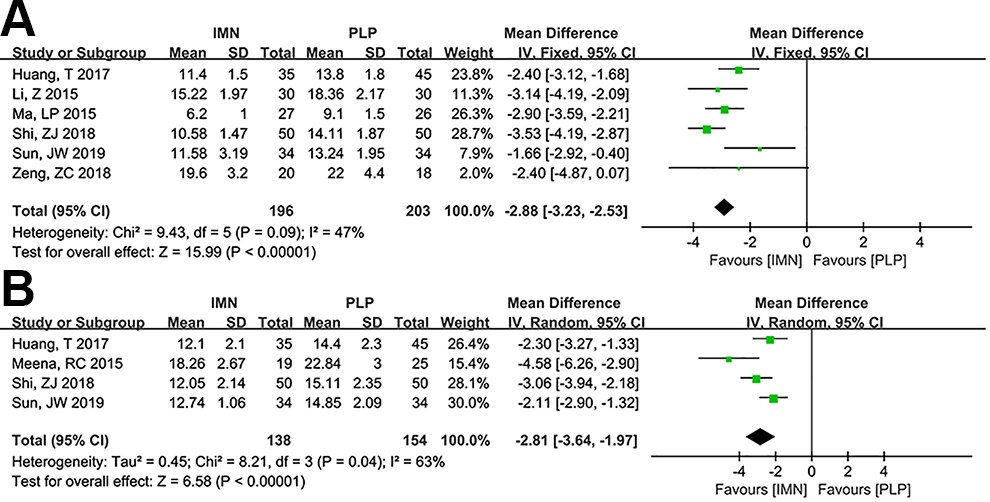
Comparison of union time (A) and full weight-bearing time (B) between IMN fixation and PLP fixation groups.
Secondary outcomes: Full weight-bearing time
Full weight-bearing time was reported in four studies. We observed that IMN fixation had shorter full weight-bearing time compared with PLP fixation (WMD = −2.81, 95% CI: −3.64 to −1.97, p < 0.001, Figure 3B), with significant heterogeneity (I 2 = 63%, p = 0.04).
Nonunion
Four studies reported the incidence of nonunion. The meta-analysis indicated no statistically significant difference in nonunion between the IMN fixation and the PLP fixation (RR = 1.76, 95% CI: 0.56 to 5.57, p = 0.33, Figure 4A), with no significant heterogeneity (p = 0.27, I 2 = 23%).

Comparison of nonunion (A), malunion (B), and OCS (C) between IMN fixation and PLP fixation groups.
Malunion
The incidence of malunion was reported in six studies. No significant heterogeneity was noted among these studies (p = 0.32, I 2 = 15%). The analysis revealed no significant difference between the two groups (RR = 1.32, 95% CI: 0.71 to 2.44, p = 0.38, Figure 4B).
OCS
There were two studies compared the differences in OCS. Figure 4C reported the results of OCS with fixed-effect model (I 2 = 0%, p = 0.54), and no significant difference was observed in IMN fixation compared with PLP fixation (RR = 1.46, 95% CI: 0.33 to 6.46, p = 0.62).
Infection
Eight studies reported the differences in infection. The results indicated that IMN fixation had significantly lower infection rate (RR = 0.50, 95% CI: 0.27 to 0.91, p = 0.02, Figure 5A) than PLP fixation, with no significant heterogeneity (I 2 = 0%, p = 0.85).

Comparison of infection (A) and total complications (B) between IMN fixation and PLP fixation groups.
Incidence of total complications
The incidence of total complications was obtained from six studies, and fixed-effect model was selected to merge the results (I 2 = 0%, p = 0.89). The results demonstrated that IMN fixation had a significantly lower incidence of total complications than PLP fixation (RR = 0.36, 95% CI: 0.22 to 0.60, p < 0.001, Figure 5B).
Publication bias assessment and Sensitivity analysis
We used Egger’s test to assess the potential publication bias in this study. Results showed that no significant publication bias was detected in all indicators except infection (egger test, p = 0.041), suggesting that the corresponding results were stable and credible. In addition, sensitivity analysis was performed to determine the effect of each significant difference index (infection, total complication, union time, and full weight-bearing time) on the pooled results. The results revealed that the combined results of total complication, union time, and full weight-bearing time were stable (p < 0.05). However, the results of infection were reversed by removing the study of Zhang et al. 15 (p = 0.101).
Discussion
Proximal tibial fracture, most commonly caused by high-energy injuries, is related to the complex comminution of displaced fracture fragments. 25 In general, there is still controversy regarding the treatment of complex proximal tibial fractures, and there is no clear gold standard between IMN and PLP fixation methods. This meta-analysis showed that in the treatment of proximal tibial fracture, IMN fixation method had a shorter union time, shorter full weight-bearing time, lower risks of infection, and fewer total complications than PLP fixation method. However, no significant differences were found in nonunion, malunion, and OCS between the two groups. To the best of our knowledge, this meta-analysis was the first to compare the efficacy and complication of IMN and PLP for proximal tibial fractures treatment.
At the time of healing, IMN fixation exhibited superior mechanical properties, thereby increasing stability compared to PLP fixation. Therefore, IMN fixation method might be more conducive to bone healing in treating human tibial fractures. 26 Meanwhile, Laigle et al. 27 indicated that the advantages of IMN fixation method were early resumption of weight-bearing and reduced the burden on patients with tibial shaft fracture. Our results were consistent with the above studies that the patients in the IMN group recovered faster than those in the PLP group. Similarly, Meena et al. 14 found that the IMN group had a significantly shorter average hospital stay (4.1 days vs. 5.3 days) and time to fracture union (18.26 weeks vs. 22.84 weeks) than PLP group, which further supported our results. In another study looking at fixation type, Morwood et al. 28 observed that patients with IMN fixation had faster time to full weight-bearing than those treated with plate fixation, which was consistent with our finding. Specially, early weight-bearing facilitated the rapid dynamisation of fracture fragments and promoted the formation of good periosteal callus, 29 which might be the reason for the rapid recovery of IMN fixation method. Therefore, postoperative functional exercise should be encouraged as early as possible to promote the recovery of limb function, thereby shortening the time of full weight-bearing. As for the PLP fixation method, higher stress on the locking plate could result in stress shielding of the fracture bones, which would delay healing due to the lack of mechanical stimulation. 30 In addition, plates were not routinely removed and require greater exposure and might affect periosteal blood supply. 31 Taken together, these factors were probably not conducive to the rapid healing of the fracture site.
Furthermore, we observed that IMN fixation resulted in fewer infection and total complications than PLP fixation. Previous studies indicated that IMN fixation method could effectively prevent bone shortening, rotational displacement, as well as significantly reduce a series of complications such as joint stiffness. 22 Meanwhile, the size of incision in the IMN fixation and the area of the incision exposed to air were relatively small, which was less likely to be infected than the long incision of the PLP fixation method. 32 Although the PLP fixation was easy to operate and complete reduction, it required extensive exposure of the fracture site, which might severely damage the blood circulation at the fracture end and increase the risk of infection. 33 However, there were no differences between two treatments in nonunion, malunion, and OCS. These findings should be confirmed by using more high-quality studies.
Several limitations should be noted in this meta-analysis. (1) Only 10 studies were included, and the sample size of each study was relatively small. (2) Subgroup analysis was not performed due to some incomplete information (such as AO classification), so we could not clarify the source of heterogeneity. (3) Three included studies 12,13,16 were not randomized controlled trials, which might affect the results. (4) The follow-up time varied greatly among the included studies and it might affect the results of heterogeneity and lead to publication bias. (5) The combined results of infection were unstable, and larger sample studies needed to be included to verify our findings. (6) Fracture type is relatively single. The fracture types reported in the included literature were all extra-articular proximal tibial fractures without intra-articular fractures. (7) In fact, in clinical application, proximal tibial fractures treated with IMN fixation sometimes require additional surgical techniques, such as plate assisted fracture reduction, that can be left or removed after IMN fixation. However, our meta-analysis only focused on the impact of a single fixation method on the outcome of proximal tibial fractures, without considering the combination of these two techniques. Thus, it is necessary to refer to the latest clinical technology and incorporate surgical details to compare fixation methods in future studies. Ultimately, a prospective, randomized, clinical trial evaluating these parameters will help more accurately define the advantages and disadvantages of each technique.
Despite the shortcomings in this study, our research still has certain clinical reference value. Notably, most of the outcome indicators had no significant heterogeneity. In addition, publication bias assessment and sensitivity analysis showed that our results were stable and reliable.
Conclusion
Compared with PLP fixation method, IMN fixation had shorter union time, shorter full weight-bearing time, lower risks of infection, and fewer total complications. However, no differences between two treatments were observed in nonunion, malunion, and OCS. Thus, more high-quality randomized controlled trials are required to verify our findings.
Supplemental material
Supplemental Material, sj-pdf-1-osj-10.1177_23094990211024395 - Comparison of intramedullary nailing fixation and percutaneous locked plating fixation for the treatment of proximal tibial fractures: A meta-analysis
Supplemental Material, sj-pdf-1-osj-10.1177_23094990211024395 for Comparison of intramedullary nailing fixation and percutaneous locked plating fixation for the treatment of proximal tibial fractures: A meta-analysis by Cheng Ren, Ming Li, Liang Sun, Zhong Li, Yibo Xu, Yao Lu, Qian Wang, Teng Ma, Hanzhong Xue and Kun Zhang in Journal of Orthopaedic Surgery
Footnotes
Abbreviations
Author contributions
Zhong Li carried out the Conception and design of the research, Cheng Ren, Ming Li participated in the Acquisition of data. Cheng Ren, Liang Sun carried out the Analysis and interpretation of data. Yao Lu, Liang Sun and Yibo Xu participated in the design of the study and performed the statistical analysis. Zhong Li, Qian Wang and Teng Ma participated in Obtaining funding. Cheng Ren drafted the manuscript and Kun Zhang, Hanzhong Xue, carried out revision of manuscript for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Key Social Development Projects of Shaanxi Science and Technology Administration (grant number 2015SF116, 2015SF110 and 2016SF340).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.